Journal of Peking University (Health Sciences) ›› 2025, Vol. 57 ›› Issue (3): 496-506. doi: 10.19723/j.issn.1671-167X.2025.03.013
Previous Articles Next Articles
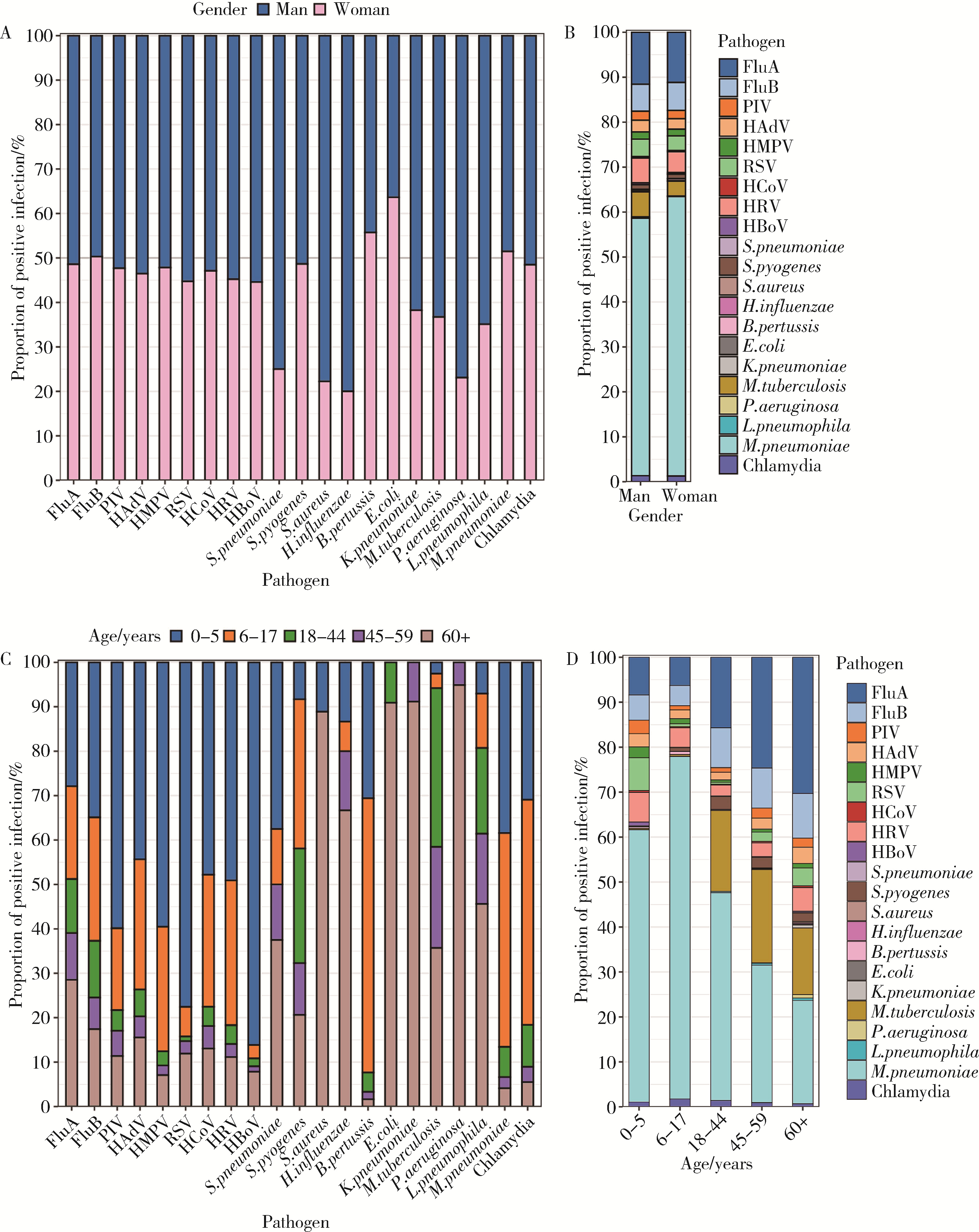
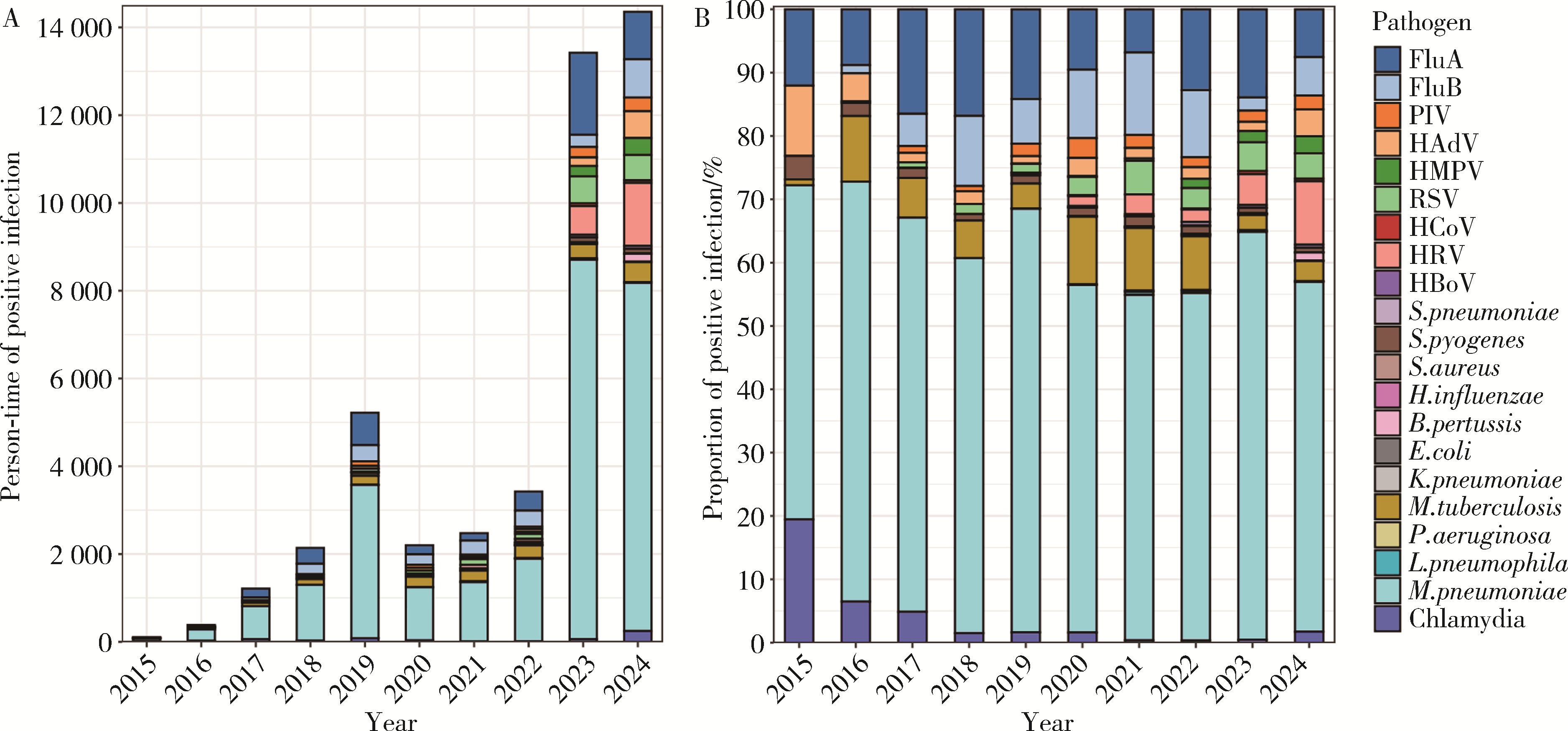
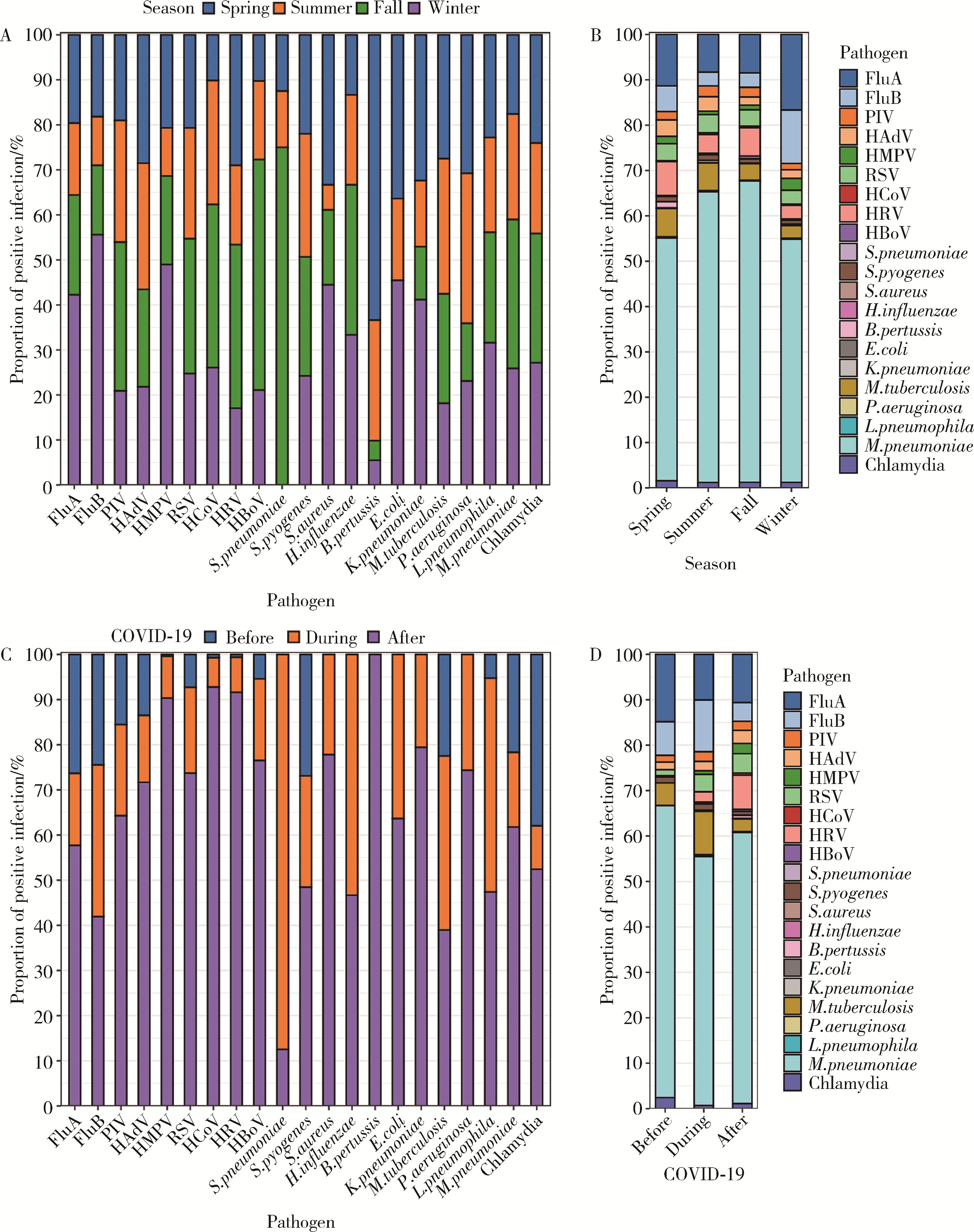
Distribution of respiratory pathogens in patients with pneumonia in Yinzhou, Ningbo, 2015-2024
Ziming YANG1,2, Shuya LI1,2, Xiaotong LI1,2, Peng SHEN3, Yexiang SUN3, Hongbo LIN3, Zhiqin JIANG3, Siyan ZHAN1,2,4,5,*( ), Zhike LIU1,2,*()
), Zhike LIU1,2,*()
- 1. Department of Epidemiology and Biostatistics, Peking University School of Public Health, Beijing 100191, China
2. Key Laboratory of Epidemiology of Major Diseases (Peking University), Ministry of Education, Beijing 100191, China
3. Yinzhou District Center for Disease Control and Prevention of Ningbo, Ningbo 315199, Zhejiang, China
4. Research Center of Clinical Epidemiology, Peking University Third Hospital, Beijing 100191, China
5. Center for Intelligent Public Health, Institute for Artificial Intelligence, Peking University, Beijing 100871, China
CLC Number:
- R184


| 1 |
doi: 10.1016/S1473-3099(24)00176-2 |
| 2 |
邹林, 高翔, 张冲, 等. 2020—2022年北京市通州区呼吸道感染患者呼吸道病原体流行特征分析[J]. 疾病监测, 2023, 38 (7): 799- 805.
|
| 3 |
杨霖昀, 唐国英, 郑小萍, 等. 2019—2022年重庆开州区儿童呼吸道感染病原体流行特征[J]. 公共卫生与预防医学, 2024, 35 (3): 137- 140.
|
| 4 |
杨雪, 吴重阳, 熊丽, 等. 非药物干预措施对成人感染呼吸道病原体流行特征的影响[J]. 国际检验医学杂志, 2024, 45 (12): 1425- 1430.
|
| 5 |
doi: 10.1080/21645515.2022.2115751 |
| 6 |
严梦瑶. 苏州地区住院儿童下呼吸道感染病原学流行特征以及与气候因素、大气污染物相关性研究[D]. 苏州: 苏州大学, 2022.
|
| 7 |
国家卫生健康委员会. 2020年第1号[EB/OL]. (2020-01-20) [2025-01-01]. http://www.nhc.gov.cn/xcs/zhengcwj/202001/44a3b8245e8049d2837a4f27529cd386.shtml.
|
| 8 |
国家卫生健康委员会. 2022年第7号[EB/OL]. (2022-12-26) [2025-01-01]. http://www.nhc.gov.cn/xcs/zhengcwj/202212/6630916374874368b9fea6c2253289e1.shtml.
|
| 9 |
张静, 王蕊, 任心慈, 等. "提高抗菌药物治疗前病原学送检率"专项行动三年改进效果追踪评价[J]. 中国感染控制杂志, 2024, 23 (11): 1430- 1437.
|
| 10 |
褚衍茹, 雷松, 劳旭影, 等. 2023—2024年宁波市冬春季急性呼吸道感染病例多病原流行特征分析[J]. 现代实用医学, 2024, 36 (9): 1162- 1165.
|
| 11 |
国家呼吸系统疾病临床医学研究中心, 国家儿童医学中心, 中华医学会儿科学分会呼吸学组, 等. 中国儿童肺炎链球菌性疾病诊断、治疗和预防专家共识[J]. 中华实用儿科临床杂志, 2020, 35 (7): 485- 505.
|
| 12 |
doi: 10.1038/s41467-021-25120-6 |
| 13 |
汪海霞, 张学东, 张舒林, 等. 2011—2023年南阳市临床检测呼吸道病原体流行趋势及新冠疫情防控的影响[J]. 中华医院感染学杂志, 2024, 34 (11): 1672- 1678.
|
| 14 |
曹艳, 陈雨, 伊洁, 等. 北京地区2023—2024年秋冬季急性呼吸道感染疾病的病原体流行情况分析: 以北京协和医院5556例患者为例[J/OL]. 协和医学杂志, 2024, 12 (2024-12-09)[2025-01-05]. https://link.cnki.net/urlid/11.5882.r.20241209.1043.002.
|
| 15 |
doi: 10.1056/NEJMp1209051 |
| 16 |
常子维, 唐海龙, 张娟, 等. 2011—2021年某院儿科住院呼吸道感染患儿病原体检测结果报告[J]. 中华医院感染学杂志, 2024, 34 (22): 3467- 3471.
|
| 17 |
World Health Organization. Global tuberculosis report 2024 [EB/OL]. (2024-10-29) [2025-01-01]. https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2024.
|
| 18 |
刘淑琼, 谢乐云, 曾赛珍, 等. 2013—2021年湖南地区社区获得性肺炎住院儿童肺炎支原体感染流行病学分析[J]. 中华微生物学和免疫学杂志, 2023, 43 (6): 432- 441.
|
| 19 |
张新星, 季伟, 顾文婧, 等. 2005年至2014年苏州地区儿童呼吸道肺炎支原体感染流行病学分析[J]. 中华传染病杂志, 2015, 33 (10): 594- 598.
|
| 20 |
毛碧波, 陈黛娜, 卢文波, 等. 2019—2023年宁波市0~17岁住院患儿肺炎支原体感染及耐药基因突变流行特征分析[J]. 中华预防医学杂志, 2024, 58 (7): 1035- 1040.
|
| 21 |
刘燕, 方巧云, 曾健君, 等. 2013—2017年惠州市重症社区获得性肺炎病例甲型流感/禽流感监测结果分析[J]. 实用预防医学, 2018, 25 (8): 922- 925.
|
| 22 |
权雅文, 李刚. 衰老与免疫的研究进展[J]. 中国临床保健杂志, 2022, 25 (4): 455- 459.
|
| 23 |
苏伟, 张复春. 甲型流感研究进展[J]. 新发传染病电子杂志, 2018, 3 (3): 182- 187.
|
| 24 |
doi: 10.1038/s41467-021-21157-9 |
| 25 |
|
| 26 |
doi: 10.1016/j.idnow.2021.05.004 |
| 27 |
韩鹏, 郑跃杰, 杨永弘, 等. 儿童新型冠状病毒流行期间的免疫债及其影响[J]. 中华实用儿科临床杂志, 2023, 38 (1): 4- 9.
|
| 28 |
曾艺, 孙艺, 杨泽璇, 等. 上海市大学生新冠肺炎疫情不同阶段知信行变化情况[J]. 中国学校卫生, 2022, 43 (11): 1655- 1658.
|
| 29 |
邹晓辉, 曹彬. 呼吸道感染病原学诊断年度进展2021[J]. 中华结核和呼吸杂志, 2022, 45 (1): 78- 82.
|
| 30 |
全旭. 新冠疫情下苏州地区下呼吸道感染住院儿童病原谱及合胞病毒感染临床特征的变化[D]. 苏州: 苏州大学, 2023.
|
| 31 |
马稹. 新冠疫情对住院社区获得性肺炎患儿常见呼吸道病毒流行趋势的影响[D]. 吉林: 吉林大学, 2023.
|
| 32 |
徐爱强, 冯录召, 谢正德. 我国婴幼儿呼吸道合胞病毒感染被动免疫预防专家共识[J]. 中国预防医学杂志, 2024, 25 (10): 1223- 1234.
|
| 33 |
张新燕, 马建中, 闫春娟. 2017—2022年天水市国家级某哨点医院流感监测结果分析[J]. 中国初级卫生保健, 2024, 38 (2): 70- 72.
|
| 34 |
麻粉莲, 郑丽舒. 人偏肺病毒感染研究进展[J]. 病毒学报, 2024, 40 (1): 133- 139.
|
| 35 |
刘洋, 游贤路, 韩真明. 重庆市百日咳流行病学特征及影响因素分析[J]. 现代预防医学, 2021, 48 (8): 1372- 1374.
|
| [1] | Doudou ZHAO, Xuan QI, Bo HUANG, Weibo GAO, Yuanyuan PEI, Yuebo JIN, Miao SHAO, Jing HE. Expression and clinical significance of lymphocyte subsets in infectious pneumonia and immune-related interstitial lung disease [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 624-630. |
| [2] | Jie ZHAO, Chun FU, Xiujuan ZHAO, Haiyan XUE, Shu LI, Zhenzhou WANG, Fengxue ZHU. Risk factors for ventilator-associated pneumonia in patients with chest trauma in intensive care unit [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 351-358. |
| [3] | Yunling GENG, Chao LIU, Ping YANG, Jiajia ZHENG, Ning SHEN, Yipeng DU. Clinical features and virulence gene distribution of Klebsiella pneumoniae multi-site infection in patients with hospital-acquired pneumonia [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 201-207. |
| [4] | Guangxu LIU, Liang ZHANG, Houyu ZHAO, Siwei DENG, Junting YANG, Ning LI, Rui MA, Yan HE, Guozhang XU, Zhike LIU, Siyan ZHAN. Epidemiological characteristics of febrile seizure among children under 6 years old in Ningbo City from 2015 to 2021 [J]. Journal of Peking University (Health Sciences), 2025, 57(3): 584-591. |
| [5] | Jiajun LIU, Guokang LIU, Yuhu ZHU. Immune-related severe pneumonia: A case report [J]. Journal of Peking University (Health Sciences), 2024, 56(5): 932-937. |
| [6] | Jinrong ZHU,Yana ZHAO,Wei HUANG,Weiwei ZHAO,Yue WANG,Song WANG,Chunyan SU. Clinical characteristics of COVID-19 infection in patients undergoing hemodialysis [J]. Journal of Peking University (Health Sciences), 2024, 56(2): 267-272. |
| [7] | Le-qing CAO,Jing-rui ZHOU,Yu-hong CHEN,Huan CHEN,Wei HAN,Yao CHEN,Yuan-yuan ZHANG,Chen-hua YAN,Yi-fei CHENG,Xiao-dong MO,Hai-xia FU,Ting-ting HAN,Meng LV,Jun KONG,Yu-qian SUN,Yu WANG,Lan-ping XU,Xiao-hui ZHANG,Xiao-jun HUANG. Relationship between treatment and prognosis in patients with late-onset severe pneumonia after allogeneic hematopoietic stem cell transplantation [J]. Journal of Peking University (Health Sciences), 2022, 54(5): 1013-1020. |
| [8] | Jing QIAN,You-jia WEI,Yi-jing CHENG,Yi ZHANG,Bo PENG,Chun-mei ZHU. Analysis of clinical features and risk factors of necrotizing pneumonia in children [J]. Journal of Peking University (Health Sciences), 2022, 54(3): 541-547. |
| [9] | LI Jia,XU Yu,WANG You-ya,GAO Zhan-cheng. Clinical characteristics of influenza pneumonia in the elderly and relationship between D-dimer and disease severity [J]. Journal of Peking University (Health Sciences), 2022, 54(1): 153-160. |
| [10] | WANG Fei,ZHU Xiang,HE Bei,ZHU Hong,SHEN Ning. Spontaneous remission of follicular bronchiolitis with nonspecific interstitial pneumonia: A case report and literature review [J]. Journal of Peking University (Health Sciences), 2021, 53(6): 1196-1200. |
| [11] | LIU Li-li,LIU Zhi-ke,ZHANG Liang,LI Ning,FANG Ting,Dong-ZHANG Liang,XU Guo-zhang,ZHAN Si-yan. Epidemiological and etiological characteristics of hand, foot and mouth disease among children aged 5 years and younger in Ningbo (2016 to 2019) [J]. Journal of Peking University (Health Sciences), 2021, 53(3): 491-497. |
| [12] | Fang BAO,Wei-li SHI,Jing HU,Di ZHANG,Dong-han GAO,Yun-xia XIA,Hong-mei JING,Xiao-yan KE,Qing-gang GE,Ning SHEN. Analysis of the correlation between lymphocyte subsets and severity of corona virus disease 19 [J]. Journal of Peking University (Health Sciences), 2020, 52(6): 1075-1081. |
| [13] | Xiao-ning YUAN,Qing-yang MENG,Ning SHEN,Yu-xuan LI,Chao LIANG,Man CUI,Qing-gang GE,Xiao-guang LI,Kun TAN,Qian CHEN,Jing WANG,Xiao-yong ZENG. Detection and evaluation of SARS-CoV-2 nucleic acid contamination in corona virus disease 19 ward surroundings and the surface of medical staff’s protective equipment [J]. Journal of Peking University (Health Sciences), 2020, 52(5): 803-808. |
| [14] | Qiu WANG,Jin-yu GUO,Hong SUN,Ling WANG,Ju-su YING,Hui-xin LIU. Investigation of protective exposure risk events in nurses against corona virus disease 2019 in Wuhan [J]. Journal of Peking University (Health Sciences), 2020, 52(4): 711-714. |
| [15] | Ming LU,Wei YAN,Xiang ZHU,Hong ZHU. Exogenous lipoid pneumonia induced by long-term usage of compound menthol nasal drops: a case report [J]. Journal of Peking University(Health Sciences), 2019, 51(2): 359-361. |
|
||