Journal of Peking University (Health Sciences) ›› 2026, Vol. 58 ›› Issue (3): 567-574. doi: 10.19723/j.issn.1671-167X.2026.03.017
Previous Articles Next Articles
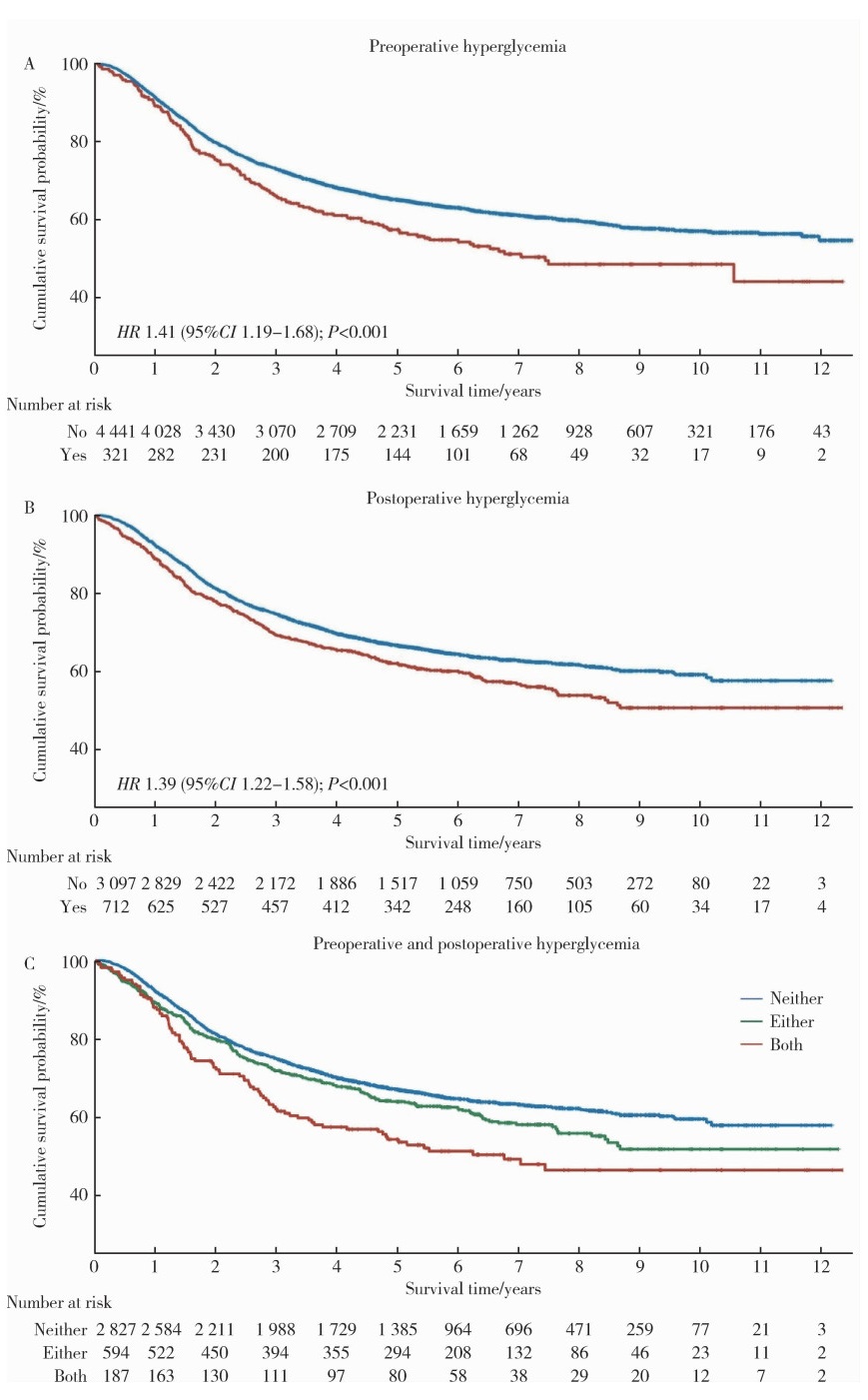
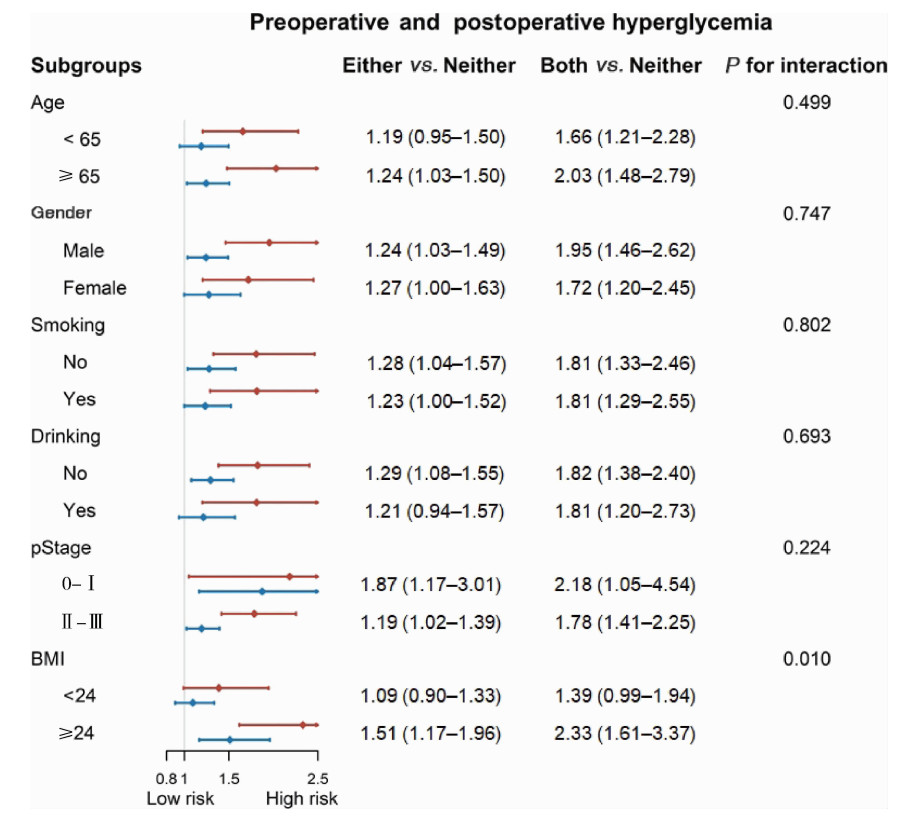
Perioperative hyperglycemia predicts poorer prognosis of esophageal squamous cell carcinoma patients treated with esophagectomy
Bo PENG1, Fangfang LIU1, Wei YANG2, Ruiping XU3, Lei CHEN2, Baozhong LI3, Xinjia WANG2, Ji KE1, Wenlei YANG1, Yu HE4, Zhen LIU1, Bolin HOU5, Liqun ZHANG2, Miaoping LIN2, Lixin ZHANG3, Fan ZHANG2, Fen CAI2, Huawen XU2, Mengfei LIU1, Ying LIU1, Yaqi PAN1, Zhonghu HE6,*( ), Yang KE6,*()
), Yang KE6,*()
- 1. Key Laboratory of Carcinogenesis and Translational Research(Ministry of Education), Department of Genetics, Peking University Cancer Hospital & Institute, Beijing 100142, China
2. Cancer Hospital of Shantou University Medical College, Shantou 515031, Guangdong, China
3. Anyang Cancer Hospital, Anyang 455000, Henan, China
4. Chinese Preventive Medicine Association, Beijing 100062, China
5. Linkdoc AI Research(LAIR), Beijing 100080, China
6. State Key Laboratory of Molecular Oncology, Department of Genetics, Peking University Cancer Hospital & Institute, Beijing 100142, China
CLC Number:
- R735.1

| 1 |
|
| 2 |
doi: 10.1136/gutjnl-2014-308124 |
| 3 |
doi: 10.1053/j.gastro.2017.08.023 |
| 4 |
doi: 10.20892/j.issn.2095-3941.2016.0093 |
| 5 |
doi: 10.1093/dote/doz091 |
| 6 |
doi: 10.1111/j.1442-2050.2008.00901.x |
| 7 |
doi: 10.1007/s10388-022-00950-5 |
| 8 |
|
| 9 |
doi: 10.1152/physrev.00030.2014 |
| 10 |
|
| 11 |
doi: 10.1097/SLA.0b013e31820b4bfc |
| 12 |
doi: 10.1097/00000658-200005000-00003 |
| 13 |
doi: 10.1186/s40880-018-0275-2 |
| 14 |
doi: 10.1093/dote/doz098 |
| 15 |
doi: 10.1016/j.ebiom.2017.01.035 |
| 16 |
doi: 10.1016/j.annepidem.2016.11.004 |
| 17 |
doi: 10.1016/j.eclinm.2020.100312 |
| 18 |
doi: 10.1245/s10434-010-1024-1 |
| 19 |
|
| 20 |
doi: 10.1503/cmaj.110977 |
| 21 |
doi: 10.1161/01.STR.0000085087.41330.FF |
| 22 |
doi: 10.1161/01.CIR.36.4.609 |
| 23 |
doi: 10.1093/qjmed/hcu218 |
| 24 |
|
| [1] | Siyan YUAN, Hewei MIN, Ping CHEN, Yibo WU, Hongxia CUI, Xuxi ZHANG, Xinying SUN. Health education preferences in patients with type 2 diabetes mellitus based on Big Five personality traits [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 600-605. |
| [2] | Fan SHU, Liyuan GE, Hanzhang DENG, Haoming YIN, Junyong OU, Shaohui DENG, Yichang HAO, Min LU, Zhanyi ZHANG, Peichen DUAN, Shudong ZHANG. Molecular characteristics for poor prognosis related renal cell carcinoma with lymph metastases [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 631-640. |
| [3] | Hao FU, Luyan SHEN, Bingyang HUANG, Shaohua MA. Clinical strategies for perioperative management of esophageal squamous cell carcinoma in the immunotherapy era [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 266-271. |
| [4] | Lingfu ZHANG, Ming CHEN, Xiaoyu ZHAO, Gang WANG, Long CUI, Xiaofeng LING, Lixin WANG, Zhi XU, Limei GUO, Chunsheng HOU. Gross classification of gallbladder cancer with primary lesion limited to the gallbladder wall and its correlation with prognosis and precancerous lesions [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 184-189. |
| [5] | Xueli TIAN, Zhiqiang SONG, Yonghui HUANG, Wei YAO. Analysis of early complications and risk factors in patients with amyotrophic lateral sclerosis after percutaneous endoscopic gastrostomy [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 190-195. |
| [6] | Xiaolin WANG, Shaoyi GUO, Dazhao CHEN, Xijie WEN, Yong HUA, Liang ZHANG, Qin ZHANG. A follow-up study on total hip arthroplasty in patients with systemic lupus erythematosus combined with osteonecrosis of femoral head [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1081-1088. |
| [7] | Hewei MIN, Yibo WU, Yuhui SHI, Mingzi LI, Xinying SUN. Analyzing the influential factors of dietary patterns and blood glucose control in type 2 diabetes patients based on the model of health action process approach model [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1145-1152. |
| [8] | Jingyan GU, Xinyi LI, Jinxia ZHAO, Rong MU. Diabetic Charcot neuroarthropathy initially misdiagnosed as rheumatoid arthritis and gout: A case report [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1193-1197. |
| [9] | Pei CAO, Qingxian LUAN. Periodontitis and systemic diseases: Thinking and explorations [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 852-858. |
| [10] | Boda GUO, Min LU, Guoliang WANG, Hongxian ZHANG, Lei LIU, Xiaofei HOU, Lei ZHAO, Xiaojun TIAN, Shudong ZHANG. Clinicopathological and prognostic differences between clear cell and non-clear cell renal cell carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 644-649. |
| [11] | Chao ZUO, Guoli WANG, Kunlin YANG, Xinyan CHE, Yisen MENG, Kai ZHANG. Comparison of efficacy and safety of transurethral thulium fiber laser enucleation of prostate in patients with different prostate volumes [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 711-716. |
| [12] | Zhao ZHAO, Weiyu ZHANG, Wenbo YANG, Yongjie ZHANG, Xiaopeng ZHANG, Huiying ZHAO, Gang ZHOU, Qiang WANG. Kidney transplantation in low-age, low-weight children: A report of two cases [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 803-807. |
| [13] | Ziyan CHEN, Xiaoyue ZHANG, Yiwu GU, Chun CHANG. Type 2 diabetes patients use E-health to manage disease willingness and influence mechanisms [J]. Journal of Peking University (Health Sciences), 2025, 57(3): 522-528. |
| [14] | Weihao LI, Jing LI, Xuemin ZHANG, Wei LI, Qingle LI, Xiaoming ZHANG. Effect of intraoperative blood salvage autotransfusion on the prognosis of patients after carotid body tumor resection [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 272-276. |
| [15] | Fei WANG, Xinyue ZHANG, Muqing LIU, Enbo WANG, Denghui DUAN. Clinical application and three-dimensional finite element analysis of along-axis extraction method in mandibular mesial and horizontally impacted third molar surgery [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 106-112. |
|
||