北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (6): 1003-1007. doi: 10.19723/j.issn.1671-167X.2019.06.004
抗氨基甲酰化蛋白抗体在类风湿关节炎合并肺间质病变早期诊断中的价值
竺红1,△( ),赵丽娟2,周艳1,陈瑶2
),赵丽娟2,周艳1,陈瑶2
- 1. 宁夏医科大学总医院风湿免疫科,宁夏银川 750004
2. 宁夏医科大学临床医学院,宁夏银川 750004
Significance of anti-carbamylated protein antibodies in patients with rheumatoid arthritis-associated intersitial lung disease
Hong ZHU1,△(),Li-juan ZHAO2,Yan ZHOU1,Yao CHEN2
- 1. Department of Rheumatology, General Hospital of Ningxia Medical University, Yinchuan 750004, China
2. Department of Clinical Medical College, Ningxia Medical University, Yinchuan, 750004, China
摘要:
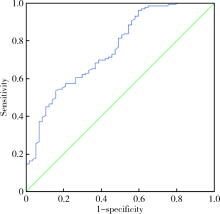
目的 探讨抗氨基甲酰化蛋白(carbamylated protein, CarP)抗体在类风湿关节炎(rheumatoid arthritis,RA)合并肺间质病变 (interstitial lung disease,ILD)早期诊断中的价值。方法 选择2017年12月至2019年6月在宁夏医科大学总医院风湿免疫科住院确诊为RA的患者,收集病例资料及血清标本,依据胸部CT检查结果分为RA-ILD组及单纯RA组,采用酶联免疫吸附试验(enzyme linked immunosorbent assay,ELISA)法测定各组血清中抗CarP抗体水平,分析其与RA-ILD的发生及其他实验室指标的相关性。组间计量资料比较采用两独立样本t检验或Mann-Whitney U检验;组间计数资料比较采用卡方检验;采用绘制受试者工作曲线(ROC曲线)确定抗CarP抗体对诊断RA-ILD最佳截断值并分析其诊断效能,相关性分析采用Spearman相关分析。结果 RA-ILD组抗CarP抗体水平为21.14(12.29,29.75), 明显高于单纯RA组的11.00(6.66,19.05),差异有统计学意义(P<0.05)。RA-ILD组抗CarP抗体阳性率(53%)高于单纯RA组(16%),差异有统计学意义(P<0.05);两组间类风湿因子(rheumatoid factor,RF)及抗环瓜氨酸肽(cyclic citrullinated peptide,CCP)抗体水平差异无统计学意义(P>0.05)。RA-ILD组年龄及疾病活动指数(disease activity score 28,DAS28)显著高于单纯RA组,差异有统计学意义(P<0.05)。RA-ILD组男性和吸烟比例高于单纯RA组,但差异无统计学意义(P>0.05)。通过绘制R0C曲线显示抗CarP抗体对RA-ILD诊断的最佳截断值为20.56 U/mL,灵敏度为53.50%,特异度为84.20%,曲线下面积为0.76 ;Spearman相关性分析示RF、年龄与抗CarP抗体呈正相关(r=0.172,P=0.043;r=0.200,P=0.006);抗CarP抗体水平与 DAS28 评分、红细胞沉降率(erythrocyte sedimentation rate,ESR)、C-反应蛋白(C-reactive protein, CRP)、抗CCP抗体、关节肿胀数和关节压痛数均无相关性(P>0.05)。结论 RA-ILD患者中血清抗CarP抗体浓度高于单纯RA患者,提示抗CarP抗体在RA-ILD发生发展中可能具有一定作用。
中图分类号:
- R593.22

| [1] | Ellman P, Ball RE . Rheumatoid disease with joint and pulmonary manifestations[J]. Br Med J, 1984,2(4583):816-820. |
| [2] | Bongartz T, Nannini C, Medina-Velasquez YF , et al. Incidence and mortality of interstitial lung disease in rheumatoid arthritis: apopulation-based study[J]. Arthritis Rheum, 2010,62(6):1583-1591. |
| [3] | 钟岩 . 类风湿关节炎合并间质性肺疾病的临床特点和危险因素分析[J]. 中国保健营养, 2017,27(18):119-120. |
| [4] | Šenolt L, Grassi W . Laboratory biomarkers or imaging in the diagnostics of rheumatoid arthritis[J]. BMC medicine, 2014,12(3):49-54. |
| [5] | 黄清水, 万腊根, 罗忠勤 , 等. 抗环瓜氨酸肽抗体对类风湿关节炎诊断价值的荟萃分析[J]. 中华医学杂志, 2006,86(31):2182-2187. |
| [6] | Shi J, van de Stadt LA, Levarht EW , et al. Anti-carbamylated protein antibodies are present in arthralgia patients and predict the development of rheumatoid arthritis[J]. Arthritis Rheum, 2013,65(4):911-915. |
| [7] | Scinocca M, Bell DA, Racape M , et al. Antihomocitrullinated fibrinogen antibodies are specific to rheumatoid arthritis and frequently bind citrullinated proteins/peptides[J]. J Rheumatol, 2014,41(2):270-279. |
| [8] | 竺红, 罗云霞, 杨亚珊 . 抗氨基甲酰化蛋白抗体在类风湿关节炎诊断价值中的评价. 中华风湿病学杂志, 2017,21(6):387-391 |
| [9] | Mohd NN, Mohd Shahrir MS, Shahid MS , et al. Clinical and high resolution computed tomography characteristics of patients with rheumatoid arthritis lung disease[J]. Int J Rheum Dis, 2009,12(2):136-144. |
| [10] | Zou YQ, Li YS, Ding XN , et al. The clinical significance of HRCT in evaluation of patients with rheumatoid arthritis-associated interstitial lung disease: a report from China[J]. Rheumatol Int, 2012,32(3):669-673. |
| [11] | Solomon JJ, Brown KK . Rheumatoid arthritis-associated interstital lung disease[J]. Open Access Rheumotal Res Rev, 2012,1(4):21-31. |
| [12] | Assayag D, Lubin M, Lee JS , et al. Predictors of mortality in rheumatoid arthritis-related interstitial lung disease[J]. Respirology, 2014,19(4):493-500. |
| [13] | Dawson JK, Fewins HE, Desmond J , et al. Fibrosing alveolitis in patients with rheumatoid arthritis as assessed by high resolution computed tomography, chest radiography, and pulmonary function tests[J]. Thorax, 2001,56(8):622-627. |
| [14] | Tanaka N, Kim JS, Newell JD , et al. Rheumatoid arthritis-related interstitial lung disease: CT findings[J]. Radiology, 2004,232(1):81-91. |
| [15] | Demoruelle MK, Solomon JJ, Fischer A , et al. The lung may play a role in the pathogenesis of rheumatoid arthritis[J]. Int J Clin Rheumtol, 2014,9(3):295-309. |
| [16] | Reynisdottir G, Karimi R, Joshua V , et al. Structural changes and antibody enrichment in the lungs are early features of anti-citrullinated protein antibody-positive rheumatoid arthritis[J]. Arthritis Rheum, 2014,66(1):31-39. |
| [17] | Kelly CA, Saravanan V, Nisar M , et al. Rheumatoid anhritis-related interstitial lung disease:associations,prognostic factors and physiological and radiological characteristics: a large multicentre UK study[J]. Rheumatology(0xford), 2014,53(9):1676-1682. |
| [18] | Basnakian AG, Shah SV, Ok E , et al. Carbamylated LDL[J]. Adv Clin Chem, 2010,51:25-52. |
| [19] | Shi J, Knevle R, Suwannalai P , et al. Autoantibodies recognizing carbamylated proteins are present in sera of patients with rheumatoid arthritis and predict joint damage[J]. Proc Natl Acad Sci USA, 2011,108(42):17372-17377. |
| [20] | Li L, Deng C, Chen S , et al. Meta-analysis:diagnostic accuracy of anti-carbamylated protein antibody for rheumatoid arthritis[J]. PLoS One, 2016,11(7):e0159000. |
| [21] | Ajeganova S, van Steenbergen HW, Verheul MK , et al. The association between anti-carbamylated prolein(anti-CarP) antibodies and radiographic progression in early rheumatoid arthritis: a study exploring replication and the added value to ACPA and rheumatoid factor[J]. Ann Rheum Dis, 2017,76(1):112-118. |
| [22] | Brink M, Verheul MK, Rnnelid J , et al. Anti-carbamylated protein antibodies in the pre-symptomatic phase of rheumatoid arthritis,their relationship with multiple anti-citrulline peptide antibodies and association with radiological damage[J]. Arthritis Res Ther, 2015,17(1):523-533. |
| [23] | 郑晓, 王玉梅, 刘秀梅 . 抗氨甲酰化蛋白抗体对类风湿关节炎的诊断价值[J]. 中华临床医师杂志: 电子版, 2017,11(4):570-573. |
| [24] | Restrepo JF, del Rincon I, Battafarano DF , et al. Clinical and laboratory factors associated with interstitial lung disease in rheumatoid arthritis[J]. Clin Rheumatol, 2015,34(9):1529-1536. |
| [25] | Sparks JA, He X, Huang J , et al. Rheumatoid arthritis disease activity predicting incident clinically apparent rheumatoid arthritis-associated interstitial lung disease: a prospective cohort study[J]. Arthritis Rheum, 2019,71(9):1472-1482. |
| [26] | Othman MA, Ghazal WSW, Hamid WZWA , et al. Anti-carbamylated protein antibodies in rheumatoid arthritis patients and their association with rheumatoid factor[J]. Saudi Med J, 2017,38(9):934-941. |
| [1] | 刘东武, 陈杰, 高明利, 于静. 类风湿关节炎伴发淋巴结Castleman样病理改变1例[J]. 北京大学学报(医学版), 2024, 56(5): 928-931. |
| [2] | 李正芳,罗采南,武丽君,吴雪,孟新艳,陈晓梅,石亚妹,钟岩. 抗氨基甲酰化蛋白抗体在诊断类风湿关节炎中的应用价值[J]. 北京大学学报(医学版), 2024, 56(4): 729-734. |
| [3] | 黄会娜,赵静,赵祥格,白自然,李霞,王冠. 乳酸对类风湿关节炎患者外周血CD4+T细胞亚群的调控作用[J]. 北京大学学报(医学版), 2024, 56(3): 519-525. |
| [4] | 汤晓菲,李永红,丁秋玲,孙卓,张阳,王育梅,田美伊,刘坚. 类风湿关节炎患者下肢深静脉血栓发病率及危险因素[J]. 北京大学学报(医学版), 2024, 56(2): 279-283. |
| [5] | 邹雪,白小娟,张丽卿. 艾拉莫德联合托法替布治疗难治性中重度类风湿关节炎的疗效[J]. 北京大学学报(医学版), 2023, 55(6): 1013-1021. |
| [6] | 吴琦,蔡月明,何娟,黄文蒂,王庆文. 血脂异常与类风湿关节炎肺间质病变的相关性分析[J]. 北京大学学报(医学版), 2023, 55(6): 982-992. |
| [7] | 张警丰,金银姬,魏慧,姚中强,赵金霞. 体重指数与类风湿关节炎临床特征的相关性分析[J]. 北京大学学报(医学版), 2023, 55(6): 993-999. |
| [8] | 金银姬,孙琳,赵金霞,刘湘源. 血清IgA型抗鼠科肉瘤病毒癌基因同源物B1抗体在类风湿关节炎中的意义[J]. 北京大学学报(医学版), 2023, 55(4): 631-635. |
| [9] | 蔡文心,李仕成,刘一鸣,梁如玉,李静,郭建萍,胡凡磊,孙晓麟,李春,刘栩,叶华,邓立宗,李茹,栗占国. 类风湿关节炎临床分层及其特征的横断面研究[J]. 北京大学学报(医学版), 2022, 54(6): 1068-1073. |
| [10] | 程昉,杨邵英,房星星,王璇,赵福涛. CCL28-CCR10通路在类风湿关节炎单核细胞迁移中的作用[J]. 北京大学学报(医学版), 2022, 54(6): 1074-1078. |
| [11] | 刘蕊,赵金霞,闫良. 类风湿关节炎合并下肢静脉血栓患者的临床特点[J]. 北京大学学报(医学版), 2022, 54(6): 1079-1085. |
| [12] | 张警丰,金银姬,魏慧,姚中强,赵金霞. 类风湿关节炎患者生活质量与疾病活动度的横断面研究[J]. 北京大学学报(医学版), 2022, 54(6): 1086-1093. |
| [13] | 高超,陈立红,王莉,姚鸿,黄晓玮,贾语博,刘田. 类风湿关节炎合并纤维肌痛简易分类标准的临床验证[J]. 北京大学学报(医学版), 2022, 54(2): 278-282. |
| [14] | 娄雪,廖莉,李兴珺,王楠,刘爽,崔若玫,徐健. 类风湿关节炎患者外周血TWEAK基因启动子区甲基化状态及其表达[J]. 北京大学学报(医学版), 2021, 53(6): 1020-1025. |
| [15] | 钟华,徐丽玲,白明欣,苏茵. 类风湿关节炎患者趋化因子CXCL9和CXCL10在骨侵蚀中的作用[J]. 北京大学学报(医学版), 2021, 53(6): 1026-1031. |
|
||
