北京大学学报(医学版) ›› 2024, Vol. 56 ›› Issue (2): 326-331. doi: 10.19723/j.issn.1671-167X.2024.02.020
肾血管平滑肌脂肪瘤破裂出血的手术时机
陈克伟,邓绍晖,刘茁,张洪宪,马潞林,张树栋*( )
)
- 北京大学第三医院泌尿外科, 北京 100191
Discussion on the surgical timing of rupture and hemorrhage of renal angiomyolipoma
Kewei CHEN,Shaohui DENG,Zhuo LIU,Hongxian ZHANG,Lulin MA,Shudong ZHANG*()
- Department of Urology, Peking University Third Hospital, Beijing 100191, China
摘要:
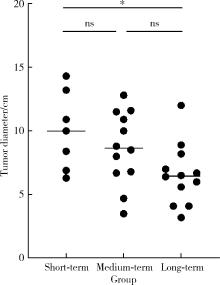
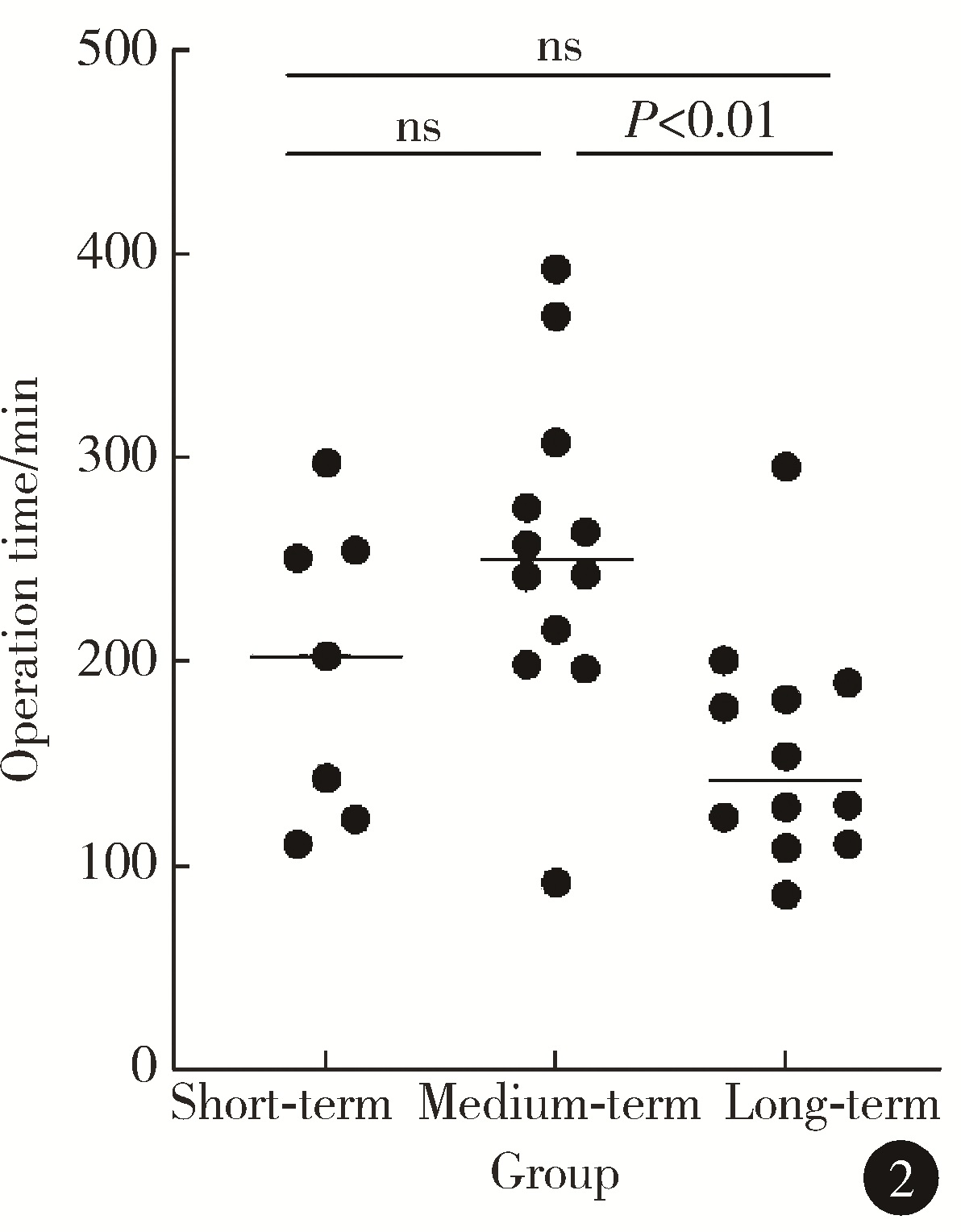
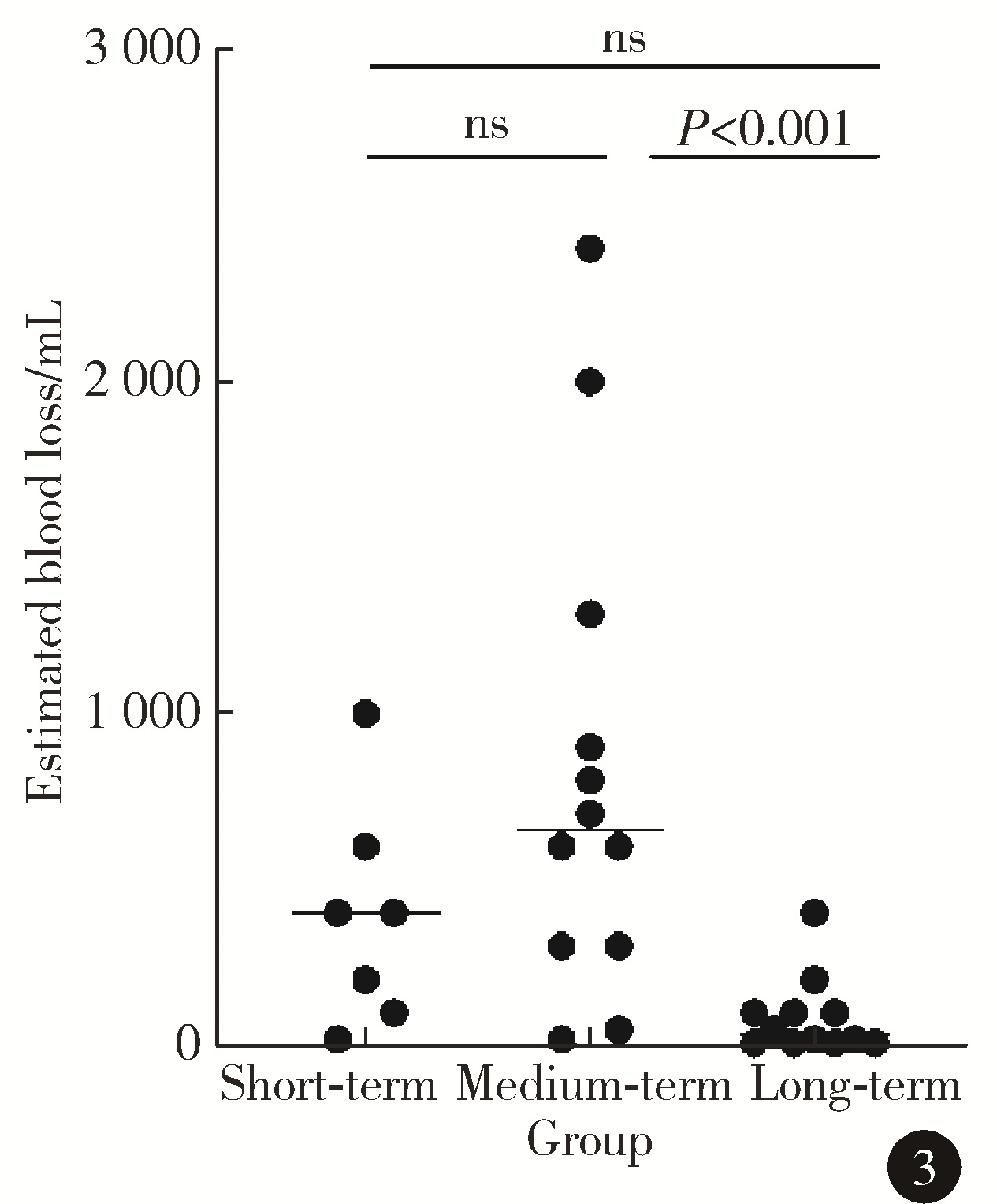
目的: 探讨不同的手术时机对肾血管平滑肌脂肪瘤(renal angiomyolipoma,RAML)破裂出血患者手术治疗效果的影响。方法: 选择北京大学第三医院泌尿外科2013年6月至2023年2月收治的31例RAML破裂出血患者的病例资料进行回顾性分析,记录患者人口学和围手术期资料,将出血后小于7 d手术定义为近期手术组,出血后7 d至6个月手术定义为中期手术组,出血后超过6个月手术定义为远期手术组,比较组间的围手术期相关指标。结果: 收集到行RAML破裂出血手术治疗的患者共31例,其中男性13例,女性18例,平均年龄(46.2±11.3)岁。近期手术组7例,中期手术组12例,远期手术组12例。肿瘤直径方面,远期手术组患者显著低于近期手术组[(6.6±2.4) cm vs. (10.0±3.0) cm, P=0.039];手术时间方面,远期手术组显著低于中期手术组[(157.5±56.8) min vs. (254.8±80.1) min, P=0.006],其余组间比较差异无统计学意义;出血量方面,远期手术组低于中期手术组[35 (10,100) mL vs. 650 (300,1 200) mL,P<0.001],其余组间比较差异无统计学意义;术中输血量方面,远期手术组显著低于中期手术组[ 0 (0,0) mL vs. 200 (0,700) mL, P=0.014],其余组间比较差异无统计学意义;术后住院天数方面,远期手术组显著低于中期手术组[5 (4, 7) d vs. 7 (6, 10) d,P=0.011],其余组间比较差异无统计学意义。结论: 对于RAML破裂出血的患者,6个月以上再行手术是一个相对安全的时间,手术时间相对最短,术中出血量相对最少,因此更推荐待保守治疗血肿机化后再进行手术治疗。
中图分类号:
- R737.11





| 1 |
Castle SM , Gorbatiy V , Ekwenna O , et al. Radiofrequency ablation (RFA) therapy for renal angiomyolipoma (AML): An alternative to angio-embolization and nephron-sparing surgery[J]. BJU Int, 2012, 109 (3): 384- 387.
doi: 10.1111/j.1464-410X.2011.10376.x |
| 2 |
Seyam RM , Alkhudair WK , Kattan SA , et al. The risks of renal angiomyolipoma: Reviewing the evidence[J]. J Kidney Cancer VHL, 2017, 4 (4): 13- 25.
doi: 10.15586/jkcvhl.2017.97 |
| 3 |
Yamakado K , Tanaka N , Nakagawa T , et al. Renal angiomyolipoma: Relationships between tumor size, aneurysm formation, and rupture[J]. Radiology, 2002, 225 (1): 78- 82.
doi: 10.1148/radiol.2251011477 |
| 4 |
Kothary N , Soulen MC , Clark TW , et al. Renal angiomyolipoma: Long-term results after arterial embolization[J]. J Vasc Interv Radiol, 2005, 16 (1): 45- 50.
doi: 10.1097/01.RVI.0000143769.79774.70 |
| 5 | 孙青风, 王侠, 吴斌. 154例肾血管平滑肌脂肪瘤诊治原则的探讨[J]. 中国自然医学杂志, 2008, 10 (4): 259- 262. |
| 6 | Nelson CP , Sanda MG . Contemporary diagnosis and management of renal angiomyolipoma[J]. J Urol, 2002, 168 (4 Pt 1): 1315- 1325. |
| 7 | Eble JN . Angiomyolipoma of kidney[J]. Semin Diagn Pathol, 1998, 15 (1): 21- 40. |
| 8 |
Neumann HP , Schwarzkopf G , Henske EP . Renal angiomyolipomas, cysts, and cancer in tuberous sclerosis complex[J]. Semin Pediatr Neurol, 1998, 5 (4): 269- 275.
doi: 10.1016/S1071-9091(98)80005-3 |
| 9 |
Parmar N , Langdon J , Kaliannan K , et al. Wunderlich syndrome: Wonder what it is[J]. Curr Probl Diagn Radiol, 2022, 51 (2): 270- 281.
doi: 10.1067/j.cpradiol.2020.12.002 |
| 10 |
Xu XF , Hu XH , Zuo QM , et al. A scoring system based on clinical features for the prediction of sporadic renal angiomyolipoma rupture and hemorrhage[J]. Medicine (Baltimore), 2020, 99 (20): e20167.
doi: 10.1097/MD.0000000000020167 |
| 11 |
Earthman WJ , Mazer MJ , Winfield AC . Angiomyolipomas in tuberous sclerosis: Subselective embolotherapy with alcohol, with long-term follow-up study[J]. Radiology, 1986, 160 (2): 437- 441.
doi: 10.1148/radiology.160.2.3726123 |
| 12 |
Ewalt DH , Diamond N , Rees C , et al. Long-term outcome of transcatheter embolization of renal angiomyolipomas due to tuberous sclerosis complex[J]. J Urol, 2005, 174 (5): 1764- 1766.
doi: 10.1097/01.ju.0000177497.31986.64 |
| 13 | 郑汉雄, 汪曾荣, 夏昕晖, 等. 手术切除与介入栓塞治疗肾错构瘤破裂出血的疗效比较[J]. 现代肿瘤医学, 2015, 23 (22): 3296- 3298. |
| 14 |
Bissler JJ , Racadio J , Donnelly LF , et al. Reduction of postembolization syndrome after ablation of renal angiomyolipoma[J]. Am J Kidney Dis, 2002, 39 (5): 966- 971.
doi: 10.1053/ajkd.2002.32770 |
| 15 | 陈挺, 张宝金, 颜力昊, 等. 肾错构瘤破裂出血的急诊处理[J]. 临床泌尿外科杂志, 2003, 18 (10): 588- 589. |
| 16 | 江洪涛, 陈昭典, 沈周俊, 等. 肾错构瘤破裂出血的诊治(附10例报告)[J]. 临床泌尿外科杂志, 2000, 15 (8): 347- 348. |
| 17 | 李四化, 陈羽, 张俊隆, 等. 肾血管平滑肌脂肪瘤破裂出血不同手术时机的围手术期风险评估[J]. 中山大学学报(医学版), 2018, 39 (3): 400. |
| 18 | 杨兴国, 聂勇, 程帆, 等. 多中心肾错构瘤破裂出血急诊手术与非手术治疗疗效比较(附53例报告)[J]. 临床泌尿外科杂志, 2016, 31 (2): 115- 119. |
| [1] | 虞乐,邓绍晖,张帆,颜野,叶剑飞,张树栋. 具有低度恶性潜能的多房囊性肾肿瘤的临床病理特征及预后[J]. 北京大学学报(医学版), 2024, 56(4): 661-666. |
| [2] | 陈克伟,刘茁,邓绍晖,张帆,叶剑飞,王国良,张树栋. 肾血管平滑肌脂肪瘤伴下腔静脉瘤栓的临床诊治[J]. 北京大学学报(医学版), 2024, 56(4): 617-623. |
| [3] | 高卿,陈彧,刘刚,陈生龙,董穗欣. 心肌梗死后室间隔穿孔:非选择性病例的外科临床结果[J]. 北京大学学报(医学版), 2019, 51(6): 1103-1107. |
| [4] | 张苏杰,赵卫红,于路平,殷华奇,张晓威,李清,刘士军,徐涛. 伴多发淋巴结肿大的乏脂型血管平滑肌脂肪瘤并发术后顽固性淋巴瘘1例报道及文献回顾[J]. 北京大学学报(医学版), 2018, 50(4): 717-721. |
| [5] | 叶雄俊,刘军,阿不都克依木·阿不力米提,熊六林,刘士军,徐涛,黄晓波. 后腹腔镜联合经腰小切口“杂交”手术在复杂肾肿瘤保留肾单位手术中的应用[J]. 北京大学学报(医学版), 2017, 49(4): 613-616. |
|
||
