北京大学学报(医学版) ›› 2025, Vol. 57 ›› Issue (2): 267-271. doi: 10.19723/j.issn.1671-167X.2025.02.007
急性心肌梗死血运重建后冠状动脉微循环障碍对患者住院期间急性左心衰竭的预测价值
王岚1, 马玉良1, 王伟民1,*( ), 朱天刚1, 靳文英1, 赵红1, 曹成富1, 王静1, 姜柏林2
), 朱天刚1, 靳文英1, 赵红1, 曹成富1, 王静1, 姜柏林2
- 1. 北京大学人民医院心血管内科,急性心肌梗死早期预警和干预北京市重点实验室,心血管转化医学研究中心,北京 100044
2. 北京大学人民医院麻醉科,北京 100044
Predictive value of coronary microcirculation dysfunction after revascularization in patients with acute myocardial infarction for acute heart failure during hospitalization
Lan WANG1, Yuliang MA1, Weimin WANG1,*(), Tiangang ZHU1, Wenying JIN1, Hong ZHAO1, Chengfu CAO1, Jing WANG1, Bailin JIANG2
- 1. Department of Cardiology, Peking University People' s Hospital, Beijing Key Laboratory of Early Prediction and Intervention of Acute Myocardial Infarction, Center for Cardiovascular Translational Research, Beijing 100044, China
2. Department of Anesthesiology, Peking University People' s Hospital, Beijing 100044, China
摘要:
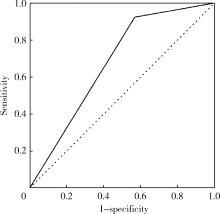
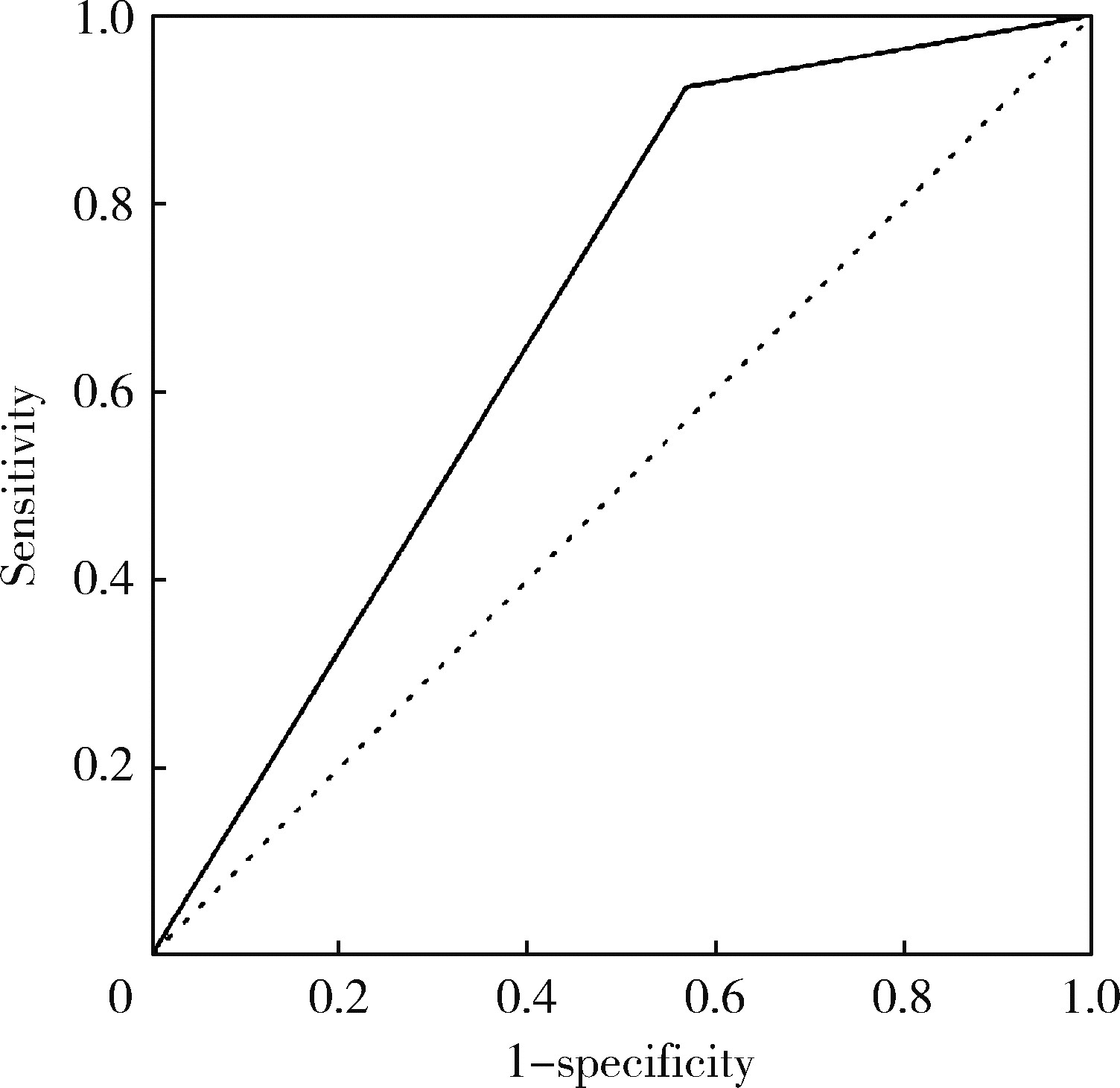
目的: 评估已行血运重建的急性心肌梗死(acute myocardial infarction,AMI)患者冠状动脉微循环障碍(coronary microcirculation dysfunction,CMD)的发生情况、临床特点,以及CMD对患者住院期间发生急性左心衰竭的预测价值。方法: 回顾性入选2015年11月至2021年7月北京大学人民医院因AMI住院,已行经皮冠状动脉介入术(percutaneous coronary intervention,PCI)完成罪犯血管血运重建,并于住院期间完成心肌声学造影(myocardial contrast echocardiography,MCE)的患者145例,根据MCE结果分为CMD组及冠状动脉微循环正常组。收集两组患者的临床资料及MCE资料,比较两组患者住院期间急性左心衰竭的发生率。应用二元Logistic回归分析校正混杂因素,探讨CMD患者发生急性左心衰竭的风险,绘制受试者工作特征(receiver operating characteristic,ROC)曲线,评估CMD对患者住院期间急性左心衰竭的预测价值。结果: 145例已行PCI的AMI患者中有87例(60%)存在CMD。与正常组相比,CMD组患者肌钙蛋白I(troponin I,TnI)峰值更高[52.8(8.1,84.0) μg/L vs. 18.9(5.7,56.1) μg/L,P=0.005],Killip分级更差(P=0.030),罪犯血管分布不同(P < 0.001),且罪犯血管PCI术前心肌梗死溶栓(thrombolysis in myocardial infarction,TIMI)血流 < 3级者更多(65.1% vs. 43.1%,P=0.025)。MCE结果显示,与正常组相比,CMD组患者左心室射血分数(left ventricular ejection fraction,LVEF)、整体长轴应变(global longitudinal strain,GLS)及室壁运动计分指数(wall motion score index,WMSI)更差(P均 < 0.001)。CMD组患者住院期间发生急性左心衰竭的比例显著高于正常组(13.8% vs. 1.7%,P=0.013),校正罪犯血管分布、罪犯血管术前TIMI血流及TnI峰值后,CMD组患者急性左心衰竭的风险依旧升高(OR=9.120,95%CI:1.152~72.192,P=0.036)。CMD预测已行血运重建的AMI患者住院期间急性左心衰竭的ROC曲线下面积(area under curve,AUC)为0.677(95%CI:0.551~0.804,P=0.035)。结论: AMI患者PCI术后依然有60%存在MCE检出的CMD,合并CMD的患者住院期间急性左心衰竭的风险显著增加。
中图分类号:
- R542.22
| 1 | 《中国心血管健康及与疾病报告》编写组. 中国心血管健康与疾病报告2019概要[J]. 中国循环杂志, 2020, 35 (9): 833- 854. |
| 2 |
张岩, 霍勇. 推动我国医疗急救体系建设: 从急性心肌梗死救治开始[J]. 北京大学学报(医学版), 2014, 46 (6): 829- 831.
doi: 10.3969/j.issn.1671-167X.2014.06.001 |
| 3 |
Thygesen K , Alpert JS , Jaffe AS , et al. Fourth universal definition of myocardial infarction (2018)[J]. JACC, 2018, 72 (18): 2231- 2264.
doi: 10.1016/j.jacc.2018.08.1038 |
| 4 |
De Waha S , Patel MR , Granger CB , et al. Relationship between microvascular obstruction and adverse events following primary percutaneous coronary intervention for ST-segment elevation myocar-dial infarction: An individual patient data pooled analysis from seven randomized trials[J]. Eur Heart J, 2017, 38 (47): 3502- 3510.
doi: 10.1093/eurheartj/ehx414 |
| 5 | 中华医学会心血管病分会, 中华心血管病杂志编辑委员会. 急性ST段抬高型心肌梗死诊断和治疗指南(2019)[J]. 中华心血管病杂志, 2019, 47 (10): 766- 783. |
| 6 |
Ibanez B , James S , Agewall S , et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC)[J]. Eur Heart J, 2018, 39 (2): 119- 177.
doi: 10.1093/eurheartj/ehx393 |
| 7 |
Bozkurt B , Coats AJS , Tsutsui H , et al. Universal definition and classification of heart failure: A report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association[J]. Eur J Heart Fail, 2021, 23 (3): 352- 380.
doi: 10.1002/ejhf.2115 |
| 8 | Lang RM , Badano LP , Mor-Avi V , et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging[J]. J Am Soc Echocardiogr, 2015, 28 (1): 1- 39.e14. |
| 9 |
Padro T , Manfrini O , Bugiardini R , et al. ESC Working Group on coronary pathophysiology and microcirculation position paper on 'coronary microvascular dysfunction in cardiovascular disease'[J]. Cardiovasc Res, 2020, 116 (4): 741- 755.
doi: 10.1093/cvr/cvaa003 |
| 10 |
段天兵, 向定成. 急性心肌梗死后冠状动脉微循环障碍发生机制和诊治方法的研究进展[J]. 中国循环杂志, 2019, 34 (7): 722- 725.
doi: 10.3969/j.issn.1000-3614.2019.07.019 |
| 11 | Marc MC , Iancu AC , Bǎlǎnescu Ş , et al. Microvascular obstruction in acute myocardial infarction: An old and unsolved mystery[J]. Med Pharm Rep, 2019, 92 (3): 216- 219. |
| 12 |
Kali A , Cokic I , Tang R , et al. Persistent microvascular obstruction after myocardial infarction culminates in the confluence of ferric iron oxide crystals, proinflammatory burden, and adverse remodeling[J]. Circ Cardiovasc Imaging, 2016, 9 (11): e004996.
doi: 10.1161/CIRCIMAGING.115.004996 |
| 13 | Tsukui T , Sakakura K , Taniguchi Y , et al. Factors associated with poor clinical outcomes of ST-elevation myocardial infarction in patients with door-to-balloon time < 90 minutes[J]. PLoS One, 2020, 15 (10): e0241251. |
| 14 |
Schaaf MJ , Mewton N , Rioufol G , et al. Pre-PCI angiographic TIMI flow in the culprit coronary artery influences infarct size and microvascular obstruction in STEMI patients[J]. J Cardiol, 2016, 67 (3): 248- 253.
doi: 10.1016/j.jjcc.2015.05.008 |
| [1] | 刘园梅, 傅义程, 郝靖欣, 张福春, 刘慧琳. 老年髋部骨折患者住院期间发生术后心力衰竭的列线图预测模型的构建及验证[J]. 北京大学学报(医学版), 2024, 56(5): 874-883. |
| [2] | 王方芳,梁芙萌,李楠,王晓晓,韩江莉,郭丽君. 急性前壁ST段抬高型心肌梗死患者直接冠状动脉介入术后微循环阻力指数与左心室不良重构的相关性[J]. 北京大学学报(医学版), 2024, 56(1): 150-156. |
| [3] | 高卿,陈彧,刘刚,陈生龙,董穗欣. 心肌梗死后室间隔穿孔:非选择性病例的外科临床结果[J]. 北京大学学报(医学版), 2019, 51(6): 1103-1107. |
| [4] | 夏经钢, 曲杨, 胡少东, 许骥, 尹春琳, 徐东. 替格瑞洛对急性ST段抬高型心肌梗死患者行急诊介入治疗的中期随访[J]. 北京大学学报(医学版), 2015, 47(3): 494-498. |
| [5] | 张岩, 霍勇. 推动我国医疗急救体系建设:从急性心肌梗死救治开始[J]. 北京大学学报(医学版), 2014, 46(6): 829-831. |
| [6] | 王宁, 王贵松, 于海奕, 米琳, 郭丽君, 高炜. 远隔缺血后适应在急性ST段抬高型心肌梗死直接经皮冠状动脉介入治疗术中的心肌保护作用[J]. 北京大学学报(医学版), 2014, 46(6): 838-843. |
| [7] | 陈少敏, 牟笛, 崔鸣, 任川, 张舒, 郭丽君. 直接经皮冠状动脉介入治疗急性心肌梗死患者血清组胺水平与心电图ST段回落的关系[J]. 北京大学学报(医学版), 2014, 46(6): 875-878. |
| [8] | 李昊, 张幼怡. 促炎细胞因子在交感/儿茶酚胺介导心脏重塑中的作用[J]. 北京大学学报(医学版), 2014, 46(6): 1001-1004. |
| [9] | 夏经钢, 曲杨, 胡少东, 许骥, 尹春琳, 徐东. 强化调脂对行非心脏手术的冠状动脉粥样硬化性心脏病患者的心肌保护作用及机制初探[J]. 北京大学学报(医学版), 2014, 46(4): 601-605. |
| [10] | 孟磊,王洁,丁文惠,杨颖,齐丽彤,霍勇. 急性心肌梗死患者血浆骨桥蛋白变化与左心室重构[J]. 北京大学学报(医学版), 2013, 45(4): 630-. |
| [11] | 李蓬*, 和璐, 沙月琴, 栾庆先 . 陈旧性心肌梗死患者的牙周状况[J]. 北京大学学报(医学版), 2013, 45(1): 22-26. |
| [12] | 曾鸿, 李晓曦, 赵文秋, 冯新恒, 郭向阳. 围产期心肌病合并急性心力衰竭剖宫产麻醉处理1例[J]. 北京大学学报(医学版), 2012, 44(5): 804-807. |
| [13] | 赵威, 白瑾, 张福春, 王鸿艳, 高炜. 急性ST段抬高心肌梗死患者早期心肺运动试验的安全性[J]. 北京大学学报(医学版), 2011, 43(4): 608-611. |
| [14] | 郑凌冰, 郭艳红, 于海奕, 米琳, 汪宇鹏, 高炜. 血清生长分化因子-15与急性冠状动脉综合征的相关性分析[J]. 北京大学学报(医学版), 2011, 43(2): 250-254. |
| [15] | 陈明, 王新刚, 霍勇. 主动脉内球囊反搏在心源性休克中的应用[J]. 北京大学学报(医学版), 2009, 41(4): 474-476. |
|
||
