北京大学学报(医学版) ›› 2026, Vol. 58 ›› Issue (1): 37-42. doi: 10.19723/j.issn.1671-167X.2026.01.005
赤藓糖醇喷砂与超声治疗对种植体周黏膜炎疗效的随机对照临床研究
孙菲1,2, 王翠2, 李思琪2, 危伊萍2, 余日月1,*( ), 胡文杰2,*()
), 胡文杰2,*()
- 1. 首都医科大学附属北京世纪坛医院口腔科, 北京 100089
2. 北京大学口腔医学院·口腔医院牙周科, 国家口腔医学中心, 国家口腔疾病临床医学研究中心, 口腔生物材料和数字诊疗装备国家工程研究中心, 北京 100081
Treatment of peri-implant mucositis using an erythritol air-polishing or ultrasonic device: A randomized controlled trial
Fei SUN1,2, Cui WANG2, Siqi LI2, Yiping WEI2, Riyue YU1,*(), Wenjie HU2,*()
- 1. Department of Stomatology, Beijing Shijitan Hospital, Capital Medical University, Beijing 100089, China
2. Department of Periodontology, Peking University School and Hospital of Stomatology & National Center for Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Research Center of Oral Biomaterials and Digital Medical Devices, Beijing 100081, China
摘要:
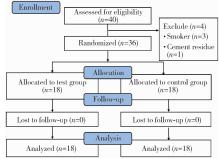
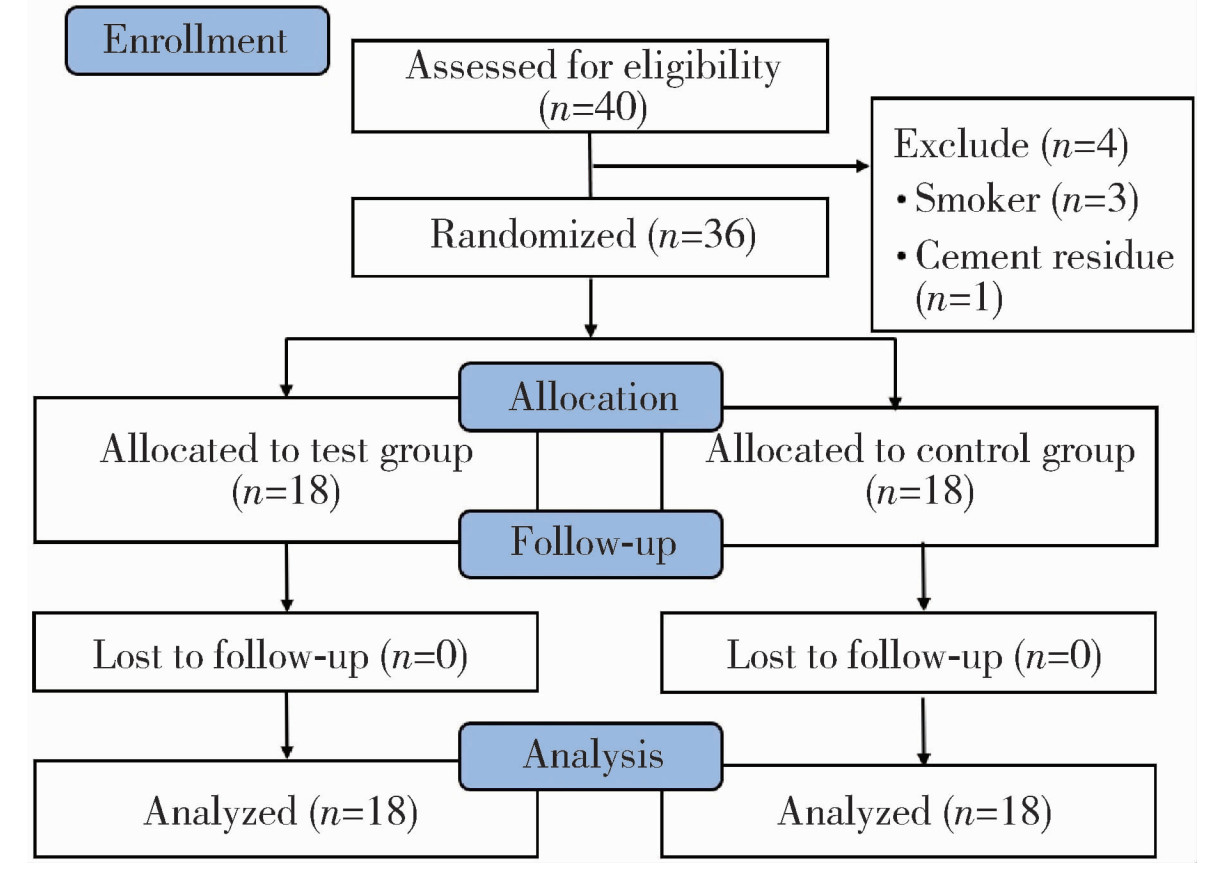
目的: 比较赤藓糖醇喷砂(erythritol air-polishing, EAP)和超声(ultrasonic debridement, US)两种方法治疗种植体周黏膜炎的短期临床疗效差异, 并评估患者报告的结局。方法: 为单盲、随机对照临床研究, 研究对象为2021年6月至2022年5月就诊于北京大学口腔医院牙周科的种植体周黏膜炎患者。共纳入36例患者(每例纳入1颗种植体), 随机分为EAP组(n=18)和US组(n=18)。分别于基线、治疗后1个月及3个月采集临床指标。主要结局指标为种植体周探诊深度(peri-implant probing depths, PPD)的变化, 次要结局指标为改良菌斑指数(modified plaque index, mPLI)、探诊出血(bleeding on probing, BOP)、探诊溢脓(suppuration on probing, SoP)、疼痛视觉模拟评分(visual analogue scale, VAS)。此外, 作为探索性分析, 还比较了两组患者PPD≥4 mm位点的比例。每次就诊均强化口腔卫生宣教, 并对种植体上部结构进行抛光。结果: EAP组和US组基线期临床指标具有可比性。对于主要结局指标平均PPD, EAP组较基线值(4.0±0.5) mm显著降低, 在治疗后1个月和3个月时分别降至(3.7±0.6) mm和(3.4±0.5) mm, 差异均具有统计学意义(P=0.011; P < 0.001);US组的平均PPD也较基线值(3.8±0.4) mm显著降低, 在治疗后1个月和3个月时分别降至(3.6±0.5) mm和(3.5±0.4) mm, 差异均具有统计学意义(P=0.038;P=0.018), 但两组间在各时间点的差异均无统计学意义(P>0.05)。次要结局指标中, 两组的平均mPLI(1、3个月均P < 0.001)与BOP(1个月P < 0.05; 3个月P < 0.001)均较基线显著改善, 治疗后VAS评分均较低, 但此三项指标的组间差异均无统计学意义(P>0.05)。治疗后3个月, EAP组PPD≥4 mm位点比例显著低于US组[(42.6±26.1)% vs.(57.4±25.1)%], 差异具有统计学意义(P=0.029)。研究期间未报告不良事件。结论: EAP与US均是治疗种植体周黏膜炎的有效方法, 总体疗效相当; 然而, 在减少深袋位点方面, EAP展现出短期潜力, 此结果尚需进一步验证。
中图分类号:
- R781.4
| 1 |
doi: 10.1016/j.jdent.2025.105914 |
| 2 |
doi: 10.1111/clr.13684 |
| 3 |
doi: 10.3390/ijerph20010477 |
| 4 |
doi: 10.1002/JPER.24-0154 |
| 5 |
|
| 6 |
doi: 10.1111/j.1600-0501.2011.02220.x |
| 7 |
doi: 10.1111/clr.12912 |
| 8 |
|
| 9 |
doi: 10.1186/s12903-022-02120-6 |
| 10 |
doi: 10.1186/s40729-025-00591-0 |
| 11 |
|
| 12 |
doi: 10.1111/idh.12206 |
| 13 |
doi: 10.3390/ma11091510 |
| 14 |
|
| 15 |
doi: 10.1111/jcpe.12395 |
| 16 |
靖无迪, 王宪娥, 谢也斯, 等. 甘氨酸龈下喷砂治疗早期种植体周围病的疗效观察[J]. 中华口腔医学杂志, 2017, 52(8): 480- 485.
|
| 17 |
doi: 10.1111/cid.13304 |
| 18 |
doi: 10.1111/idh.12814 |
| 19 |
doi: 10.1186/s12903-021-01397-3 |
| [1] | 孙菲,李思琪,危伊萍,钟金晟,王翠,胡文杰. 种植体周病非手术治疗中联合应用甘氨酸粉喷砂的临床效果评价[J]. 北京大学学报(医学版), 2022, 54(1): 119-125. |
|
||
