北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (4): 798-802. doi: 10.19723/j.issn.1671-167X.2021.04.030
耻骨下缘部分切除辅助后尿道吻合术在男性骨盆骨折后尿道离断修复中的应用
王建伟,徐啸,鲍正清,刘振华,何峰,黄广林,满立波( )
)
- 北京积水潭医院,北京大学第四临床医学院泌尿外科, 北京 100096
Outcomes of partial pubectomy assisted anastomotic urethroplasty for male patients with pelvic fracture urethral distraction defect
WANG Jian-wei,XU Xiao,BAO Zheng-qing,LIU Zhen-hua,HE Feng,HUANG Guang-lin,MAN Li-bo()
- Department of Urology, Beijing Jishuitan Hospital, the Fourth Medical College of Peking University, Beijing 100096, China
摘要:
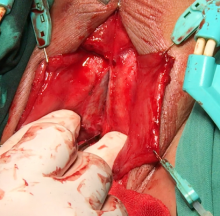
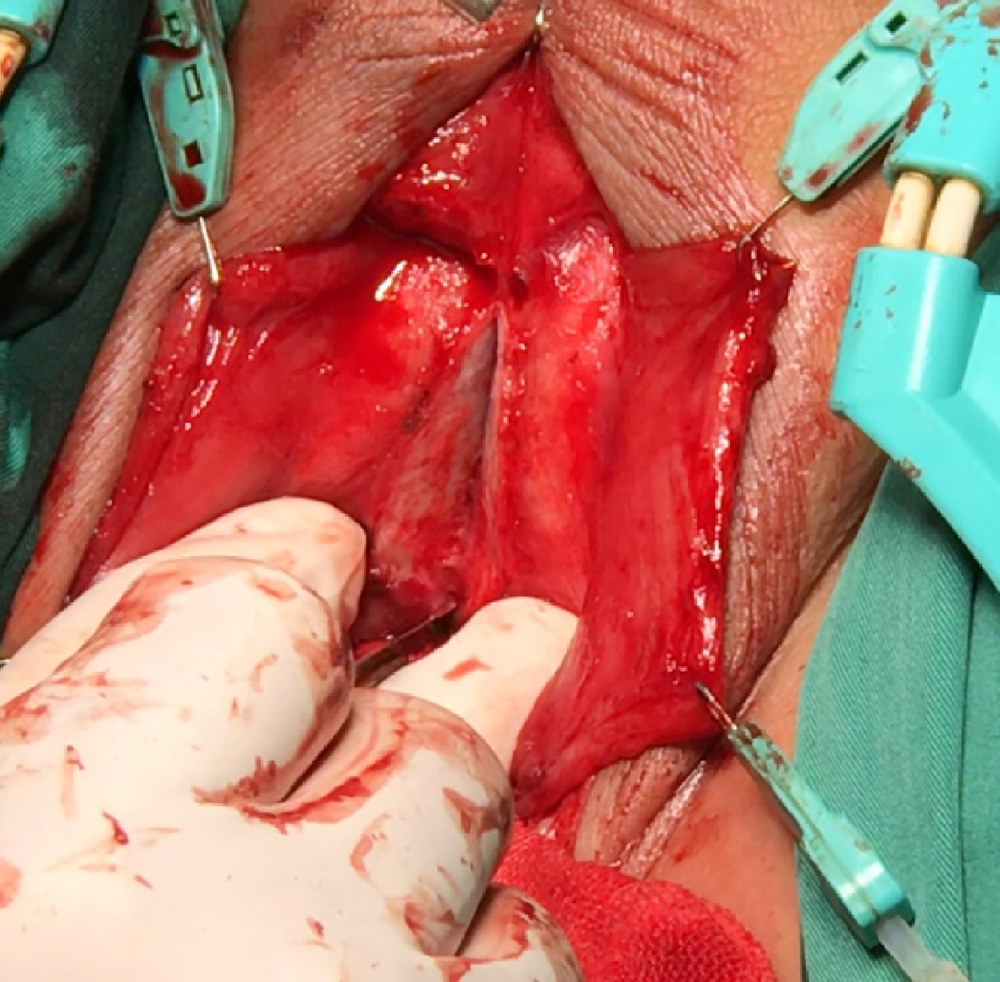
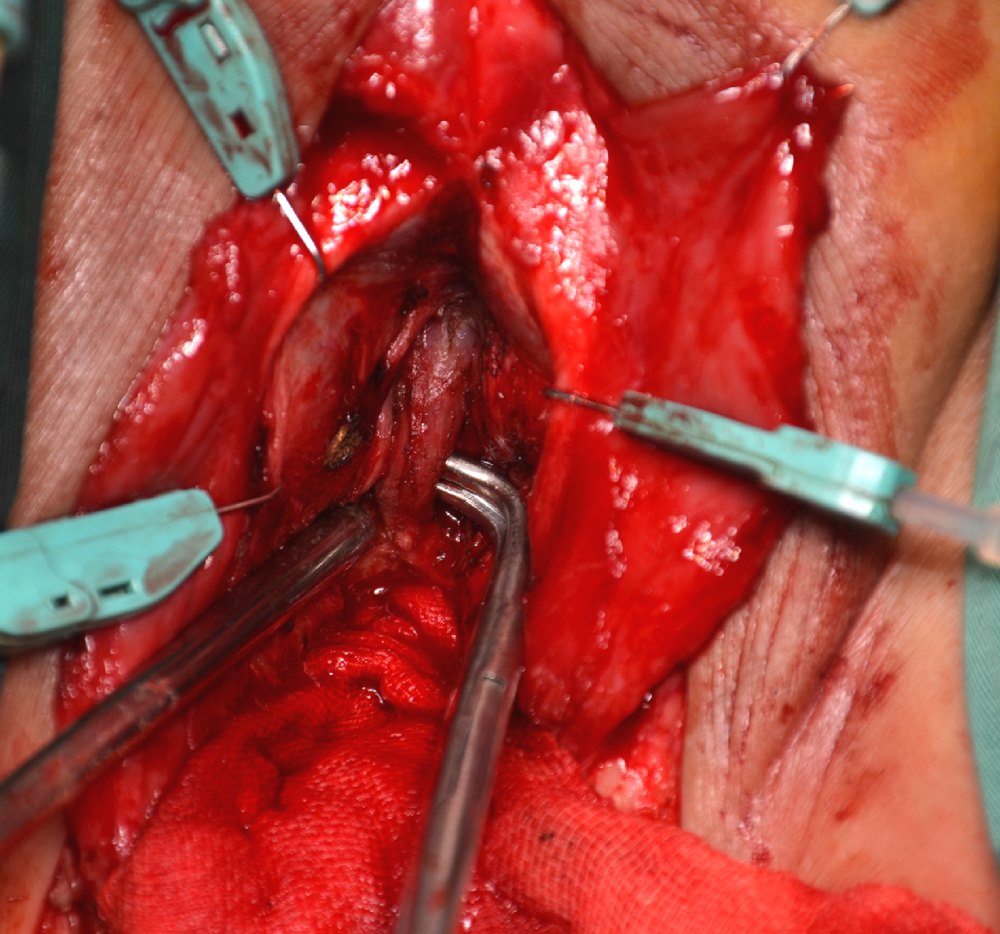
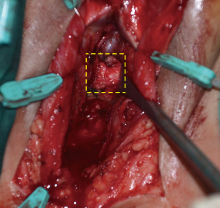
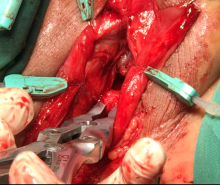
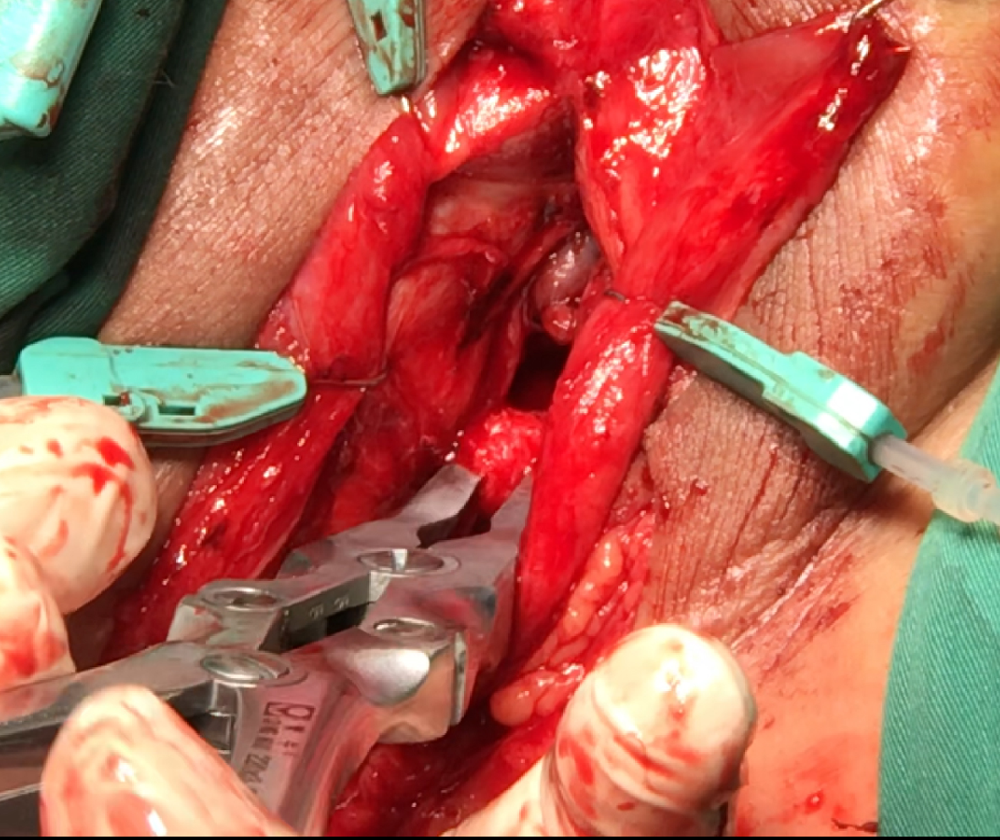
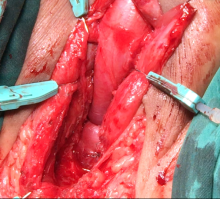
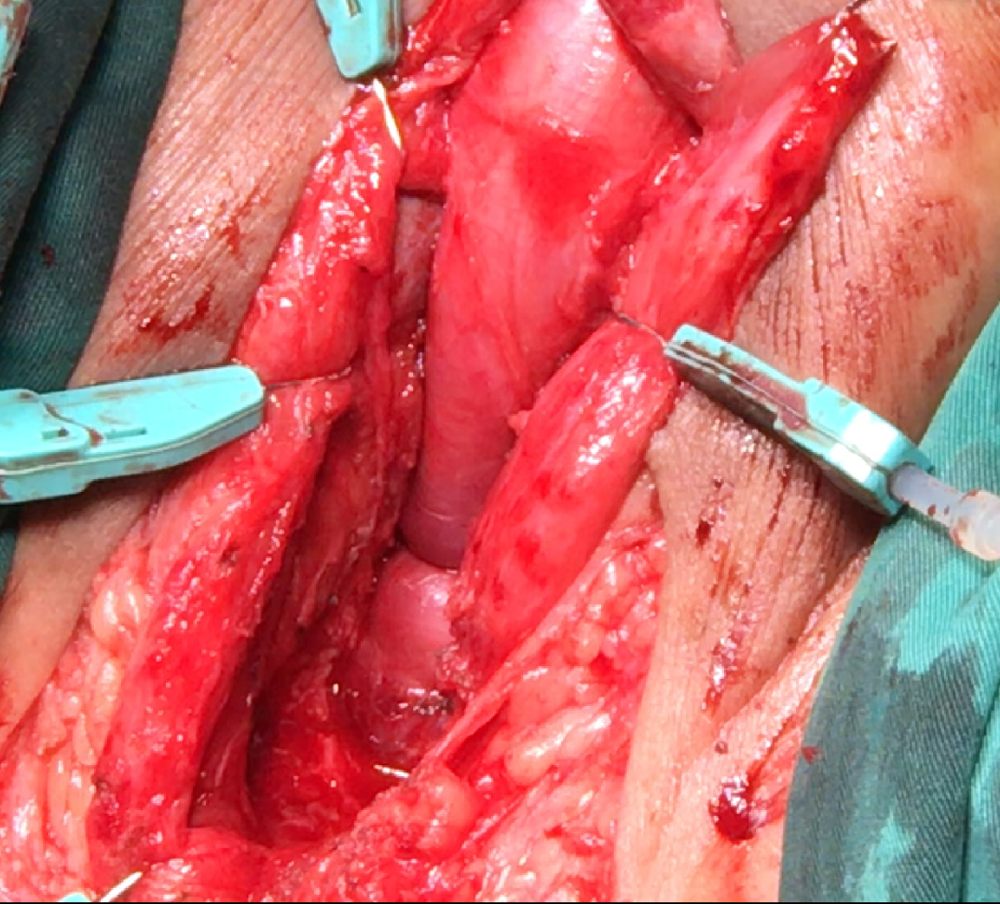
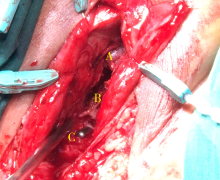
目的: 总结耻骨下缘部分切除技术辅助后尿道吻合术治疗男性骨盆骨折后尿道离断(pelvic fracture urethral distraction defect, PFUDD)的临床效果并分析其技术要点。方法: 回顾性分析采用耻骨下缘部分切除技术辅助后尿道吻合术治疗的男性PFUDD患者63例,患者均以以下步骤完成后尿道吻合:(1)充分游离尿道海绵体球部,在尿道闭锁处切断尿道并切除瘢痕;(2)向远端适当游离尿道海绵体,劈开阴茎海绵体纵隔;(3)切除耻骨联合下缘,完成无张力吻合。结果: 63例患者的平均年龄(39.2±15.6)岁(15~72岁),平均尿道狭窄长度(3.85±0.91) cm (1.5~5.5 cm), 均采用耻骨下缘切除技术辅助完成后尿道吻合,手术时间平均为(160.2±28.1) min (110~210 min),术中估计失血量为(261.1±130.3) mL (100~800 mL),术后或术中输血者3例(4.8%)。术后并发症包括出血和泌尿系感染,均对症处理后治愈。患者的中位随访时间为23个月(12~37个月),术后平均最大尿流率为(23.7±7.4) mL/s (15.0~48.2 mL/s)。耻骨下缘切除技术辅助后尿道吻合治疗男性PFUDD的手术成功率为95.2%(60/63例)。结论: 耻骨下缘部分切除能够有效缩短远近端尿道间距离,辅助部分复杂PFUDD患者完成无张力吻合,技术要点包括阴茎海绵体纵隔切开充分暴露耻骨联合、游离结扎阴茎背静脉、充分切除耻骨骨质下方与尿道之间瘢痕组织暴露健康尿道近端。
中图分类号:
- R699.6





| [1] |
Xu YM, Song LJ, Wang KI, et al. Changing trends in the causes and management of male urethral stricture disease in China: An observational descriptive study from 13 centers [J]. BJU Int, 2015, 116(6):938-944.
doi: 10.1111/bju.12945 |
| [2] | 满立波, 王建伟. 图解尿道成形术[M]. 北京: 人民卫生出版社, 2018: 43-49. |
| [3] | Joshi PM, Batra V, Kulkarni SB. Controversies in the management of pelvic fracture urethral distraction defects [J]. Turk J Urol, 2019, 45(1):1-6. |
| [4] |
Horiguchi A. Management of male pelvic fracture urethral injuries: review and current topics [J]. Int J Urol, 2019, 26(6):596-607.
doi: 10.1111/iju.13947 pmid: 30895658 |
| [5] |
Wessells H, Angermeier KW, Elliott S, et al. Male urethral stricture: American Urological Association guideline [J]. J Urol, 2017, 197(1):182-190.
doi: S0022-5347(16)30961-2 pmid: 27497791 |
| [6] |
Horiguchi A, Shinchi M, Masunaga A, et al. Do transurethral treatment increase the complexity of urethral stricture? [J]. J Urol, 2018, 199(2):508-514.
doi: S0022-5347(17)77417-4 pmid: 28866464 |
| [7] |
Koraitim MM. Optimising the outcome after anastomotic posterior urethroplasty [J]. Arab J Urol, 2015, 13(1):27-31.
doi: 10.1016/j.aju.2014.12.006 |
| [8] |
Andrich DE, Malley KJO, Summerton DJ, et al. The type of urethroplasty for pelvic fracture urethral distraction defect cannot be predicted preoperatively [J]. J Urol, 2003, 170(2 Pt 1):464-467.
doi: 10.1097/01.ju.0000076752.32199.40 |
| [9] |
Horiguchi A, Edo H, Soga S, et al. Pubourethral stump angle measured on preoperative magnetic resonance imaging predeicts urethroplasty type for pelvic fracture injury repair [J]. Urology, 2018, 112:198-204.
doi: S0090-4295(17)31199-8 pmid: 29158171 |
| [10] | Joshi PM, Desai DJ, Shah D, et al. Magnetic resonance imaging procedure for pelvic fracture urethral injuries and recto urethral fistulas: A simple protocaol [J]. Turk J Urol, 2021, 47(1):35-42. |
| [11] |
Yin L, Li Z, Kong C, et al. Urethral pull-through operation for the management of pelvic fracture urethral distraction defects [J]. Urology, 2011, 78(4):946-950.
doi: 10.1016/j.urology.2011.05.027 |
| [12] |
Kulkarni SB, Joshi PM, Hunter C, et al. Complex posterior urethral injury [J]. Arab J Urol, 2015, 13(1):43-52.
doi: 10.1016/j.aju.2014.11.008 |
| [13] | 王建伟, 满立波, 徐啸, 等. 耻骨会阴联合切口后尿道吻合术治疗复杂男性骨盆骨折后尿道离断 [J]. 北京大学学报(医学版), 2020, 52(4):646-650. |
| [14] | 王建伟, 满立波, 黄广林, 等. 经会阴三步法手术策略治疗单纯性男性骨盆骨折后尿道离断 [J]. 北京大学学报(医学版), 2018, 50(4):617-620. |
| [15] |
Saini DK, Sinha RJ, Solhal AK, et al. Analysis of anastomotic urethroplasty for pelvic fracture urethral distraction defect: Decadal experience from a high-volume tertiary care center [J]. Urol Ann, 2019, 11(1):77-82.
doi: 10.4103/UA.UA_48_17 |
| [16] |
Webster GD, Peterson AC. Simple perineal and elaborated peri-neal posterior urethroplasty [J]. Arab J Urol, 2015, 13(1):17-23.
doi: 10.1016/j.aju.2015.01.002 |
| [17] |
Johnsen NV, Moses RA, Elliott SP, et al. Multicenter analysis of posterior urethroplasty complexity and outcomes following pelvic fracture urethral injury [J]. World J Urol, 2020, 38(4):1073-1079.
doi: 10.1007/s00345-019-02824-5 pmid: 31144093 |
| [18] | Ríosa E, Martínez-Piñeirob L. Treatment of posterior urethral distractions defects following pelvic fracture [J]. Asian J Urol, 2018, 5(3):164-171. |
| [1] | 冷汶远, 高端, 李晓宇, 左炜, 胡伟民, 朱振鹏, 徐纯如, 林健, 李学松. 口腔黏膜补片与脱细胞真皮基质补片治疗长段尿道狭窄的疗效和安全性对比[J]. 北京大学学报(医学版), 2025, 57(5): 975-979. |
| [2] | 刘振华,王建伟,黄广林,李贵忠,满立波. 尿道狭窄患者术前菌尿的病原菌分布及危险因素分析[J]. 北京大学学报(医学版), 2023, 55(5): 943-947. |
| [3] | 王建伟,满立波,徐啸,刘振华,何峰,黄广林,翟建坡,周宁,李玮. 耻骨会阴联合切口后尿道吻合术治疗复杂男性骨盆骨折后尿道离断[J]. 北京大学学报(医学版), 2020, 52(4): 646-650. |
| [4] | 王建伟,满立波,黄广林,何峰,王海,王海东,徐啸,李伟,翟建坡,刘振华. 口腔黏膜背侧移植结合阴茎带蒂皮瓣腹侧覆盖治疗阴茎部尿道狭窄[J]. 北京大学学报(医学版), 2019, 51(4): 641-645. |
| [5] | 王建伟,满立波,黄广林,王海,徐啸,朱晓斐,李玮,刘振华. 经会阴三步法手术策略治疗单纯性男性骨盆骨折后尿道离断[J]. 北京大学学报(医学版), 2018, 50(4): 617-620. |
| [6] | 谢天朋, 黄晓波, 许清泉, 叶海云, 杨庆亚, 王晓峰. B超监测下球囊扩张治疗尿道狭窄5例[J]. 北京大学学报(医学版), 2014, 46(4): 657-658. |
| [7] | 黄广林, 满立波, 王海, 王建伟, 翟建坡, 朱晓斐, 周宁, 徐啸. 使用尿道旋切刀治疗女性尿道闭锁[J]. 北京大学学报(医学版), 2014, 46(4): 574-577. |
|
||
