北京大学学报(医学版) ›› 2023, Vol. 55 ›› Issue (6): 958-965. doi: 10.19723/j.issn.1671-167X.2023.06.002
抗Jo-1抗体在特发性炎性肌病临床分层及疾病谱中的意义
李嘉辰1,赖展鸿1,邵苗1,金月波1,高小娟2,张科3,侯儆4,张燕英5,栗占国1,*( ),李玉慧1,*()
),李玉慧1,*()
- 1. 北京大学人民医院风湿免疫科, 北京 100044
2. 宁德师范学院附属宁德市医院风湿免疫科, 福建宁德 352199
3. 中国人民解放军第80集团军医院内分泌科, 山东潍坊 261000
4. 张家口市第一医院肾内科, 河北张家口 075041
5. 深圳市中医院风湿病科, 深圳 518033
Significance of anti-Jo-1 antibody's clinical stratification in idiopathic inflammatory myopathy and disease spectrum
Jia-chen LI1,Zhan-hong LAI1,Miao SHAO1,Yue-bo JIN1,Xiao-juan GAO2,Ke ZHANG3,Jing HOU4,Yan-ying ZHANG5,Zhan-guo LI1,*(),Yu-hui LI1,*()
- 1. Department of Rheumatology and Immunology, Peking University People's Hospital, Beijing 100044, China
2. Department of Rheumatology and Immunology, Ningde Hospital Affiliated to Ningde Normal University, Ningde 352199, Fujian, China
3. Department of Endocrinology, 80th Group Army Hospital of Chinese PLA, Weifang 261000, Shandong, China
4. Department of Nephrology, Zhangjiakou First Hospital, Zhangjiakou 075041, Hebei, China
5. Department of Rheumatology, Shenzhen Hospital of Traditional Chinese Medicine, Shenzhen 518033, China
摘要:
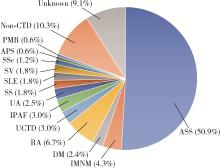
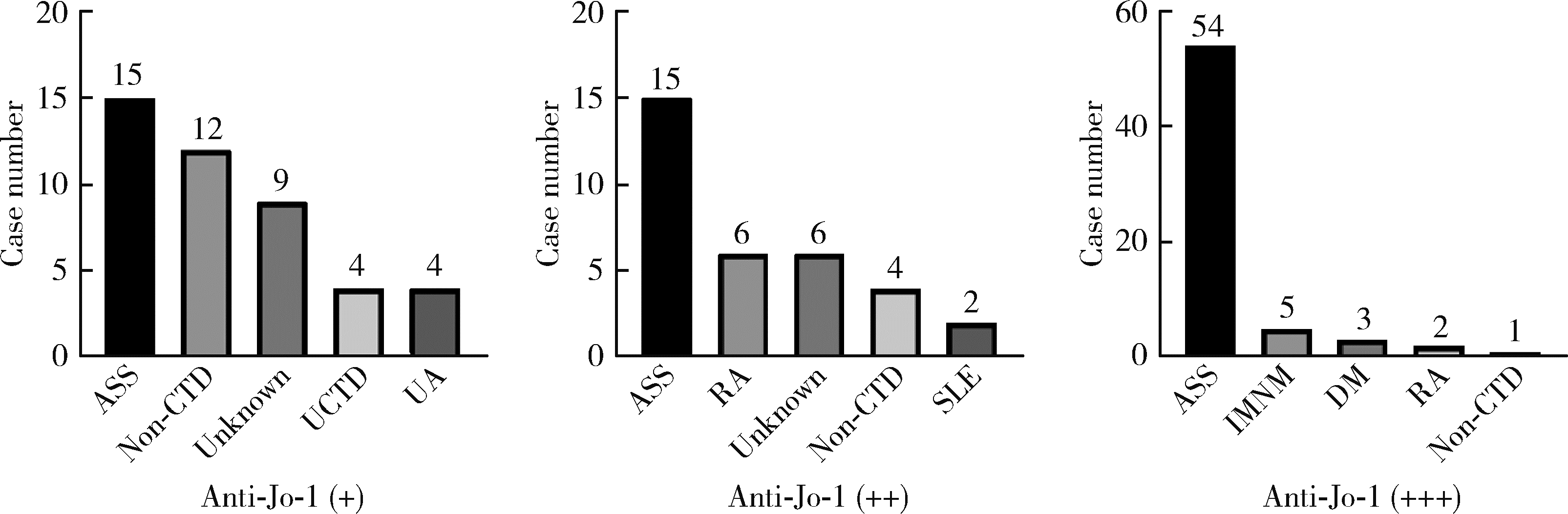
目的: 探究抗组氨酰tRNA合成酶(histidyl tRNA synthetase,Jo-1)抗体在特发性炎性肌病(idiopathic inflammatory myopathies,IIM)及其他疾病谱的意义。方法: 入组北京大学人民医院2016—2022年利用免疫印迹法检测抗Jo-1抗体阳性的患者,同时入组抗Jo-1抗体阴性的抗合成酶综合征(anti-synthetase syndrome,ASS)患者作为对照,分析患者的基本信息、临床特征以及炎症和免疫学指标。结果: 共入组165例抗Jo-1抗体阳性患者,结缔组织病(connective tissue disease,CTD)占80.6%(133/165),其中IIM占总数的57.6%(95/165),包括ASS(84/165,50.9%)、免疫介导坏死性肌病(7/165,4.2%)以及皮肌炎(4/165,2.4%),其他CTD占23.0%(38/165),包括类风湿关节炎(11/165,6.7%)、未分化结缔组织病(5/165, 3.0%)、具有自身免疫特征的间质性肺炎(5/165,3.0%)、未分化关节炎(4/165,2.4%)、干燥综合征(3/165,1.8%)、系统性红斑狼疮(3/165,1.8%)和系统性血管炎(3/165,1.8%)等;其他疾病包括恶性肿瘤(3/165,1.8%)和感染(4/165,2.4%)等;未明确诊断患者占9.1%(15/165)。在ASS亚组分析中,抗Jo-1抗体阳性的ASS患者相比于抗体阴性者起病年龄更低(49.9岁vs. 55.0岁,P=0.026),更多表现为关节炎(60.7% vs. 33.3%,P=0.002)和肌痛(47.1% vs. 22.2%,P=0.004)。ASS患者随着抗Jo-1抗体滴度的升高,关节炎、技工手、Gottron征、雷诺现象(Raynaud phenomenon)以及肌酸激酶、α-羟丁酸脱氢酶指标异常的发生率升高。抗Jo-1抗体阳性ASS患者在合并一种以上其他肌炎抗体阳性时,肌痛、肌无力的发生率升高(P < 0.05)。结论: 抗Jo-1抗体阳性患者疾病谱广,以ASS为主,但也可见于其他CTD、肿瘤、感染等疾病,应注意鉴别。
中图分类号:
- R593.2




| 1 |
Tanboon J , Nishino I . Classification of idiopathic inflammatory myopathies: Pathology perspectives[J]. Curr Opin Neurol, 2019, 32 (5): 704- 714.
doi: 10.1097/WCO.0000000000000740 |
| 2 |
Galindo-Feria AS , Horuluoglu B , Lundberg IE . Anti-Jo 1 autoantibodies, from clinic to the bench[J]. Rheumatology and Autoimmnity, 2022, 2 (2): 57- 68.
doi: 10.1002/rai2.12035 |
| 3 | García-De La Torre I . Clinical usefulness of autoantibodies in idiopathic inflammatory myositis[J]. Front Immunol, 2015, 6, 331. |
| 4 |
Ceribelli A , De Santis M , Isailovic N , et al. The immune response and the pathogenesis of idiopathic inflammatory myositis: A critical review[J]. Clin Rev Allergy Immunol, 2017, 52 (1): 58- 70.
doi: 10.1007/s12016-016-8527-x |
| 5 |
Zhan X , Yan W , Wang Y , et al. Clinical features of anti-synthetase syndrome associated interstitial lung disease: A retrospective cohort in China[J]. BMC Pulm Med, 2021, 21 (1): 57.
doi: 10.1186/s12890-021-01399-5 |
| 6 |
Fredi M , Cavazzana I , Quinzanini M , et al. Rare autoantibodies to cellular antigens in systemic lupus erythematosus[J]. Lupus, 2014, 23 (7): 672- 677.
doi: 10.1177/0961203314524850 |
| 7 |
Kumar RR , Jha S , Dhooria A , et al. Anti-Jo-1 syndrome often misdiagnosed as rheumatoid arthritis (for many years): A single-center experience[J]. J Clin Rheumatol, 2021, 27 (4): 150- 155.
doi: 10.1097/RHU.0000000000001234 |
| 8 |
Ishikawa Y , Yukawa N , Ohmura K , et al. Etanercept-induced anti-Jo-1-antibody-positive polymyositis in a patient with rheumatoid arthritis: A case report and review of the literature[J]. Clin Rheumatol, 2010, 29 (5): 563- 566.
doi: 10.1007/s10067-009-1370-1 |
| 9 |
Eriksson C , Rantapää-Dahlqvist S . Cytokines in relation to autoantibodies before onset of symptoms for systemic lupus erythematosus[J]. Lupus, 2014, 23 (7): 691- 696.
doi: 10.1177/0961203314523869 |
| 10 | 赵娜, 刘颖, 孙小凤, 等. 不同抗氨酰tRNA合成酶抗体阳性的抗合成酶综合征60例临床和影像学相关特征分析[J]. 中华风湿病学杂志, 2019, 23 (5): 320- 325. |
| 11 |
Adams RA , Fernandes-Cerqueira C , Notarnicola A , et al. Serum-circulating His-tRNA synthetase inhibits organ-targeted immune responses[J]. Cell Mol Immunol, 2021, 18 (6): 1463- 1475.
doi: 10.1038/s41423-019-0331-0 |
| 12 |
Honda M , Shimizu F , Sato R , et al. Jo-1 antibodies from myositis induce complement-dependent cytotoxicity and TREM-1 upregulation in muscle endothelial cells[J]. Neurol Neuroimmunol Neuroinflamm, 2023, 10 (4): e200116.
doi: 10.1212/NXI.0000000000200116 |
| 13 |
Cavagna L , Nuño L , Scirè CA , et al. Clinical spectrum time course in anti Jo-1 positive antisynthetase syndrome: Results from an international retrospective multicenter study[J]. Medicine (Baltimore), 2015, 94 (32): e1144.
doi: 10.1097/MD.0000000000001144 |
| 14 |
Monti S , Montecucco C , Cavagna L . Clinical spectrum of anti-Jo-1-associated disease[J]. Curr Opin Rheumatol, 2017, 29 (6): 612- 617.
doi: 10.1097/BOR.0000000000000434 |
| 15 |
Lundberg IE , Tjärnlund A , Bottai M , et al. 2017 European League Against Rheumatism/American College of Rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups[J]. Ann Rheum Dis, 2017, 76 (12): 1955- 1964.
doi: 10.1136/annrheumdis-2017-211468 |
| 16 |
Solomon J , Swigris JJ , Brown KK . Myositis-related interstitial lung disease and antisynthetase syndrome[J]. J Bras Pneumol, 2011, 37 (1): 100- 109.
doi: 10.1590/S1806-37132011000100015 |
| 17 |
Allenbach Y , Mammen AL , Benveniste O , et al. 224th ENMC international workshop: Clinico-sero-pathological classification of immune-mediated necrotizing myopathies Zandvoort, The Netherlands, 14-16 October 2016[J]. Neuromuscul Disord, 2018, 28 (1): 87- 99.
doi: 10.1016/j.nmd.2017.09.016 |
| 18 |
Mielnik P , Wiesik-Szewczyk E , Olesinska M , et al. Clinical features and prognosis of patients with idiopathic inflammatory myo-pathies and anti-Jo-1 antibodies[J]. Autoimmunity, 2006, 39 (3): 243- 247.
doi: 10.1080/08916930600623767 |
| 19 |
Aggarwal R , Cassidy E , Fertig N , et al. Patients with non-Jo-1 anti-tRNA-synthetase autoantibodies have worse survival than Jo-1 positive patients[J]. Ann Rheum Dis, 2014, 73 (1): 227- 232.
doi: 10.1136/annrheumdis-2012-201800 |
| 20 |
Ge YP , Zhang YL , Shu XM , et al. Clinical characteristics of anti-isoleucyl-tRNA synthetase antibody associated syndrome and comparison with different patient cohorts[J]. Clin Exp Rheumatol, 2022, 40 (3): 625- 630.
doi: 10.55563/clinexprheumatol/v2rbd0 |
| 21 |
Satoh M , Tanaka S , Ceribelli A , et al. A comprehensive overview on myositis-specific antibodies: New and old biomarkers in idiopathic inflammatory myopathy[J]. Clin Rev Allergy Immunol, 2017, 52 (1): 1- 19.
doi: 10.1007/s12016-015-8510-y |
| 22 |
Liu Y , Luo H , Wang L , et al. Increased serum matrix metalloproteinase-9 levels are associated with anti-Jo1 but not anti-MDA5 in myositis patients[J]. Aging Dis, 2019, 10 (4): 746- 755.
doi: 10.14336/AD.2018.1120 |
| 23 |
Zhao L , Su K , Liu T , et al. Myositis-specific autoantibodies in adults with idiopathic inflammatory myopathy: Correlations with diagnosis and disease activity[J]. Clin Rheumatol, 2021, 40 (3): 1009- 1016.
doi: 10.1007/s10067-020-05273-3 |
| 24 |
Zhang S , Shu X , Tian X , et al. Enhanced formation and impaired degradation of neutrophil extracellular traps in dermatomyositis and polymyositis: A potential contributor to interstitial lung disease complications[J]. Clin Exp Immunol, 2014, 177 (1): 134- 141.
doi: 10.1111/cei.12319 |
| 25 |
Kryštůfková O , Hulejová H , Mann HF , et al. Serum levels of B-cell activating factor of the TNF family (BAFF) correlate with anti-Jo-1 autoantibodies levels and disease activity in patients with anti-Jo-1positive polymyositis and dermatomyositis[J]. Arthritis Res Ther, 2018, 20 (1): 158.
doi: 10.1186/s13075-018-1650-8 |
| 26 |
Ascherman DP , Oriss TB , Oddis CV , et al. Critical requirement for professional APCs in eliciting T cell responses to novel fragments of histidyl-tRNA synthetase (Jo-1) in Jo-1 antibody-positive polymyositis[J]. J Immunol, 2002, 169 (12): 7127- 7134.
doi: 10.4049/jimmunol.169.12.7127 |
| 27 |
Oldroyd AGS , Allard AB , Callen JP , et al. A systematic review and meta-analysis to inform cancer screening guidelines in idiopathic inflammatory myopathies[J]. Rheumatology (Oxford), 2021, 60 (6): 2615- 2628.
doi: 10.1093/rheumatology/keab166 |
| 28 | 郑艺明, 郝洪军, 刘怡琳, 等. Ro52抗体与其他肌炎抗体共阳性的相关性研究[J]. 北京大学学报(医学版), 2020, 52 (6): 1088- 1092. |
| 29 |
Marie I , Hatron PY , Dominique S , et al. Short-term and long-term outcome of anti-Jo1-positive patients with anti-Ro52 antibody[J]. Semin Arthritis Rheum, 2012, 41 (6): 890- 899.
doi: 10.1016/j.semarthrit.2011.09.008 |
| [1] | 兰静雯, 陈哲, 程永静, 赵丽珂. 老年结缔组织病相关间质性肺病临床特征及抗纤维化治疗的疗效和安全性[J]. 北京大学学报(医学版), 2025, 57(6): 1101-1106. |
| [2] | 练益瑞, 刘静璇, 赵亮, 赵静, 臧思田, 李玉慧. 抗PM/Scl抗体相关风湿性疾病谱及其在特发性炎性肌病中的免疫学特征[J]. 北京大学学报(医学版), 2025, 57(6): 1018-1023. |
| [3] | 朱玉静, 王磊, 吕成银, 谈文峰, 张缪佳. 抗EJ抗体阳性抗合成酶综合征相关间质性肺疾病复发的临床特征分析[J]. 北京大学学报(医学版), 2024, 56(6): 980-986. |
| [4] | 赵亮, 史成龙, 马柯, 赵静, 王潇, 邢晓燕, 莫万星, 练益瑞, 高超, 李玉慧. 抗合成酶综合征重叠类风湿关节炎患者的免疫学特征[J]. 北京大学学报(医学版), 2024, 56(6): 972-979. |
| [5] | 游芳凝,罗靓,刘香君,张学武,李春. 未分化结缔组织病患者的妊娠结局、疾病演变及其影响因素[J]. 北京大学学报(医学版), 2023, 55(6): 1045-1052. |
| [6] | 罗澜,邢晓燕,肖云抒,陈珂彦,朱冯赟智,张学武,李玉慧. 抗合成酶综合征合并心脏受累患者的临床及免疫学特征[J]. 北京大学学报(医学版), 2021, 53(6): 1078-1082. |
| [7] | 魏士雄,黎苏佳,刘毅. 幼年特发性关节炎成人后的临床特点及生物制剂治疗[J]. 北京大学学报(医学版), 2020, 52(6): 1014-1022. |
| [8] | 姚海红,王旖旎,张霞,赵金霞,贾园,王昭,栗占国. 67例成人巨噬细胞活化综合征的临床特征及治疗转归[J]. 北京大学学报(医学版), 2019, 51(6): 996-1002. |
| [9] | 王永福,刘媛. 自身抗体在肿瘤及感染性疾病发生、发展中的作用[J]. 北京大学学报(医学版), 2018, 50(6): 952-955. |
| [10] | 王昱,周炜,郝燕捷,李光韬,邓雪蓉,赵娟,张卓莉. 跟骨定量超声在筛查结缔组织病患者合并骨质疏松中的应用[J]. 北京大学学报(医学版), 2013, 45(5): 766-769. |
| [11] | 石宇红, 李茹 , 陈适 , 苏茵 , 贾园. 91例混合性结缔组织病患者的临床特点及转归[J]. 北京大学学报(医学版), 2012, 44(2): 270-274. |
| [12] | 邓晓莉, 刘湘源, 赵金霞. 弥漫结缔组织病患者心血管并发症的临床特点分析[J]. 北京大学学报(医学版), 2010, 42(2): 143-146. |
|
||
