北京大学学报(医学版) ›› 2026, Vol. 58 ›› Issue (3): 624-630. doi: 10.19723/j.issn.1671-167X.2026.03.024
感染性肺炎与免疫相关间质性肺病中淋巴细胞亚群的表达
赵豆豆1,2,*, 齐晅1,3,*, 黄博1, 高伟波4, 裴源源4, 金月波1, 邵苗1, 何菁1,*( )
)
- 1. 北京大学人民医院风湿免疫科, 北京 100044
2. 晋城市人民医院风湿免疫科, 山西晋城 048000
3. 河北医科大学第二医院风湿免疫科, 石家庄 050000
4. 北京大学人民医院急诊科, 北京 100044
Expression and clinical significance of lymphocyte subsets in infectious pneumonia and immune-related interstitial lung disease
Doudou ZHAO1,2, Xuan QI1,3, Bo HUANG1, Weibo GAO4, Yuanyuan PEI4, Yuebo JIN1, Miao SHAO1, Jing HE1,*()
- 1. Peking University People's Hospital, Rheumatology and Immunology Department, Beijing 100044, China
2. Jincheng People's Hospital, Rheumatology and Immunology Department, Jincheng 048000, Shanxi, China
3. The Second Hospital of Hebei Medical University, Rheumatology and Immunology Department, Shijiazhuang 050000, China
4. Peking University People's Hospital, Emergency Department, Beijing 100044, China
摘要:
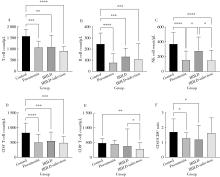
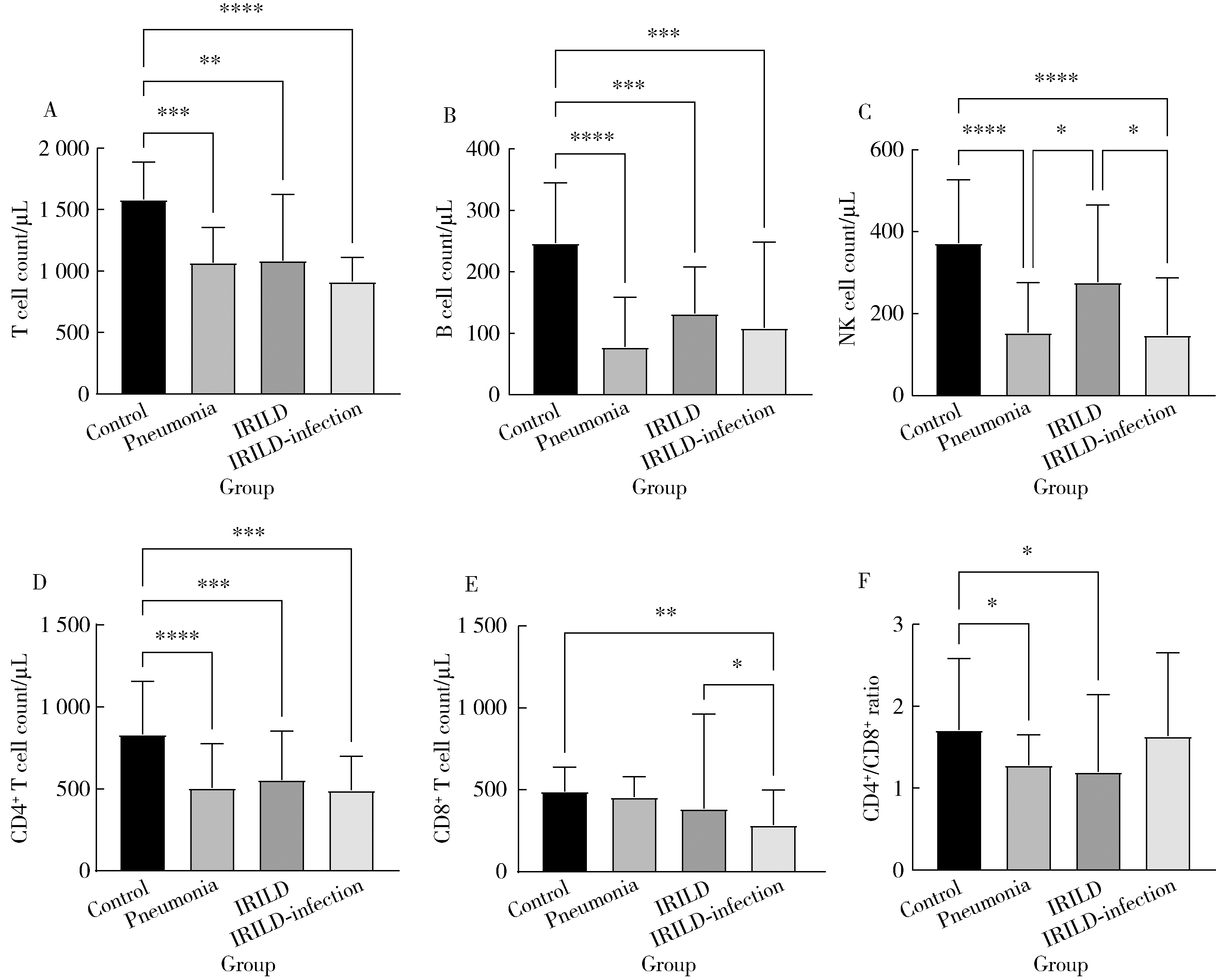
目的: 比较感染性肺炎和免疫相关间质性肺病(immune-related interstitial lung disease, IRILD)患者淋巴细胞亚群表达的差异,评估不同肺炎患者的免疫状态,从免疫学的角度为有效鉴别不同肺炎提供新的实验室指标。方法: 连续纳入2023年1月至2024年3月就诊于北京大学人民医院风湿免疫科的感染性肺炎患者27例、单纯IRILD患者27例以及IRILD合并感染患者24例,并选择同期进行体检的50名健康志愿者作为对照组。采用流式细胞术检测各组淋巴细胞亚群水平。结果: 病例组与对照组间年龄差异无统计学意义(P>0.05)。在实验室指标方面,与IRILD组相比,感染性肺炎组患者中性粒细胞、C反应蛋白、降钙素原(procalcitonin,PCT)、红细胞沉降率(erythrocyte sedimentation rate,ESR)、D-二聚体、纤维蛋白原水平增高(P<0.05),IRILD合并感染组患者PCT、ESR、免疫球蛋白G水平增高(P<0.05)。在淋巴细胞亚群水平方面,与对照组相比,感染性肺炎组患者的T、B、自然杀伤(natural killer,NK)、CD4+T细胞数,CD4+/CD8+比值明显降低(P<0.05),IRILD组患者的T、B,CD4+T细胞数、CD4+/CD8+比值明显降低(P<0.05),IRILD合并感染组患者T、B、NK、CD4+T、CD8+T细胞数明显降低(P<0.05)。与IRILD组患者相比,感染性肺炎组患者NK细胞数明显下降(P<0.05),IRILD合并感染组患者NK、CD8+T细胞数明显降低(P<0.05)。结论: 不同肺炎淋巴细胞亚群水平存在一定差异,为有效鉴别不同肺炎提供了新的思路。
中图分类号:
- R563
| 1 |
doi: 10.3389/fimmu.2023.1119564 |
| 2 |
|
| 3 |
doi: 10.1148/rg.2015140334 |
| 4 |
doi: 10.1183/13993003.00829-2015 |
| 5 |
葛均波, 徐永健, 王辰. 内科学[M]. 9版. 北京: 人民卫生出版社, 2018: 41- 44.
|
| 6 |
中华医学会健康管理学分会. TBNK淋巴细胞检测在健康管理中的应用专家共识[J]. 中华健康管理学杂志, 2023, 17 (2): 85- 95.
|
| 7 |
doi: 10.1002/iid3.1009 |
| 8 |
doi: 10.1080/22221751.2023.2208679 |
| 9 |
doi: 10.1097/MOP.0000000000000357 |
| 10 |
doi: 10.1111/imcb.12611 |
| 11 |
doi: 10.1186/s13075-022-02811-z |
| 12 |
doi: 10.1007/s10753-022-01747-5 |
| 13 |
doi: 10.1016/j.intimp.2019.105912 |
| 14 |
doi: 10.1164/rccm.200812-1936OC |
| 15 |
doi: 10.4049/jimmunol.1900980 |
| 16 |
左艳华, 刘靓, 许化恒, 等. 结缔组织病相关性间质性肺炎患者涎液化糖链抗原与T细胞亚群水平变化及其临床意义[J]. 临床军医杂志, 2021, 49 (3): 336- 337.
|
| 17 |
张晶晶, 陈智勇, 王红, 等. 特发性炎性肌病间质性肺炎患者并发肺部感染的临床特征[J]. 中华风湿病学杂志, 2020, 24 (4): 253- 257.
|
| 18 |
耿陶然, 韩扬, 邱志峰, 等. 重症流行性感冒患者T淋巴细胞与预后研究[J]. 中华内科杂志, 2020, 59 (3): 200- 206.
|
| 19 |
doi: 10.1007/s10067-023-06716-3 |
| 20 |
|
| 21 |
doi: 10.1016/j.rmed.2012.09.021 |
| [1] | 林文灏, 谢阳, 王芳晴, 王淑盈, 刘香君, 胡凡磊, 贾园. 基于B细胞单细胞转录组测序的干燥综合征分子分型[J]. 北京大学学报(医学版), 2025, 57(6): 1032-1041. |
| [2] | 赵亮, 史成龙, 马柯, 赵静, 王潇, 邢晓燕, 莫万星, 练益瑞, 高超, 李玉慧. 抗合成酶综合征重叠类风湿关节炎患者的免疫学特征[J]. 北京大学学报(医学版), 2024, 56(6): 972-979. |
| [3] | 李敏,侯林卿,金月波,何菁. 系统性红斑狼疮合并视网膜病变的临床及免疫学特点[J]. 北京大学学报(医学版), 2022, 54(6): 1106-1111. |
| [4] | 包芳,史尉利,胡静,张娣,高东晗,夏云霞,景红梅,克晓燕,葛庆岗,沈宁. 新型冠状病毒肺炎淋巴细胞亚群与严重程度的相关分析[J]. 北京大学学报(医学版), 2020, 52(6): 1075-1081. |
| [5] | 朱明霞,万文丽,李海申,王晶,王艳芳,胡凯,克晓燕. 造血干细胞移植后的早期免疫重建[J]. 北京大学学报(医学版), 2016, 48(3): 505-522. |
| [6] | 邵彬,李惠平,邸立军,宋国红,姜晗昉,梁旭,王超颖,严颖,林晓琳,王丽娜,宛凤玲,. 外周血淋巴细胞亚群监测对复发转移性乳腺癌的预测及预后价值[J]. 北京大学学报(医学版), 2016, 48(2): 304-309. |
| [7] | 孙佳鹏,卢新天,赵卫红,华瑛. 自身免疫性淋巴细胞增生综合征1例并文献复习[J]. 北京大学学报(医学版), 2015, 47(6): 1022-1027. |
| [8] | 赵翔宇,赵晓甦,王亚哲,常英军,吕萌,王洪涛,韩婷婷,黄晓军. 自然杀伤细胞表面杀伤免疫球蛋白样受体和CD57分子的表达及其功能[J]. 北京大学学报(医学版), 2014, 46(1): 115-119. |
| [9] | 李百花, 张秋香, 董殿军, 林晓明. 番茄红素对急性肺损伤大鼠免疫细胞和炎性细胞因子的影响[J]. 北京大学学报(医学版), 2007, 39(1): 77-82. |
| [10] | 尤鹏, 刘玉兰, 陈国栋. 大鼠肝移植自发免疫耐受模型CD4+CD25+和CD8+CD28-调节性T细胞的变化[J]. 北京大学学报(医学版), 2006, 38(3): 266-270. |
| [11] | . ApoE基因缺陷鼠免疫、血液稳态和抗氧化功能改变[J]. 北京大学学报(医学版), 2001, 33(4): 347-350. |
|
||
