北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (1): 70-74. doi: 10.19723/j.issn.1671-167X.2019.01.013
生物陶瓷材料在乳牙牙髓切断术中的应用
雷玥,杨颖婷,战园( )
)
- 北京大学口腔医学院·口腔医院,第三门诊部 国家口腔疾病临床医学研究中心 口腔数字化医疗技术和材料国家工程实验室 口腔数字医学北京市重点实验室,北京 100083
Evaluation of bioceramic putty repairment in primary molars pulpotomy
Yue LEI,Ying-ting YANG,Yuan ZHAN()
- Third Clinical Division, Peking University School and Hospital of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology, Beijing 100083, China
摘要:
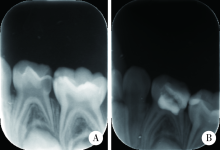
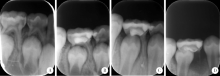
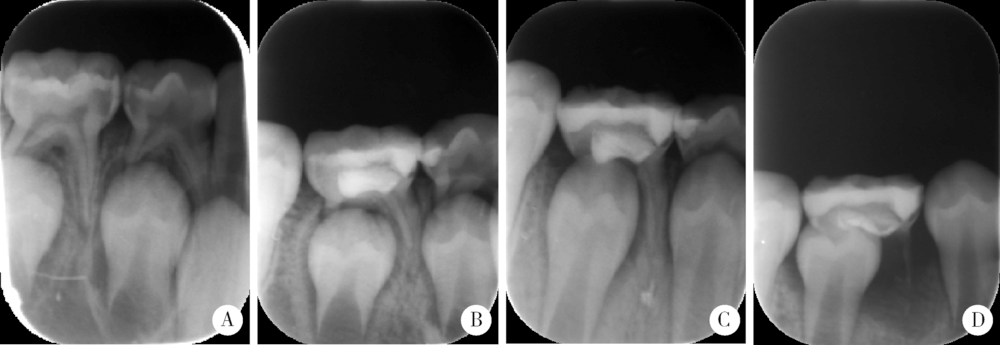
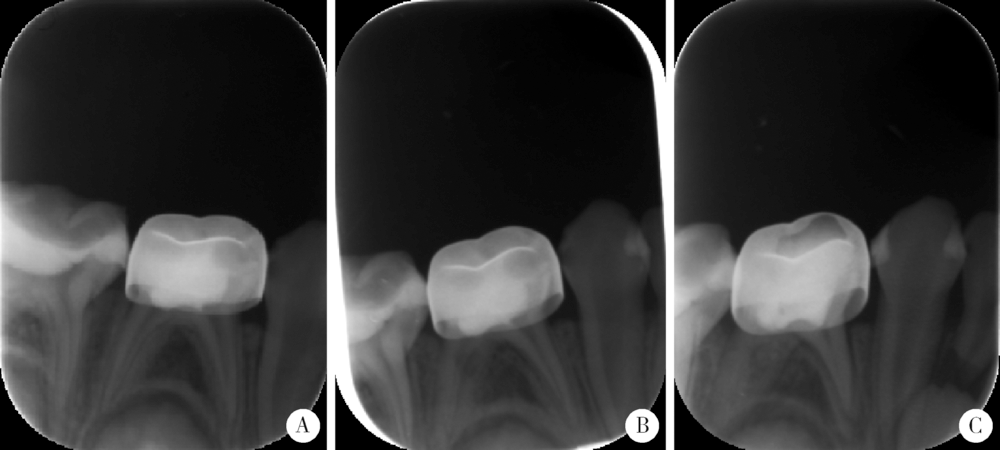
目的:研究生物陶瓷材料(iRoot BP Plus)作为盖髓剂用于乳牙牙髓切断术的临床可操作性和疗效,为临床应用提供参考依据。方法:选择2016年9月至2017年9月到北京大学口腔医院第三门诊部儿科就诊患者,在乳磨牙的牙髓切断术中使用生物陶瓷材料作为盖髓剂,以治疗时间为观察开始时间,以最后一次拍摄X线片的时间为观察终点时间,对患牙进行定期随访观察1年以上,每次复诊时记录患牙的临床检查和X线片检查情况,将患牙预后归为N、H、P0、PX、PY五类,N为临床和X线均未见异常,H为临床未见异常,X线表现为牙根生理性吸收,P0为临床未见异常,X线出现牙髓钙化、牙根吸收等改变,但暂时无需治疗,PX为临床出现或未出现异常,X线出现根尖周病变,需要根管治疗或拔除,PY为乳牙早失;其中N、H定义为成功,P0、PX、PY定义为失败。结果:截至2018年9月,共纳入患牙40颗(患者34人),初诊年龄为3.1~8.5岁,平均(4.7±1.2)岁,观察时间12~24个月(中位时间16个月),患牙预后符合N的牙齿34颗,符合H的2颗,符合P0的1颗,符合PX的3颗,符合PY的0颗。使用生物陶瓷材料作为盖髓剂的乳磨牙牙髓切断术12个月成功率95%。结论:使用生物陶瓷材料作为盖髓剂进行乳牙牙髓切断术取得满意疗效,可以作为盖髓剂用于乳牙牙髓切断术的常规治疗。
中图分类号:
- R781.3



| [1] |
Simancas-Pallares MA, Díaz-Caballero AJ, Luna-Ricardo LM . Mineral trioxide aggregate in primary teeth pulpotomy. A systema-tic literature review[J]. Avances En Odontoestomatología, 2011,27(2):91-98.
doi: 10.4321/S0213-12852011000200005 pmid: 20526246 |
| [2] |
王敏永, 刘鹤, 李盛林 , 等. 三氧化矿物凝聚体对乳、恒牙牙髓细胞增殖和分化影响的比较[J]. 华西口腔医学杂志, 2015,33(1):75-79.
doi: 10.7518/hxkq.2015.01.017 |
| [3] |
Shivani U, RuchikaRoongta N, Sangeeta T , et al. Current perspectives of bio-ceramic technology in endodontics: calcium enriched mixture cement, review of its composition, properties and applications[J]. Restor Dent Endod, 2015,40(1):1-13.
doi: 10.5395/rde.2015.40.1.1 pmid: 4320271 |
| [4] |
de Souza ET, Tameirão N, Roter JM , et al. Tridimensional quantitative porosity characterization of three set calcium silicate-based repair cements for endodontic use[J]. Microsc Res Tech, 2013,76(10):1093-1098.
doi: 10.1002/jemt.22270 pmid: 23913667 |
| [5] |
Jiang Y, Zheng Q, Zhou X , et al. A comparative study on root canal repair materials: a cytocompatibility assessment in L929 and MG63 cells[J]. Sci World J, 2014,2014(12):463826.
doi: 10.1155/2014/463826 pmid: 24526893 |
| [6] |
Ciasca M, Aminoshariae A, Jin G , et al. A comparison of the cytotoxicity and proinflammatory cytokine production of EndoSequence root repair material and ProRoot mineral trioxide aggregate in human osteoblast cell culture using reverse-transcriptase polymerase chain reaction[J]. J Endod, 2012,38(4):486-489.
doi: 10.1016/j.joen.2011.12.004 pmid: 22414834 |
| [7] |
Lovato KF, Sedgley CM . Antibacterial activity of EndoSequence root repair material and ProRoot MTA against clinical isolates of enterococcus faecalis[J]. J Endod, 2011,37(11):1542.
doi: 10.1016/j.joen.2011.06.022 pmid: 22000459 |
| [8] |
Shokouhinejad N, Nekoofar MH, Razmi H , et al. Bioactivity of EndoSequence root repair material and bioaggregate[J]. Int Endod J, 2012,45(12):1127.
doi: 10.1111/j.1365-2591.2012.02083.x pmid: 22803801 |
| [9] | 秦满 . 儿童口腔科诊疗指南与护理常规[M]. 北京: 人民卫生出版社, 2015: 62. |
| [10] |
Casas MJ, Layug MA, Kenny DJ , et al. Two-year outcomes of primary molar ferric sulfate pulpotomy and root canal therapy[J]. Pediatr Dent, 2004,26(1):44-48.
doi: 10.1007/s00246-003-0506-3 pmid: 15080357 |
| [11] | 窦桂丽, 吴南, 赵双云 , 等. 乳磨牙牙髓切断术两年疗效观察及其影响因素回顾性分析[J]. 北京大学学报(医学版), 2018,50(1):170-175. |
| [12] |
Stanley HR . Pulp capping: conserving the dental pulp, can it be done? Is it worth it?[J]. Oral Surgery Oral Medicine Oral Pathology, 1989,68(5):628-639.
doi: 10.1016/0030-4220(89)90252-1 pmid: 2682429 |
| [13] |
Elmeligy O, Abdalla M, Elbaraway S , et al. Histological evaluation of electrosurgery and formocresolpulpotomy techniques in primary teeth in dogs[J]. J Clin Pediatr Dent, 2001,26(1):81-85.
doi: 10.17796/jcpd.26.1.w2243176tj661n8p pmid: 11688819 |
| [14] |
Hunter AR, Kirk EE, Robinson DH , et al. A slow release calcium delivery system for the study of reparative dentine formation[J]. Dent Traumatol, 1998,14(3):112-118.
doi: 10.1111/j.1600-9657.1998.tb00822.x pmid: 9863419 |
| [15] |
Harandi A, Forghani M, Ghoddusi J . Vital pulp therapy with three different pulpotomy agents in immature molars: a case report[J]. Iran Endod J, 2013,8(3):145.
pmid: 3734519 |
| [16] |
Subramaniam P, Konde S, Mathew S , et al. Mineral trioxide aggregate as pulp capping agent for primary teeth pulpotomy: 2 year follow up study[J]. J Clin Pediatr Dent, 2009,33(4):311-314.
doi: 10.1016/j.ijom.2009.01.014 pmid: 19725237 |
| [17] |
Fernández CC, Martínez SS, Jimeno FG , et al. Clinical and radiographic outcomes of the use of four dressing materials in pulpotomized primary molars: a randomized clinical trial with 2-year follow-up[J]. Int J Paediatr Dent, 2013,23(6):400.
doi: 10.1111/ipd.12009 pmid: 23171351 |
| [18] |
Asgary S, Parirokh M, Eghbal MJ , et al. Chemical differences between white and gray mineral trioxide aggregate[J]. J Endod, 2005,31(2):101-103.
doi: 10.1097/01.DON.0000133156.85164.B2 pmid: 15671818 |
| [19] |
Machado J, Johnson JD, Paranjpe A . The effects of endosequence root repair material on differentiation of dental pulp cells[J]. J Endod, 2016,42(1):101.
doi: 10.1016/j.joen.2015.08.007 pmid: 26410154 |
| [20] |
Oncel TZ, Torun D, Demirkaya K , et al. Effects of “iRoot BP” and “white mineral trioxide aggregate” on cell viability and the expression of genes associated with mineralization[J]. Int Endod J, 2015,48(10):986-993.
doi: 10.1111/iej.12393 pmid: 25286824 |
| [21] |
Zhang J, Zhu LX, Cheng X , et al. Promotion of dental pulp cell migration and pulp repair by a bioceramic putty involving FGFR-mediated signaling pathways[J]. J Dent Res, 2015,94(6):853-862.
doi: 10.1177/0022034515572020 pmid: 25724555 |
| [22] |
Shi S, Bao ZF, Liu Y , et al. Comparison of in vivo dental pulp responses to capping with iRoot BP plus and mineral trioxide aggregate[J]. Int Endod J, 2016,49(2):154.
doi: 10.1111/iej.12439 pmid: 25661049 |
| [23] |
Azimi S, Fazlyab M, Sadri D , et al. Comparison of pulp response to mineral trioxide aggregate and a bioceramic paste in partial pulpotomy of sound human premolars: a randomized controlled trial[J]. Int Endod J, 2014,47(9):873-881.
doi: 10.1111/iej.12231 pmid: 24330490 |
| [24] | Hutcheson C, Seale NS, Mcwhorter A , et al. Multi-surface composite vs stainless steel crown restorations after mineral trioxide aggregate pulpotomy: a randomized controlled trial[J]. Pediatr Dent, 2012,34(7):460. |
| [25] |
Dentistry AAOP . Guideline on pulp therapy for primary and young permanent teeth[J]. Pediatr Dent, 2004,26(4):115-119.
pmid: 15656447 |
| [1] | 臧海玲, 梁宇红. 上颌第二磨牙慢性根尖周炎合并器械分离的根管再治疗1例[J]. 北京大学学报(医学版), 2026, 58(1): 214-219. |
| [2] | 杨颖婷, 李若竹, 窦桂丽, 雷玥, 夏斌. iRoot BP Plus用于年轻恒牙外伤部分牙髓切断治疗的临床随机对照研究[J]. 北京大学学报(医学版), 2024, 56(6): 1083-1088. |
| [3] | 郑佳佳,杨雪,温泉,付元,邵校,丁美丽. 生物活性陶瓷iRoot BP Plus®在儿童年轻恒前牙复杂冠折牙髓切断术中的应用[J]. 北京大学学报(医学版), 2024, 56(1): 179-184. |
| [4] | 赵晓一,刘畅,钱锟,潘洁. 成熟恒牙牙髓切断术的疗效及影像学评价[J]. 北京大学学报(医学版), 2024, 56(1): 138-143. |
| [5] | 雍颹,钱锟,朱文昊,赵晓一,刘畅,潘洁. 成年恒牙牙髓切断后牙髓钙化的X线片评价[J]. 北京大学学报(医学版), 2023, 55(1): 88-93. |
| [6] | 王爽,彭楚芳,刘鹤. 新型生物陶瓷材料用于乳磨牙牙髓切断术的临床疗效[J]. 北京大学学报(医学版), 2022, 54(6): 1196-1201. |
| [7] | 钱锟,潘洁,朱文昊,赵晓一,刘畅,雍颹. 两种硅酸钙类材料用于成熟恒牙牙髓切断术的临床效果[J]. 北京大学学报(医学版), 2022, 54(1): 113-118. |
| [8] | 窦桂丽,吴南,赵双云,夏斌. 乳磨牙牙髓切断术两年疗效观察及其影响因素回顾性分析[J]. 北京大学学报(医学版), 2018, 50(1): 170-175. |
| [9] | 战园,刘鹤. 第一乳磨牙与第一前磨牙异位埋伏阻生1例[J]. 北京大学学报(医学版), 2017, 49(1): 181-183. |
| [10] | 郭怡丹,张笋. Er:YAG激光用于比格犬牙髓切断术[J]. 北京大学学报(医学版), 2016, 48(4): 714-719. |
| [11] | 郑佳佳,陈小贤,张笋,葛立宏. 中日两国部分口腔医师乳牙活髓保存诊疗操作现况调查[J]. 北京大学学报(医学版), 2015, 47(6): 1050-1052. |
| [12] | 白洁, 秦满, 姬爱平. Pulpdent Multi-Cal用于年轻恒前牙活髓切断术的临床研究[J]. 北京大学学报(医学版), 2011, 43(6): 882-885. |
|
||
