北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (4): 641-645. doi: 10.19723/j.issn.1671-167X.2019.04.008
口腔黏膜背侧移植结合阴茎带蒂皮瓣腹侧覆盖治疗阴茎部尿道狭窄
王建伟,满立波( ),黄广林,何峰,王海,王海东,徐啸,李伟,翟建坡,刘振华
),黄广林,何峰,王海,王海东,徐啸,李伟,翟建坡,刘振华
- 北京积水潭医院泌尿外科, 北京大学第四临床医学院, 北京 100096
Single-stage repair of penile urethral stricture using combined dorsal onlay oral mucosa grafting with ventral onlay penile skin flap
Jian-wei WANG,Li-bo MAN(),Guang-lin HUANG,Feng HE,Hai WANG,Hai-dong WANG,Xiao XU,Wei LI,Jian-po ZHAI,Zhen-hua LIU
- Department of Urology, Beijing Jishuitan Hospital, The Fourth Medical College of Peking University, Beijing 100096, China
摘要:
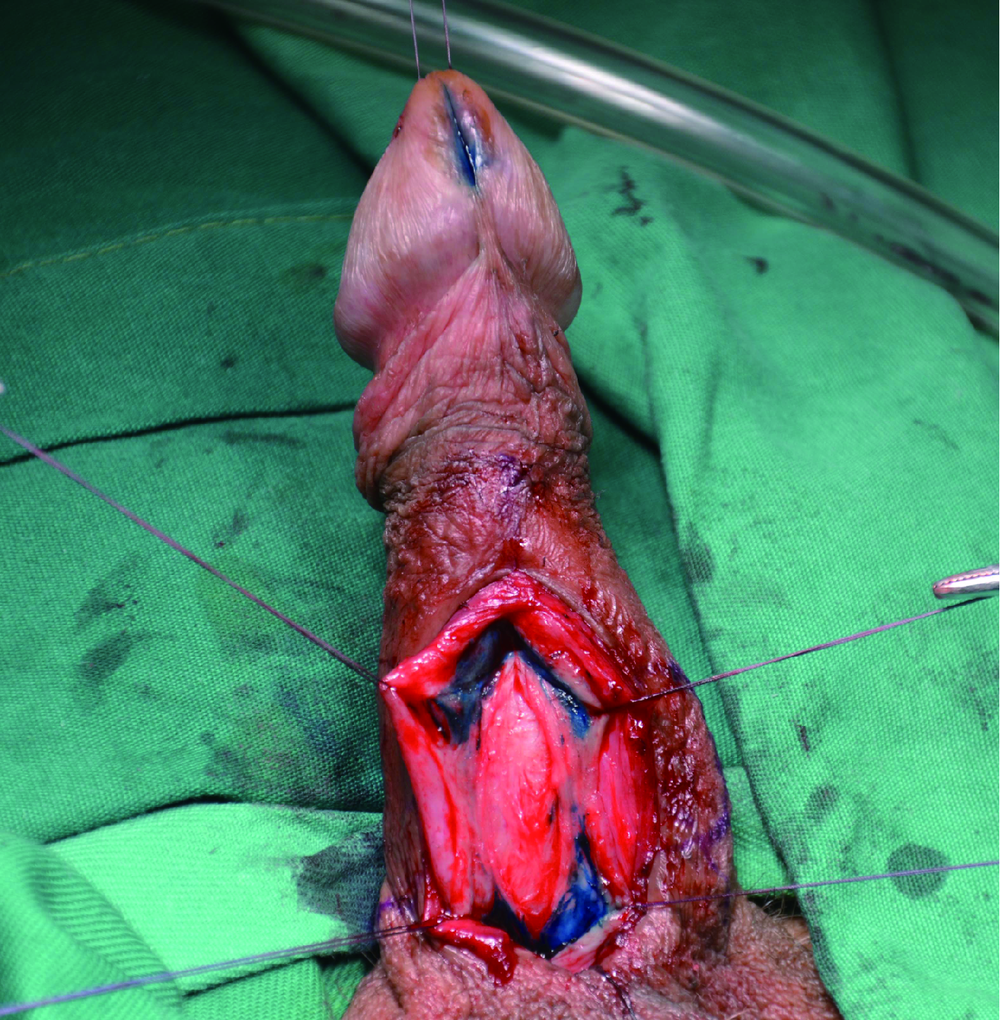
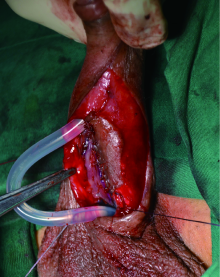
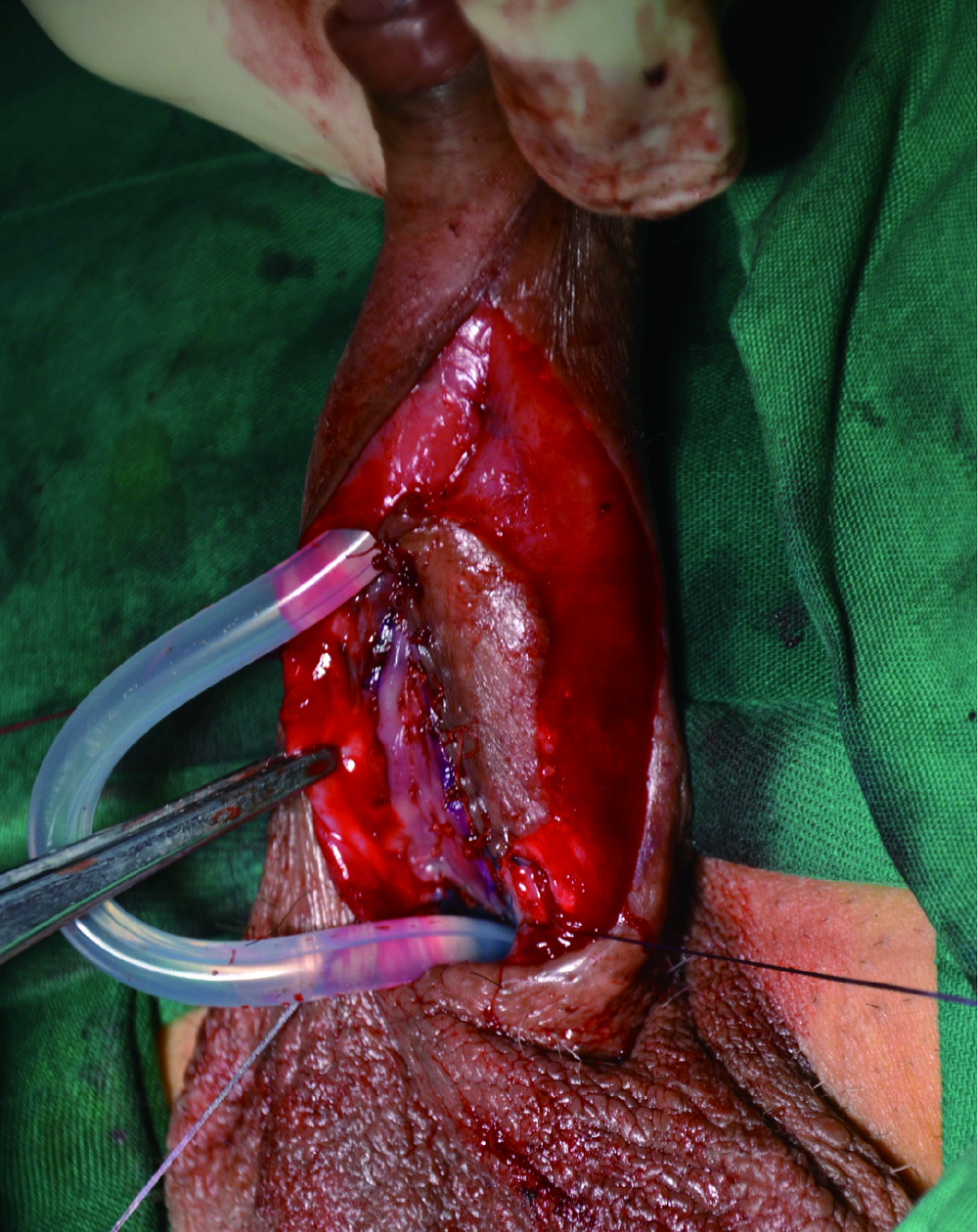
目的:总结口腔黏膜背侧游离移植结合阴茎带蒂皮瓣腹侧覆盖尿道扩大成形术治疗阴茎部尿道狭窄的临床效果及经验。方法:选择北京积水潭医院泌尿外科2015年11月至2018年10月采用口腔黏膜背侧游离移植结合阴茎带蒂皮瓣腹侧覆盖尿道扩大成形术治疗阴茎部尿道狭窄患者22例的病例资料进行回顾性分析。所有患者均无术前尿瘘等合并症,均为单纯性单处阴茎部尿道狭窄,其中医源性狭窄14例(63.6%)、感染性狭窄2例(9.1%)、特发性狭窄6例(27.3%)。术中均从腹侧纵行切开尿道狭窄段,先采用游离口腔黏膜做狭窄段背侧嵌式修补,腹侧采用纵行阴茎带蒂皮瓣(Orandi皮瓣)覆盖修补,留置16F或14F硅胶尿管,3周后拔除尿管并行尿道造影及膀胱镜检查。术后最大尿流率≥15 mL/s且不需要尿道扩张等外科干预可视为手术成功。结果:本组患者年龄平均52.6(18~73)岁。患者尿道狭窄均位于前尿道阴茎部,长度平均5.3(2.5~10.0) cm,术前平均最大尿流率6.7 mL/s。口腔黏膜取材长度平均5.5(3.2~10.5) cm,阴茎皮瓣长度平均6.0(3.5~11.0) cm。手术时间平均225(150~420) min,术中平均估计失血量53(20.0~110.0) mL。采用颊黏膜19例(86.4%), 舌黏膜3例(13.6%),其中双侧颊黏膜取材5例(22.7%)。平均随访20.5(5~51)个月,术后6个月平均最大尿流率21.2(15~32) mL/s。术后尿瘘形成1例、再狭窄2例,手术成功率为81.8%(18/22), 2例再狭窄患者1例再次行尿道成形术后治愈,另1例行定期尿道扩张治疗。术后感染2例,表现为尿道口脓液溢出、阴茎肿胀,对症处理后治愈。局部皮肤坏死1例,给予保守治疗成功。尿瘘患者行瘘修补术后治愈。结论:口腔黏膜背侧游离移植结合阴茎带蒂皮瓣腹侧覆盖尿道扩大成形术治疗阴茎部尿道狭窄22例平均随访20.5个月,手术成功率为81.8%,临床效果明确,适用于严重前尿道阴茎部狭窄且局部阴茎皮肤状况良好的患者。
中图分类号:
- R699









| [1] | McAninch JW, Morey AF . Penile circular fasciocutaneous skin flap in 1-stage reconstruction of complex anterior urethral strictures[J]. J Urol, 1998,159(4):1209-1213. |
| [2] | Morey AF . Urethral plate salvage with dorsal graft promotes successful penile flaponlay reconstruction of severe pendulous strictures[J]. J Urol, 2001,166(4):1376-1378. |
| [3] | Bayne DB, Gaither TW, Awad MA , et al. Guidelines of guidelines: a review of urethral stricture evaluation, management, and follow-up[J]. Transl Androl Urol, 2017,6(2):288-294. |
| [4] | Horiguchi A . Substitution urethroplasty using oral mucosa graft for male anterior urethral stricture disease: current topics and reviews[J]. Int J Urol, 2017,24(7):493-503. |
| [5] | Erickson BA, Breyer BN , McAninch JW. Single-stage segmental urethral replacement using combined ventral onlay fasciocutaneous flap with dorsal onlay buccal grafting for long segment strictures[J]. BJU Int, 2012,109(9):1392-1396. |
| [6] | Greenwell TJ, Venn AF, Mundy AR . Changing practice in anteriorurethroplasty[J]. BJU Int, 1999,83(6):631-635. |
| [7] | Wessells H, Angermeier KW, Elliott S , et al. Male urethral stricture: American Urological Association Guideline[J]. J Urol, 2017,197(1):182-190. |
| [8] | Gelman J, Sohn W . 1-stage repair of obliterative distal urethral strictures with buccal graft urethral plate reconstruction and simultaneous onlay penile skin flap[J]. J Urol, 2011,186(3):935-938. |
| [9] | Djordjevic ML, Majstorovic M, Stanojevic D , et al. Combined buccal mucosa graft and dorsal penile skin flap for repair of severe hypospadias[J]. Urology, 2008,71(5):821-825. |
| [10] | Soliman MG, Abo Farha MA, El Abd AS , et al. Dorsal onlay urethroplasty using buccal mucosa graft versus penile skin flap for management of long anterior urethral strictures: a prospective randomized study[J]. Scand J Urol, 2014,48(5):466-473. |
| [11] | 满立波, 王建伟 . 图解尿道成形术[M]. 北京: 人民卫生出版社, 2018: 52-59. |
| [1] | 池彦廷, 蒋鸿杰, 陈艳, 徐志秀, 李斌斌. 直接免疫荧光在口腔黏膜寻常型天疱疮诊断中的价值: 基于多指标联合分析的回顾性研究[J]. 北京大学学报(医学版), 2026, 58(1): 68-73. |
| [2] | 冷汶远, 高端, 李晓宇, 左炜, 胡伟民, 朱振鹏, 徐纯如, 林健, 李学松. 口腔黏膜补片与脱细胞真皮基质补片治疗长段尿道狭窄的疗效和安全性对比[J]. 北京大学学报(医学版), 2025, 57(5): 975-979. |
| [3] | 朱慧, 闵赛南, 苏家增, 陈艳, 彭歆, 于尧, 俞光岩. 口腔黏膜嗜酸性溃疡的临床病理分析[J]. 北京大学学报(医学版), 2025, 57(3): 620-625. |
| [4] | 王鹃, 邱立新, 尉华杰. 下颌磨牙穿龈形态设计对种植体周围软组织影响的随机对照临床研究[J]. 北京大学学报(医学版), 2025, 57(1): 65-72. |
| [5] | 王杰, 王建伟, 夏海缀, 徐啸, 翟建坡, 何峰, 黄广林, 李贵忠. 阴茎远端尿道狭窄疾病的手术治疗方式[J]. 北京大学学报(医学版), 2024, 56(6): 1075-1082. |
| [6] | 周培茹, 蒋析, 华红. 口腔黏膜病患者口腔种植的时机及注意事项[J]. 北京大学学报(医学版), 2021, 53(1): 5-8. |
| [7] | 王莺, Obada Barry, Gerhard Wahl, 陈波,林野. 应用激光多普勒血流仪监测口腔黏膜血流[J]. 北京大学学报(医学版), 2016, 48(4): 697-701. |
| [8] | 丁宁, 闫志敏, 华红. 实时荧光定量PCR法检测原发性Sjögren综合征口腔真菌菌群[J]. 北京大学学报(医学版), 2013, 45(1): 17-21. |
| [9] | 曹婕*, 刘宏伟, 刘晓松, 金建秋, 张平. 口腔黏膜微核细胞数与上皮异常增生病损癌变的关系[J]. 北京大学学报(医学版), 2011, 43(4): 600-602. |
| [10] | 林野, 邱立新, 胡秀莲, 王莺, 李健慧. 硬腭游离黏膜移植在种植体周软组织结构重建中的应用[J]. 北京大学学报(医学版), 2007, 39(1): 21-25. |
| [11] | 杨天智, 陈大兵, 张强. 不同吸收促进剂及酶抑制剂对胰岛素体内及体外口腔黏膜渗透性的影响[J]. 北京大学学报(医学版), 2001, 33(3): 238-242. |
|
||
