北京大学学报(医学版) ›› 2020, Vol. 52 ›› Issue (3): 521-526. doi: 10.19723/j.issn.1671-167X.2020.03.019
基于15省城镇医疗保险数据测算我国成人进行性肌萎缩患病率
许璐1,陈璐2,樊东升2,冯菁楠1,刘立立1,詹思延1,3,王胜锋1,△( )
)
- 1. 北京大学公共卫生学院流行病与卫生统计学系,北京 100191
2. 北京大学第三医院神经内科,北京 100191
3. 北京大学第三医院临床流行病学中心,北京 100191
Calculation of the prevalence of progressive muscular atrophy among adults in China based on urban medical insurance data from 15 provinces
Lu XU1,Lu CHEN2,Dong-sheng FAN2,Jing-nan FENG1,Li-li LIU1,Si-yan ZHAN1,3,Sheng-feng WANG1,△()
- 1. Department of Epidemiology and Biostatistics, Peking University School of Public Health, Beijing 100191, China
2. Department of Neurology, Peking University Third Hospital, Beijing 100191, China
3. Research Center of Clinical Epidemiology, Peking University Third Hospital, Beijing 100191, China
摘要:
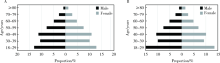
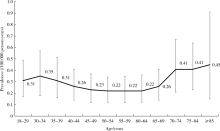
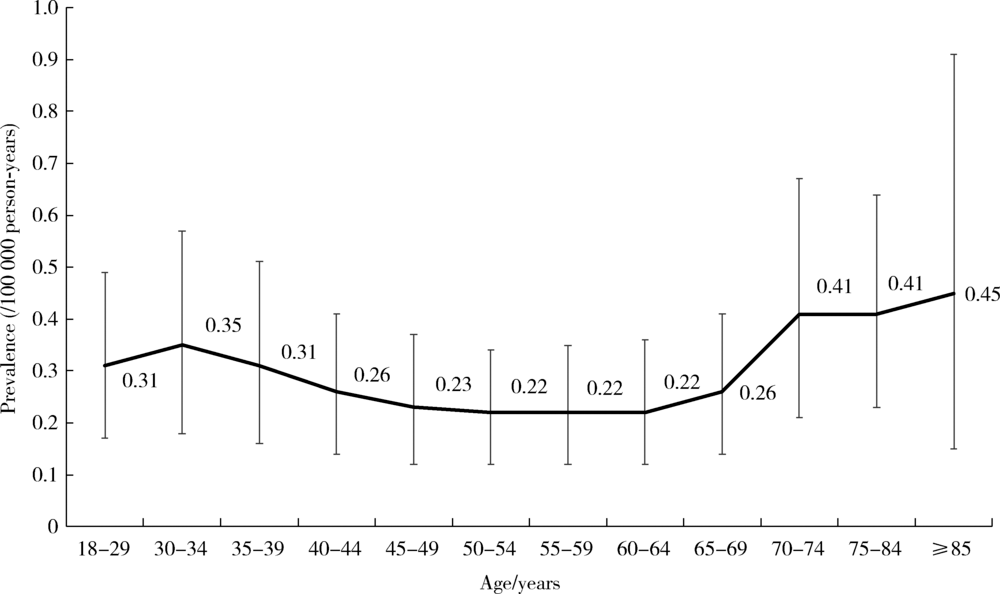
目的 分析进行性肌萎缩(progressive muscular atrophy,PMA)患者的基本人口学特征并测算其患病率。方法 研究基于我国15省2016年1月1日至12月31日的城镇职工和城镇居民医疗保险数据,排除18岁以下儿童。通过疾病诊断名称和疾病诊断编码来识别PMA患者,按照性别、地区和年龄进行亚组分析,并依据我国2010年全国人口普查数据计算PMA按年龄调整后的患病标化率,通过不估算诊断信息缺失的参保人群中潜在的PMA患者数和剔除诊断信息缺失率前10%的省份(湖北、山东)进行敏感性分析。结果 纳入的总参保人年数为99 609万,其中男性为51 841万,女性为47 767万。研究人群与我国2010年人口普查性别年龄结构类似,研究人群具有全国代表性。2016年我国PMA患病率为0.28/10万人年(95%CI:0.24~0.33),其中女性为0.21/10万人年(95%CI:0.16~0.26),男性为0.35/10万人年(95%CI:0.28~0.42)。我国PMA患病率存在地区差异,表现为西南地区患病率最低(0.11/10万人年,95%CI:0.07~0.15),西北地区患病率最高(3.47/10万人年,95%CI:0.80~7.99)。各年龄段患病率差异较小,其中70岁以上人群患病率相对较高。全国患病标化率为0.29/10万人年(95%CI:0.27~0.31)。不估算诊断信息缺失的参保人群中潜在的PMA患者数和剔除诊断信息缺失率前10%的省份后所得的敏感性分析结果分别为0.17/10万人年(95%CI:0.14~0.20)和0.24/10万人年(95%CI:0.20~0.28)。结论 通过测算我国城镇人口中成人PMA的患病率,为PMA相关医疗政策的制定提供基础数据,也为PMA疾病机制的研究提供线索。
中图分类号:
- R195.4

| [1] | Liewluck T, Saperstein DS. Progressive muscular atrophy[J]. Neurol Clin, 2015,33(4):761-773. |
| [2] |
Fowler WS, Miller RD, Mulder DW, et al. Exertional dyspnea: a primary complaint in unusual cases of progressive muscular atrophy and amyotrophic lateral sclerosis[J]. Ann Intern Med, 1957,46(1):119-125.
pmid: 13395221 |
| [3] | Logroscino G, Piccininni M, Marin B, et al. Global, regional, and national burden of motor neuron diseases 1990—2016: a systematic analysis for the Global Burden of Disease Study 2016[J]. Lancet Neurol, 2018,17(12):1083-1097. |
| [4] | Xu L, Liu T, Liu L, et al. Global variation in prevalence and incidence of amyotrophic lateral sclerosis: a systematic review and meta-analysis[J]. J Neurol, 2020,267(4):944-953. |
| [5] |
Pinho AC, Goncalves E. Are amyotrophic lateral sclerosis caregi-vers at higher risk for health problems?[J]. Acta Med Port, 2016,29(1):56-62.
pmid: 26926900 |
| [6] | Tsai CP, Wang KC, Hwang CS, et al. Incidence, prevalence, and medical expenditures of classical amyotrophic lateral sclerosis in Taiwan, 1999—2008[J]. J Formos Med Assoc, 2015,114(7):612-619. |
| [7] | Riku Y, Atsuta N, Yoshida M, et al. Differential motor neuron involvement in progressive muscular atrophy: a comparative study with amyotrophic lateral sclerosis[J]. BMJ Open, 2014,4(5):e005213. |
| [8] |
Kim WK, Liu X, Sandner J, et al. Study of 962 patients indicates progressive muscular atrophy is a form of ALS[J]. Neurology, 2009,73(20):1686-1692.
pmid: 19917992 |
| [9] | 王胜锋, 詹思延, 许璐, 等. 基于医保数据的单病种诊断信息快速结构化方法: 中国, CN109344250A [P]. 2019-02-15. |
| [10] |
Xu L, Chen L, Wang S, et al. Incidence and prevalence of amyotrophic lateral sclerosis in urban China: a national population-based study[J]. J Neurol Neurosurg Psychiatry, 2020,91(5):520-525.
pmid: 32139654 |
| [11] | Noubiap JJ, Nansseu JR, Nyaga UF, et al. Global prevalence of diabetes in active tuberculosis: a systematic review and meta-analysis of data from 2.3 million patients with tuberculosis[J]. Lancet Glob Health, 2019,7(4):e448-e460. |
| [12] |
Leigh PN, Ray-Chaudhuri K. Motor neuron disease[J]. J Neurol Neurosurg Psychiatry, 1994,57(8):886-896.
pmid: 8057109 |
| [13] | Chio A, Brignolio F, Leone M, et al. A survival analysis of 155 cases of progressive muscular atrophy[J]. Acta Neurol Scand, 1985,72(4):407-413. |
| [14] |
Maragakis NJ. Motor neuron disease: progressive muscular atrophy in the ALS spectrum[J]. Nat Rev Neurol, 2010,6(4):187-188.
pmid: 20379201 |
| [15] | Marin B, Boumediene F, Logroscino G, et al. Variation in worldwide incidence of amyotrophic lateral sclerosis: a meta-analysis[J]. Int J Epidemiol, 2017,46(1):57-74. |
| [16] | 邢志宏, 叶植材. 中国统计年鉴 [M]. 北京: 中国统计出版社, 2017: 31. |
| [17] | Cui F, Liu M, Chen Y, et al. Epidemiological characteristics of motor neuron disease in Chinese patients[J]. Acta Neurol Scand, 2014,130(2):111-117. |
| [18] | Wicks P, Abrahams S, Leigh PN, et al. Absence of cognitive, behavioral, or emotional dysfunction in progressive muscular atrophy[J]. Neurology, 2006,67(9):1718-1719. |
| [19] |
Chen L, Zhang B, Chen R, et al. Natural history and clinical features of sporadic amyotrophic lateral sclerosis in China[J]. J Neurol Neurosurg Psychiatry, 2015,86(10):1075-1081.
pmid: 26124198 |
| [20] | Smoyer-Tomic KE, Amato AA, Fernandes AW. Incidence and prevalence of idiopathic inflammatory myopathies among commercially insured, medicare supplemental insured, and medicaid enrolled populations: an administrative claims analysis[J]. BMC Musculoskelet Disord, 2012,13:103. |
| [21] | Ki M, Choi HY, Kim KA, et al. Incidence, prevalence and complications of Budd-Chiari syndrome in South Korea: a nationwide, population-based study[J]. Liver Int, 2016,36(7):1067-1073. |
| [22] |
Rhee C, Dantes R, Epstein L, et al. Incidence and trends of sepsis in US hospitals using clinical vs claims data, 2009—2014[J]. JAMA, 2017,318(13):1241-1249.
doi: 10.1001/jama.2017.13836 pmid: 28903154 |
| [23] |
Donnachie E, Schneider A, Mehring M, et al. Incidence of irritable bowel syndrome and chronic fatigue following GI infection: a population-level study using routinely collected claims data[J]. Gut, 2018,67(6):1078-1086.
pmid: 28601847 |
| [1] | 黄宁, 刘笑晗, 郭静. 医疗保险对流动慢性病患者卫生服务利用的影响以及健康风险感知在其中的调节作用[J]. 北京大学学报(医学版), 2026, 58(1): 160-168. |
| [2] | 章湖洋, 景日泽, 王金喜, 方海. 心力衰竭患者门诊服务利用对住院率的影响及其阈值效应——以浙江省城镇职工患者为例[J]. 北京大学学报(医学版), 2025, 57(4): 753-758. |
| [3] | 陈欣, 杨君婷, 郭金鑫, 李淑雅, 刘志科, 朱颖靓, 李奉娟, 詹思延, 郭娟娟. 2022—2024年青岛市10~59岁女性自身免疫性甲状腺病的患病率特征[J]. 北京大学学报(医学版), 2025, 57(3): 507-513. |
| [4] | 阿娜尔古丽·阿不都肉什提, 宋迎豪, 闫晓晋, 高永康, 刘波, 胡刚. 1990—2021年中国及全球增龄性听力损失的疾病负担与未来趋势预测[J]. 北京大学学报(医学版), 2025, 57(3): 545-553. |
| [5] | 林芳汝, 唐志辉. 种植单冠修复后种植体周健康的相关分析[J]. 北京大学学报(医学版), 2025, 57(2): 347-353. |
| [6] | 曾媛媛,谢云,陈道南,王瑞兰. 脓毒症患者发生正常甲状腺性病态综合征的相关因素[J]. 北京大学学报(医学版), 2024, 56(3): 526-532. |
| [7] | 傅强,高冠英,徐雁,林卓华,孙由静,崔立刚. 无症状髋关节前上盂唇撕裂超声与磁共振检查的对比研究[J]. 北京大学学报(医学版), 2023, 55(4): 665-669. |
| [8] | 林咏惟,周雅琳,赵润茏,许雅君,刘燕萍. 孕早期女性铁营养状况及其影响因素分析[J]. 北京大学学报(医学版), 2023, 55(4): 600-605. |
| [9] | 吴俊慧,陈泓伯,武轶群,吴瑶,王紫荆,吴涛,王梦莹,王斯悦,王小文,王伽婷,于欢,胡永华. 2015—2017年北京市2型糖尿病患者骨关节炎患病的相关因素[J]. 北京大学学报(医学版), 2021, 53(3): 518-522. |
| [10] | 耿研,宋志博,张晓慧,邓雪蓉,王昱,张卓莉. 银屑病关节炎抑郁和焦虑患病情况及相关因素[J]. 北京大学学报(医学版), 2020, 52(6): 1048-1055. |
| [11] | 邓思危,陈则亦,刘志科,王健,卓琳,高双庆,余家阔,詹思延. 基于城镇医保数据库骨关节伤病的流行病学研究[J]. 北京大学学报(医学版), 2020, 52(3): 527-534. |
| [12] | 石慧峰, 张敬旭, 张嵘, 王晓莉. 中国0~6岁儿童孤独症谱系障碍患病率的meta分析[J]. 北京大学学报(医学版), 2017, 49(5): 798-806. |
| [13] | 郁静茹, 金蕾, 肖利华, 靳蕾. 北京通州区神经管缺陷患病率及其与监测时限的关系[J]. 北京大学学报(医学版), 2015, 47(6): 1042-1045. |
| [14] | 李恒, 黄悦勤, 马亚婷, 刘肇瑞. 中国归因于非痴呆器质性精神障碍残疾的描述性流行病学研究[J]. 北京大学学报(医学版), 2014, 46(2): 247-253. |
| [15] | 庞明樊, 冯星淋. 城市中老年慢性病防治就诊倾向分析[J]. 北京大学学报(医学版), 2014, 46(2): 220-225. |
|
||
