北京大学学报(医学版) ›› 2020, Vol. 52 ›› Issue (5): 828-835. doi: 10.19723/j.issn.1671-167X.2020.05.006
食管胃流出道梗阻患者的病因及不同亚组食管动力特点分析
王琨,徐志洁,葛颖,夏志伟,段丽萍( )
)
- 北京大学第三医院消化科,北京 100191
Study of etiology and esophageal motility characteristics of esophagogastric junction outlet obstruction patients
Kun WANG,Zhi-jie XU,Ying GE,Zhi-wei XIA,Li-ping DUAN()
- Department of Gastroenterology, Peking University Third Hospital, Beijing 100191, China
摘要:
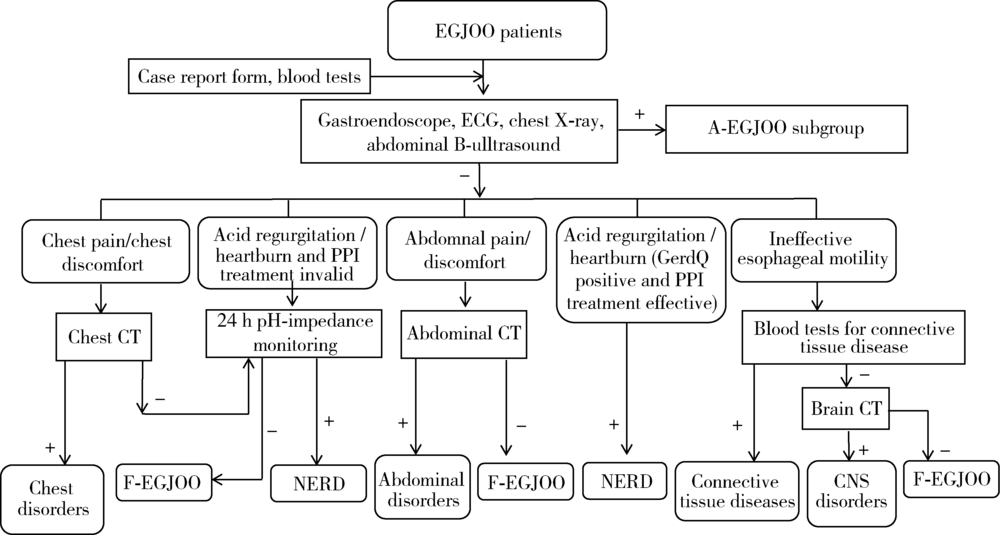
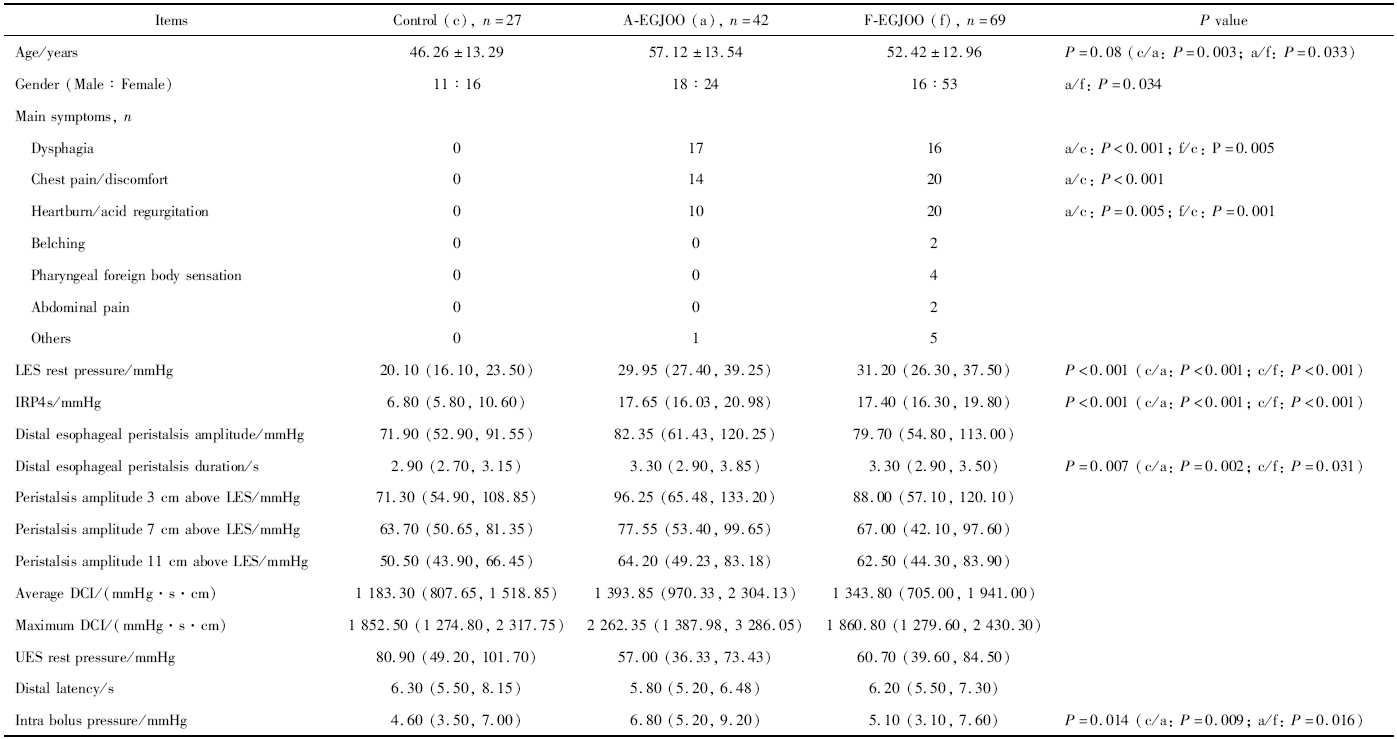
目的:分析食管胃流出道梗阻(esophagogastric junction outlet obstruction,EGJOO)患者的病因,探讨不同亚型EGJOO患者临床及食管动力特点。方法:回顾分析北京大学第三医院消化科因各种症状接受高分辨率食管压力测定的患者,筛选EGJOO患者。分析EGJOO患者的临床特点,探讨病因,依据病因将患者分为解剖异常性EGJOO组(anatomic EGJOO,A-EGJOO)和功能性EGJOO组(functional EGJOO,F-EGJOO)。比较两组患者间症状、食管动力参数的差异,将差异参数绘制受试者工作特征(receiver operating characteristic,ROC)曲线,分析差异参数鉴别两个亚组患者的诊断效力。结果:EGJOO患者最常见的症状为胸痛/胸骨后不适(30.63%),其次为吞咽困难(29.73%)及反酸烧心(27.03%)。原发病因中最常见的为非糜烂性反流病(36.04%),其次为反流性食管炎(17.12%),其他病因包括食管胃交界部良、恶性病变,有部分患者为结缔组织病(6.31%)及中枢神经系统疾病(2.70%), 19例患者(17.12%)经完善研究流程后未发现明确病因。A-EGJOO患者的食团内压明显高于F-EGJOO患者[6.80 (5.20, 9.20) mmHg vs. 5.10 (3.10, 7.60) mmHg, P=0.016],以食团内压为标准,ROC曲线下面积为0.637(P=0.016),当食团内压≥5.15 mmHg时,其从EGJOO中鉴别出A-EGJOO的敏感度为78.60%、特异度为50.70%。结论:EGJOO患者的常见症状为胸痛、吞咽困难,常见的病因除胃食管反流病,食管胃交界部各类良、恶性病变外,还存在食管胃交界部腔外病变及非消化道疾病等原发病因。在食管动力特点上,A-EGJOO患者的食团内压高于F-EGJOO患者,在EGJOO亚型的鉴别诊断中,食团内压具有一定的敏感度和特异度,但由于ROC曲线下面积小于0.7,作为鉴别诊断指标的意义有限。
中图分类号:
- R571


| [1] |
Kahrilas PJ, Bredenoord AJ, Fox M, et al. The Chicago classification of esophageal motility disorder, v3.0[J]. Neurogastroenterol Motil, 2015,27(2):160-174.
doi: 10.1111/nmo.12477 pmid: 25469569 |
| [2] |
Clayton SB, Patel R, Richter JE. Functional and anatomic eso-phagogastic junction outflow obstruction: Manometry, timed barium esophagram findings, and treatment outcomes[J]. Clin Gastroenterol Hepatol, 2016,14(6):907-911.
doi: 10.1016/j.cgh.2015.12.041 pmid: 26792374 |
| [3] | Shin IS, Min YW, Rhee PL. Esophagogastric junction outflow obstruction transformed to type Ⅱ achalasia[J]. J Neurogastorne-terol Motil, 2016,22(2):344-345. |
| [4] |
Ihara E, Muta K, Fukaura K, et al. Diagnosis and treatment strategy of Achalasia subtypes and esophagogastric junction outflow obstruction based on high-resolution manometry[J]. Digestion, 2017,95(1):29-35.
doi: 10.1159/000452354 pmid: 28052278 |
| [5] |
Kim HP, Vance RB, Shaheen NJ, et al. The prevalence and diagnostic utility of endoscopic features of eosinophilic esophagitis: A meta-analysis[J]. Clin Gastroenterol Hepatol, 2012,10(9):988-996.
doi: 10.1016/j.cgh.2012.04.019 pmid: 22610003 |
| [6] |
Armstrong D, Bennett JR, Blum AL, et al. The endoscopic assessment of esophagitis: a progress report on observer agreement[J]. Gastroenterology, 1996,111(1):85-92.
doi: 10.1053/gast.1996.v111.pm8698230 pmid: 8698230 |
| [7] | Zerbib F, Des Varannea SB, Roman S, et al. Normal values and day-to-day variability of 24-h-ambulatory oesophageal impedance pH monitoring in a Belgian-French cohort of healthy subjects[J]. Aliment Pha rmacol Ther, 2005,22(10):1011-1021. |
| [8] |
Samo S, Qayed E. Esophagogastric junction outflow obstruction: Where are we now in diagnosis and management?[J]. World J Gastroenterol, 2019,25(4):411-417.
doi: 10.3748/wjg.v25.i4.411 pmid: 30700938 |
| [9] |
Pérez-Fernández MT, Santander C, Marinero A, et al. Characte-rization and follow-up of esophagogastric junction outflow obstruction detected by high resolution manometry[J]. Neurogastroenterol Motil, 2016,28(1):116-126.
pmid: 26517978 |
| [10] | Schupack D, Katzka DA, Geno DM, et al. The clinical significance of esophagogastric junction outflow obstruction and hypercontractile esophagus in high resolution esophageal manometry[J]. Neruogastroenterol Motil, 2017,29(10):1-9. |
| [11] |
Ong AML, Namasivayam V, Wang YT. Evaluation of symptomatic esophagogastric junction outflow obstruction[J]. J Gastroenterol Hepatol, 2018,33(10):1745-1750.
doi: 10.1111/jgh.14155 pmid: 29660156 |
| [12] |
Gyawali CP, Kushnir VM. High-resolution manometric characte-ristics help differentiate types of distal esophageal obstruction in patients with peristalsis[J]. Neurogastroenterol Motil, 2011,23(6):502-508, e197.
pmid: 21303431 |
| [13] | 王琨, 段丽萍, 夏志伟, 等. 基于高分辨食管压力测定及阻抗-pH监测的难治性烧心患者食管动力特点[J]. 中华医学杂志, 2014,94(34):2650-2655. |
| [1] | 孟伶宇, 黄永辉, 闫秀娥, 王迎春. 兔食管良性环周狭窄模型的建立[J]. 北京大学学报(医学版), 2026, 58(2): 380-387. |
|
||
