北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (3): 473-478. doi: 10.19723/j.issn.1671-167X.2021.03.006
双胎妊娠孕早期甲状腺功能及其与早产的关联性
宋沁峰1,2,李宏田1,2,杨静3,原鹏波3,程志浩1,2,刘建蒙1,2,Δ( ),赵扬玉3,Δ()
),赵扬玉3,Δ()
- 1.北京大学生育健康研究所,国家卫生健康委员会生育健康重点实验室,北京 100191
2.北京大学公共卫生学院流行病与卫生统计学系,北京 100191
3.北京大学第三医院妇产科,北京 100191
Thyroid function of first-trimester twin pregnant women and its association with preterm delivery
SONG Qin-feng1,2,LI Hong-tian1,2,YANG Jing3,YUAN Peng-bo3,CHENG Zhi-hao1,2,LIU Jian-meng1,2,Δ(),ZHAO Yang-yu3,Δ()
- 1. Institute of Reproductive and Child Health, National Health Commission Key Laboratory of Reproductive Health, Peking University, Beijing 100191, China
2. Department of Epidemiology and Biostatistics, Peking University School of Public Health, Beijing 100191, China
3. Department of Obstetrics and Gynecology, Peking University Third Hospital, Beijing 100191, China
摘要:
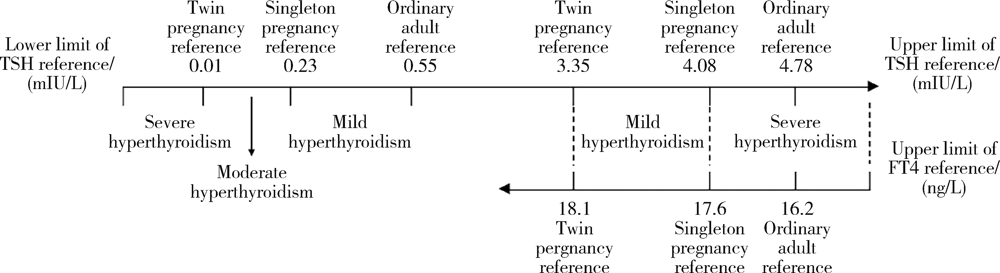
目的: 根据不同参考范围,描述双胎妊娠孕妇孕早期甲状腺功能异常情况,并探究其与早产的关联性。方法: 以2017年3月至2020年2月在北京大学第三医院募集的双胎妊娠孕妇为对象,根据Siemens公司生产的检测试剂盒标识的普通成人甲状腺激素参考范围、既往研究建立的单胎妊娠特异甲状腺激素参考范围和双胎妊娠特异甲状腺激素参考范围,描述孕妇甲状腺功能减退(简称“甲减”)和甲状腺功能亢进(简称“甲亢”)情况;根据Siemens公司生产的甲状腺自身抗体检测试剂盒标识的参考范围,描述孕妇甲状腺自身抗体阳性情况;先后以所有参考范围均判定正常的孕妇、双胎特异参考范围判定正常且甲状腺自身抗体阴性的孕妇为对照,采用多变量对数二项式模型分析甲状腺功能与早产的关联性。结果: 共纳入双胎妊娠孕妇570例,根据普通成人、单胎和双胎参考范围的甲减检出率依次为1.2%、1.6%和3.5%,甲亢检出率依次为32.6%、18.1%和1.1%。调整潜在混杂因素后,与根据三种参考范围判定均正常的孕妇相比,根据双胎特异参考范围判定为甲亢者的早产发生风险显著增加 [调整相对危险度(adjusted relative risk,ARR)为1.41,95%置信区间(confidence interval,CI)为1.14~1.75],根据双胎特异参考范围判定为正常但根据单胎特异参考范围判定为甲亢者(ARR=1.00,95%CI:0.81~1.25)和仅根据普通成人参考范围判定为甲亢者(ARR=1.06,95%CI:0.85~1.32)的早产发生风险均未见显著增加;根据普通成人或单胎特异参考范围判定为甲减者(ARR=1.40,95%CI:0.88~2.22)和仅根据双胎特异参考范围判定为甲减者(ARR=1.53,95%CI:1.03~2.28)的早产发生风险均临界显著或显著增加。综合双胎特异参考范围判定结果与甲状腺自身抗体情况进一步分析发现,与双胎特异参考范围判定为正常且甲状腺自身抗体阴性者相比,单纯甲减者、单纯抗体阳性者以及甲减合并抗体阳性者的早产发生风险均临界显著或显著增加,ARR依次为1.46(95%CI:0.93~2.27)、1.32(95%CI:1.15~1.52)和1.78(95%CI:1.30~2.44)。结论: 根据普通成人或单胎特异参考范围判定双胎妊娠孕妇孕早期甲状腺功能可能会漏诊甲减、误诊甲亢,甲减漏诊孕妇早产发生风险高于甲状腺功能正常孕妇,甲亢误诊孕妇早产发生风险与甲状腺功能正常孕妇相仿,表明亟待建立与推广双胎妊娠特异性甲状腺功能指标参考范围;此外,对双胎妊娠甲减孕妇进行产前诊断和治疗时还应考虑甲状腺自身抗体情况。
中图分类号:
- R173

| [1] | 《妊娠和产后甲状腺疾病诊治指南(第2版) 编撰委员会, 中华医学会内分泌学分会, 中华医学会围产医学分会. 妊娠和产后甲状腺疾病诊治指南(第2版)[J]. 中华内分泌代谢杂志, 2019,35(8):636-665. |
| [2] | 胡静, 郭晓玥, 赵扬玉. 双胎妊娠与母体甲状腺功能的研究进展[J]. 实用妇产科杂志, 2020,36(4):265-267. |
| [3] |
Alexander EK, Pearce EN, Brent GA, et al. 2017 guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and the postpartum[J]. Thyroid, 2017,27(3):315-389.
doi: 10.1089/thy.2016.0457 pmid: 28056690 |
| [4] |
Gaberšček S, Zaletel K. Thyroid physiology and autoimmunity in pregnancy and after delivery[J]. Expert Rev Clin Immunol, 2011,7(5):697-707.
doi: 10.1586/eci.11.42 pmid: 21895480 |
| [5] |
Rosario PW, Carvalho M, Calsolari MR. TSH reference values in the first trimester of gestation and correlation between maternal TSH and obstetric and neonatal outcomes: a prospective Brazilian study[J]. Arch Endocrinol Metab, 2016,60(4):314-318.
doi: 10.1590/2359-3997000000132 |
| [6] |
Lazarus J, Brown RS, Daumerie C, et al. 2014 European Thyroid Association guidelines for the management of subclinical hypothyroidism in pregnancy and in children[J]. Eur Thyroid J, 2014,3(2):76-94.
doi: 10.1159/000362597 pmid: 25114871 |
| [7] | 张杨, 刘芳, 孙伟杰, 等. 妊娠期特异性甲状腺相关指标的参考范围[J]. 中华医学杂志, 2016,96(5):339-343. |
| [8] |
Jiang YX, Sun WJ, Zhang Y, et al. Thyroid function of twin-pregnant women in early pregnancy[J]. Chin Med J, 2019,132(17):2033-2038.
doi: 10.1097/CM9.0000000000000381 |
| [9] |
Chawanpaiboon S, Vogel JP, Moller AB, et al. Global, regional, and national estimates of levels of preterm birth in 2014: a syste-matic review and modelling analysis[J]. Lancet Glob Health, 2019,7(1):e37-e46.
doi: 10.1016/S2214-109X(18)30451-0 |
| [10] |
Männistö T, Mendola P, Grewal J, et al. Thyroid diseases and adverse pregnancy outcomes in a contemporary US cohort[J]. J Clin Endocrinol Metab, 2013,98(7):2725-2733.
doi: 10.1210/jc.2012-4233 |
| [11] |
He X, Wang P, Wang Z, et al. Thyroid antibodies and risk of preterm delivery: a meta-analysis of prospective cohort studies[J]. Eur J Endocrinol, 2012,167(4):455-464.
doi: 10.1530/EJE-12-0379 |
| [12] | Barjaktarovic M, Korevaar TI, Chaker L, et al. The association of maternal thyroid function with placental hemodynamics[J]. Hum Reprod, 2017,32(3):653-661. |
| [13] | 中华医学会妇产科学分会产科学组. 早产的临床诊断与治疗指南(2014)[J]. 中国实用乡村医生杂志, 2015 (12):9-11. |
| [14] | 中华人民共和国国家卫生和计划生育委员会. 中华人民共和国卫生行业标准成人体重判定: WS/T 428—2013[S/OL]. (2013-08-08) [2021-03-03]. http://www.nhc.gov.cn/wjw/yingyang/201308/a233d450fdbc47c5ad4f08b7e394d1e8.shtml. |
| [15] |
Goldenberg RL, Culhane JF, Iams JD, et al. Epidemiology and causes of preterm birth[J]. Lancet, 2008,371(9606):75-84.
doi: 10.1016/S0140-6736(08)60074-4 pmid: 18177778 |
| [16] |
Korevaar TIM, Derakhshan A, Taylor PN, et al. Association of thyroid function test abnormalities and thyroid autoimmunity with preterm birth: a systematic review and meta-analysis[J]. JAMA, 2019,322(7):632-641.
doi: 10.1001/jama.2019.10931 pmid: 31429897 |
| [17] | 胡寒, 岳军. 妊娠期甲状腺疾病对妊娠结局、胎儿及妊娠期代谢性疾病发生发展的影响研究进展[J]. 山东医药, 2018,58(35):97-100. |
| [18] | 马逸杰, 陈大方. 妊娠期高血压对早产、低出生体重的影响[J]. 中国生育健康杂志, 2020,31(6):517-521. |
| [19] |
Sibai BM, Caritis SN, Hauth JC, et al. Preterm delivery in women with pregestational diabetes mellitus or chronic hypertension relative to women with uncomplicated pregnancies[J]. Am J Obstet Gynecol, 2000,183(6):1520-1524.
pmid: 11120521 |
| [20] |
Thilaganathan B, Khalil A. Multiple pregnancy: preface[J]. Best Pract Res Clin Obstet Gynaecol, 2014,28(2):189-190.
doi: 10.1016/j.bpobgyn.2013.12.009 pmid: 24388730 |
| [1] | 白银晓,刘春毅,张杰,孟文颖,金蕾,靳蕾. 妇女围受孕期服用叶酸或含叶酸的多种微量营养素补充剂与早产的关联性研究[J]. 北京大学学报(医学版), 2023, 55(3): 495-501. |
| [2] | 于昊哲,曾唯珍,吴文雨,姚中强,冯云. 原发性干燥综合征合并甲状腺功能减退眼表状态评估[J]. 北京大学学报(医学版), 2022, 54(4): 705-711. |
| [3] | 陈阳阳,周玉博,杨静,花语蒙,原鹏波,刘爱萍,魏瑗. 双胎妊娠孕期体质量对血清高敏C反应蛋白与妊娠期糖尿病关联的影响:一项队列研究[J]. 北京大学学报(医学版), 2022, 54(3): 427-433. |
| [4] | 李秀兰,吴艳,钟晓云,王敏,黄利. 新生儿重症监护室早产儿母乳喂养促进策略研究[J]. 北京大学学报(医学版), 2019, 51(4): 711-715. |
| [5] | 王立芳,周虹,张妍,王燕. 孕前体质指数与早产的关系[J]. 北京大学学报(医学版), 2016, 48(3): 414-417. |
| [6] | 吴艳, 钟晓云, 蒋静, 龚华. 住院早产超低和极低出生体重儿强化母乳喂养的前瞻性对照研究[J]. 北京大学学报(医学版), 2016, 48(1): 143-148. |
| [7] | 蔡佳,张曼. 孕期不同甲状腺功能状态血清高密度脂蛋白胆固醇和载脂蛋白A-Ⅰ的变化趋势[J]. 北京大学学报(医学版), 2015, 47(6): 910-913. |
| [8] | 冯琪. 早产儿院内营养策略进展及其意义[J]. 北京大学学报(医学版), 2013, 45(2): 333-. |
| [9] | 徐佳露, 杨茹莱, 毛华庆, 赵正言. 浙江省不同地域新生儿先天性甲状腺功能低下症筛查分析[J]. 北京大学学报(医学版), 2012, 44(5): 816-818. |
| [10] | 姚海红, 李玉慧, 张学武, 栗占国. 皮肌炎合并甲状腺功能异常的临床及免疫学特征分析[J]. 北京大学学报(医学版), 2011, 43(2): 209-212. |
| [11] | 沙月琴, 黄振, 陈智滨, 康军, 和璐, 于晓潜. 孕妇牙周炎与新生儿早产低体重的关联[J]. 北京大学学报(医学版), 2009, 41(1): 117-120. |
| [12] | 伍细言, 王华, 黄定梅, 雷花香, 胡蓉, 马力, 邹珊静, 禹虹. 湖南省106 224例新生儿先天性甲状腺功能减低症筛查[J]. 北京大学学报(医学版), 2005, 37(1): 42-44. |
| [13] | 金莹, 陈大方, 杨帆, 李志平, 方治安, 李凌松, 王黎华. 细胞色素P450氧化酶基因MSP1位点多态性与早产的关联性研究[J]. 北京大学学报(医学版), 2004, 36(6): 595-599. |
| [14] | 陈大方, 胡永华, 杨帆, 吴白燕, 陈枥, 方治安, 王黎华. 母亲与婴儿亚甲基四氢叶酸还原酶C677T多态性与早产和低出生体重的相关性研究[J]. 北京大学学报(医学版), 2004, 36(3): 248-253. |
| [15] | 陈大方, 胡永华, 吴白燕, 陈枥, 方治安, 杨帆, 王黎华. 肿瘤坏死因子α/G308A多态性与早产的关联性研究[J]. 北京大学学报(医学版), 2003, 35(4): 377-381. |
|
||
