北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (3): 491-497. doi: 10.19723/j.issn.1671-167X.2021.03.009
2016—2019年宁波市5岁及以下儿童手足口病流行病学特征
刘立立1,刘志科1,张良2,Δ( ),李宁2,方挺2,张栋梁2,许国章2,詹思延1,Δ()
),李宁2,方挺2,张栋梁2,许国章2,詹思延1,Δ()
- 1.北京大学公共卫生学院流行病与卫生统计学系, 北京 100191
2.宁波市疾病控制与预防中心, 浙江宁波 315010
Epidemiological and etiological characteristics of hand, foot and mouth disease among children aged 5 years and younger in Ningbo (2016 to 2019)
LIU Li-li1,LIU Zhi-ke1,ZHANG Liang2,Δ(),LI Ning2,FANG Ting2,Dong-ZHANG Liang2,XU Guo-zhang2,ZHAN Si-yan1,Δ()
- 1. Department of Epidemiology and Biostatistics, Peking University School of Public Health, Beijing 100191, China
2. Ningbo Municipal Center for Disease Control and Prevention, Ningbo 315010, Zhejiang, China
摘要:
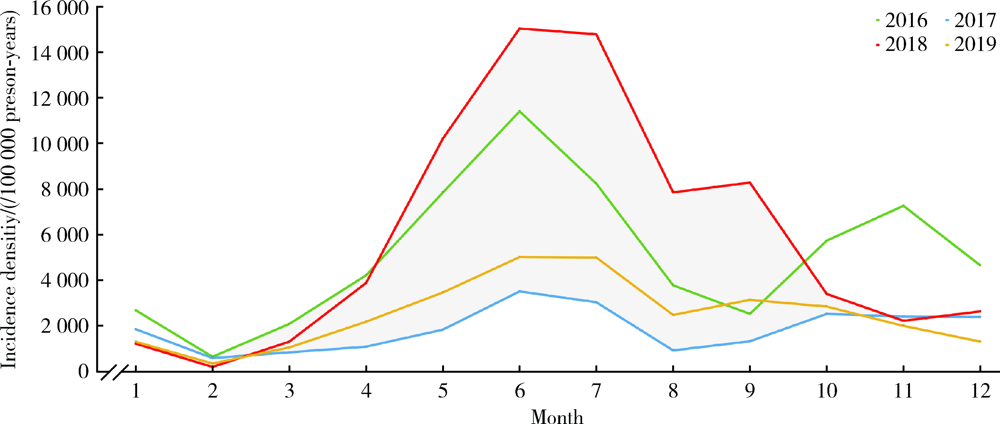
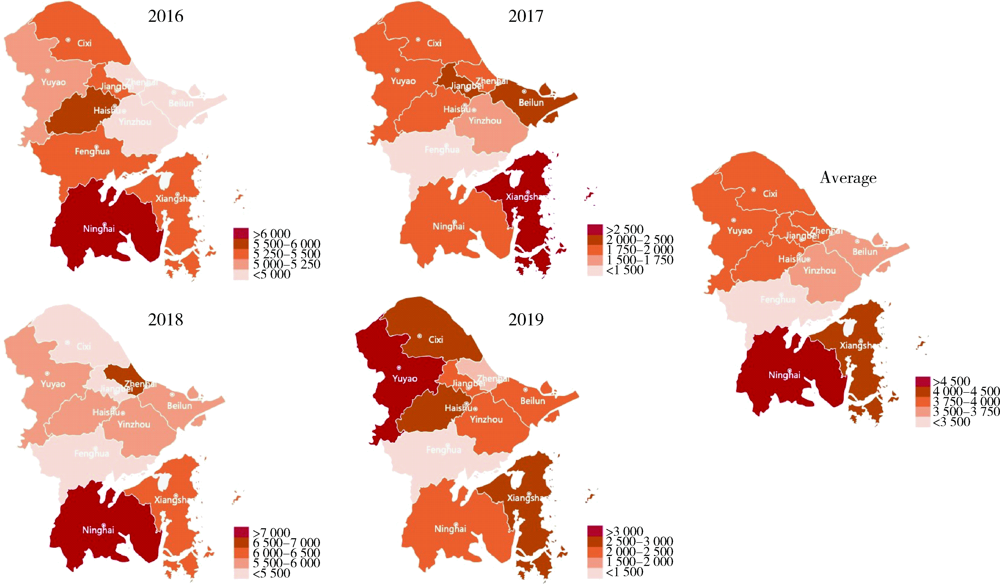
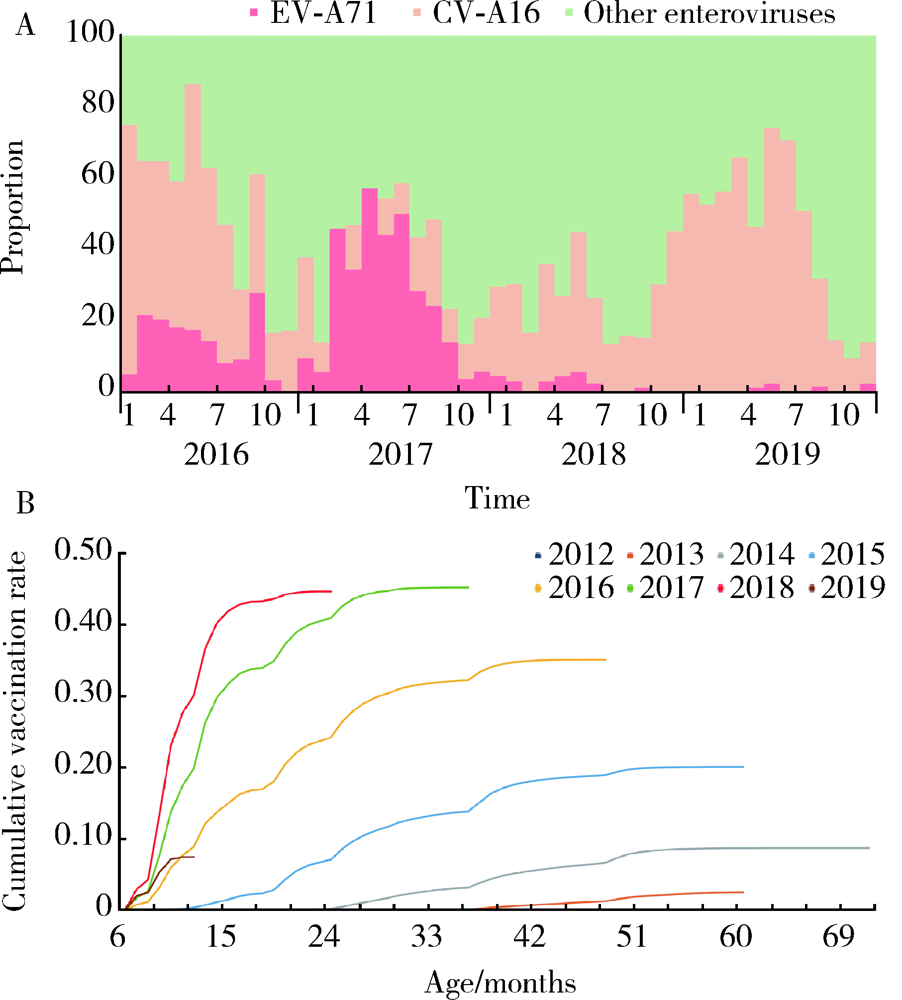
目的: 描述肠道病毒71型(EV-A71)疫苗可及后的2016—2019年宁波市5岁及以下儿童手足口病流行特征及病原学情况。方法: 采用队列设计,回顾性收集2016—2019年宁波全民健康信息平台中传染病报卡和电子病历内手足口病发病资料,人口学统计信息来源于预防接种信息系统,通过实时荧光定量PCR方法进行病毒分型。采用Wilson法估算发病密度及95%置信区间。结果: 2016—2019年,队列累计观察5岁及以下常住儿童1 044 800人,总观察人时为2 651 081人年,期间新发手足口病102 471例,年均发病密度为3 865.25/10万人年。4年间手足口病发病人数为93 421人,其中单人单次发病为84 875人(90.85%), 单人发病2次及以上为8 946人(9.15%);单次发病只需就诊一次者为69 771人(66.06%),有19.92%的患者需就诊2次,而有14.02%(14 801人)的患者需就诊3次及以上。发病具有明显的季节性和周期性,主要集中在每年4至7月,流行周期为2年;绝大部分病例为1~3岁儿童,男性多于女性。各地区发病密度不同,以宁海县最高(4 524.76/10万人年),象山县次之(3 984.22/10万人年)。病毒分型3 748例,实验室确诊2 834例,检出阳性率75.61%,其中肠道病毒71型、柯萨奇病毒A16和其他肠道病毒分别占9.03%、31.55%和59.42%。研究期间,EV-A71疫苗累计接种率逐年升高,EV-A71型病毒占比从2016年的13.34%降低至2019年的0.71%,同期重症病例占比也从1.26%降低至0.54%。结论: 宁波市手足口病疫情依然严峻,1~3岁以下儿童(特别是1岁男性儿童)是重点防控人群,随着疫苗接种率升高,EV-A71感染比例和重症占比均逐渐降低,应及时关注手足口病流行毒株的变化对疾病监测与防控的潜在影响。
中图分类号:
- R572.5

| [1] |
Xie C, Wen H, Yang W, et al. Trend analysis and forecast of daily reported incidence of hand, foot and mouth disease in Hubei, China by prophet model[J]. Sci Rep, 2021,11(1):1445.
doi: 10.1038/s41598-021-81100-2 |
| [2] |
Tyring S. Hand foot and mouth disease: enteroviral load and disease severity[J]. EBioMedicine, 2020,62(12):103115.
doi: 10.1016/j.ebiom.2020.103115 |
| [3] |
Schmidt C. More cases of hand, foot, and mouth disease in China: a consequence of climate change[J]. Environ Health Perspect, 2018,126(9):94002.
doi: 10.1289/EHP3778 |
| [4] |
Li Y, Zhou Y, Cheng Y, et al. Effectiveness of EV-A71 vaccination in prevention of paediatric hand, foot, and mouth disease associated with EV-A71 virus infection requiring hospitalisation in Henan, China, 2017-18: a test-negative case-control study[J]. Lancet Child Adolesc Health, 2019,3(10):697-704.
doi: 10.1016/S2352-4642(19)30185-3 |
| [5] |
Li Y, Chang Z, Wu P, et al. Emerging enteroviruses causing hand, foot and mouth disease, China, 2010—2016[J]. Emerg Infect Dis, 2018,24(10):1902-1906.
doi: 10.3201/eid2410.171953 |
| [6] | 许国章, 倪红霞, 易波, 等. 浙江省宁波市2008—2011年手足口病流行病学及病原学特征分析[J]. 中华流行病学杂志, 2013,34(4):361-365. |
| [7] | 丁克琴, 陈奕, 谢蕾, 等. 2011—2015年宁波市手足口病流行病学与病原学特征分析[J]. 现代预防医学, 2016,43(23):4251-4254, 4263. |
| [8] |
Zhu F, Xu W, Xia J, et al. Efficacy, safety, and immunogenicity of an enterovirus 71 vaccine in China[J]. N Engl J Med, 2014,370(9):818-828.
doi: 10.1056/NEJMoa1304923 |
| [9] |
Liu Z, Zhang L, Yang Y, et al. Active surveillance of adverse events following human papillomavirus vaccination: feasibility pilot study based on the regional health care information platform in the city of Ningbo, China[J]. J Med Internet Res, 2020,22(6):e17446.
doi: 10.2196/17446 |
| [10] | Huang J, Liao Q, Ooi M, et al. Epidemiology of recurrent hand, foot and mouth disease, China, 2008—2015[J]. Emerg Infect Dis, 2018,24(3):432-442. |
| [11] | 国家统计局. 人口和就业[EB/OL]. (2020-06-19)[2021-01-20]. http://www.stats.gov.cn/tjzs/cjwtjd/201308/t20130829_74322.html. |
| [12] | 叶科军. 丙种球蛋白治疗小儿重症手足口病疗效观察[J]. 吉林医学, 2013,34(32):6733-6734. |
| [13] | 张静, 靳妍, 孙军玲, 等手足口病重症病例临床分期与结局分析[J]. 中华流行病学杂志, 2017,38(5):651-655. |
| [14] | 任敏睿, 崔金朝, 聂陶然, 等. 2008—2018年中国手足口病重症病例流行病学特征分析[J]. 中华流行病学杂志, 2020,41(11):1802-1807. |
| [15] | 王笑笑, 蔡剑, 韩桃利, 等. 2009—2017年浙江省手足口病流行病学特征及病原学监测分析[J]. 中华实验和临床病毒学杂志, 2019,33(1):1-5. |
| [16] | 陈琦, 邢学森, 吴杨, 等. 湖北省2009—2015年手足口病流行病学和病原学分析[J]. 中华流行病学杂志, 2017,38(4):441-445. |
| [17] | 金丽珠, 葛辉, 杜雪杰, 等. 2015年全国医疗机构法定传染病报告质量调查分析[J]. 疾病监测, 2016,31(10):883-886. |
| [18] | 陈飒, 赵斌, 刘艳, 等. 陕西省2009—2018年手足口病流行特征及动态变化分析[J]. 中华流行病学杂志, 2019,40(9):1120-1124. |
| [19] |
Guan X, Che Y, Wei S, et al. Effectiveness and safety of an inactivated enterovirus 71 vaccine in children aged 6-71 months in a phase Ⅳ study[J]. Clin Infect Dis, 2020,71(9):2421-2427.
doi: 10.1093/cid/ciz1114 |
| [20] |
Jiang L, Wang J, Zhang C, et al. Effectiveness of enterovirus A71 vaccine in severe hand, foot, and mouth disease cases in Guangxi, China[J]. Vaccine, 2020,38(7):1804-1809.
doi: S0264-410X(19)31667-6 pmid: 31892446 |
| [21] | 黄威, 陈雨, 罗恺炜 等. 湖南省2008—2017年手足口病病原学与流行特征分析[J]. 中华实验和临床病毒学杂志, 2019,33(1):16-20. |
| [22] |
Fan S, Liao Y, Jiang G, et al. Efficacy of an inactivated bivalent vaccine for enterovirus 71 and coxsackievirus A16 in mice immunized intradermally[J]. Vaccine, 2021,39(3):596-604.
doi: 10.1016/j.vaccine.2020.11.070 |
| [23] |
Liu D, Leung K, Jit M, et al. Cost-effectiveness of bivalent versus monovalent vaccines against hand, foot and mouth disease[J]. Clin Microbiol Infect, 2020,26(3):373-380.
doi: 10.1016/j.cmi.2019.06.029 |
| [24] | Wang J, Teng Z, Cui X, et al. Epidemiological and serological surveillance of hand-foot-and-mouth disease in Shanghai, China, 2012—2016[J]. Emerg Microbes Infect, 2018,7(1):8. |
| [25] | Yang B, Liu F, Liao Q, et al. Epidemiology of hand, foot and mouth disease in China, 2008 to 2015 prior to the introduction of EV-A71 vaccine[J]. Euro Surveill. 2017,22(50):824. |
| [26] | 邢志红, 叶植材. 中国统计年鉴[M]. 北京: 中国统计出版社, 2017: 1. |
| [27] | 孟兆敏, 吴瑞君. 流动人口与户籍人口的收入差异及其影响因素: 以上海市为例[J]. 城市问题, 2016,6(1):82-91. |
| [1] | 刘光旭, 张良, 赵厚宇, 邓思危, 杨君婷, 李宁, 马瑞, 何艳, 许国章, 刘志科, 詹思延. 2015—2021年宁波市6岁以下儿童热性惊厥的流行病学特征[J]. 北京大学学报(医学版), 2025, 57(3): 584-591. |
| [2] | 刘光奇,庞元捷,吴疆,吕敏,于孟轲,李雨橦,黄旸木. 2013—2019年流感季北京市住院老年人流感疫苗接种趋势分析[J]. 北京大学学报(医学版), 2022, 54(3): 505-510. |
|
||
