北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (6): 1128-1132. doi: 10.19723/j.issn.1671-167X.2021.06.020
卡托普利试验在醛固酮腺瘤无创诊断中的临床价值
董博*,马晓伟( ),郭晓蕙,高莹,张俊清
),郭晓蕙,高莹,张俊清
- 北京大学第一医院内分泌科,北京 100034
Clinical value of captopril test in noninvasive diagnosis of aldosterone-producing adenoma
DONG Bo*,MA Xiao-wei(),GUO Xiao-hui,GAO Ying,ZHANG Jun-qing
- Department of Endocrinology, Peking University First Hospital, Beijing 100034, China
摘要:
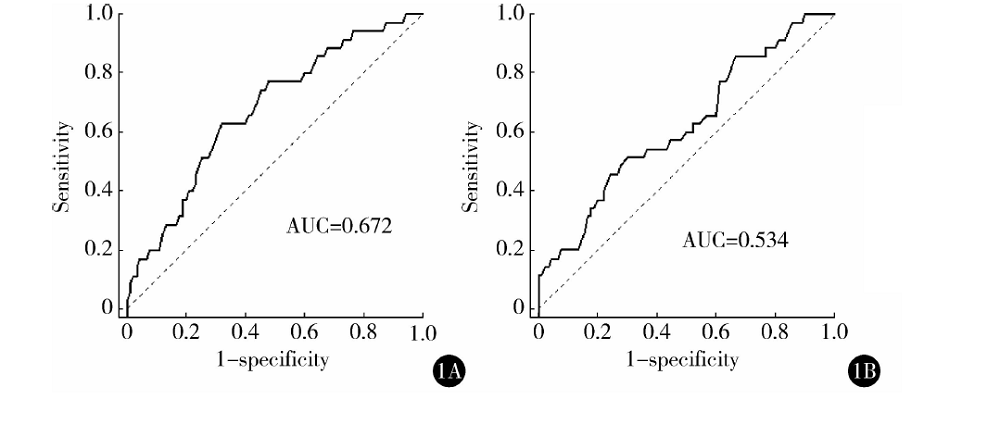
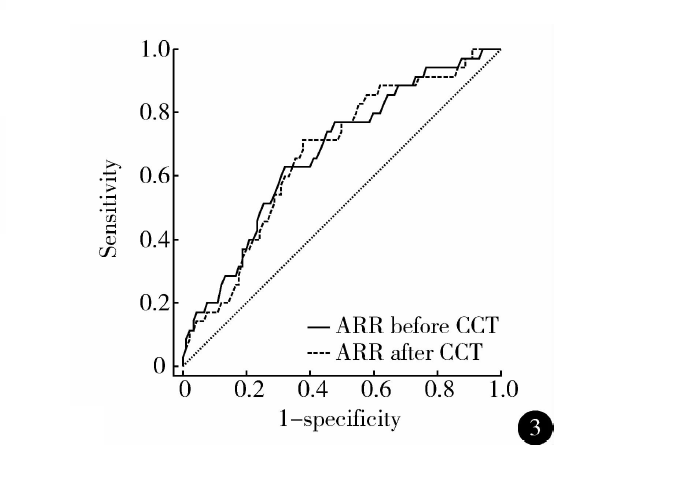
目的:分析原发性醛固酮增多症(primary aldosteronism,PA)中醛固酮腺瘤(aldosterone-producing adenoma,APA)亚型的临床特点及卡托普利试验(captopril challenge test,CCT)在APA诊断中的应用价值,尝试寻找从PA中识别APA的临床特异性无创指标。方法:回顾性收集因高血压住院患者的临床资料,确诊PA者90例,其中手术证实为APA者34例。对两组患者临床指标,包括CCT前后的血浆醛固酮浓度(plasma aldosterone concentration,PAC)、醛固酮/肾素比值(aldosterone to renin ratio,ARR)以及CCT后的醛固酮抑制率(%)进行比较,并绘制CCT前后相关指标的受试者工作特征曲线,比较曲线下面积(area under the curve,AUC)。结果:与PA组相比,APA患者确诊时高血压病程较短,低血钾发生率更高,血钾平均水平更低,两者的血压水平、性别分布、血钠水平、体重指数差异无统计学意义。APA组CCT前ARR及CCT后PAC、ARR、醛固酮抑制率均较PA组高,其中CCT前后ARR均对APA有诊断价值:CCT前ARR临界点为7.12时,灵敏度为35.85%,特异度为77.78%;CCT后ARR临界点为4.23时,灵敏度为71.43%,特异度为62.22%;两者对PA分型的诊断价值相当。CCT前ARR>7.12联合低血钾的诊断特异度高达80%。结论:CCT前后ARR对APA的诊断均具有临床价值,当联合低血钾时诊断特异度增高。
中图分类号:
- R586


| [1] |
Funder JW, Carey RM, Mantero F, et al. The management of primary aldosteronism: Case detection, diagnosis, and treatment. An endocrine society clinical practice guideline[J]. J Clin Endocrinol Metab, 2016, 101(5):1889-1916.
doi: 10.1210/jc.2015-4061 pmid: 26934393 |
| [2] |
Williams TA, Lenders J, Mulatero P, et al. Outcomes after adrenalectomy for unilateral primary aldosteronism: An international consensus on outcome measures and analysis of remission rates in an international cohort[J]. Lancet Diabetes Endocrinol, 2017, 5(9):689-699.
doi: 10.1016/S2213-8587(17)30135-3 |
| [3] | Williams TA, Reincke M. Management of endocrine disease: Diagnosis and management of primary aldosteronism: the Endocrine Society guideline 2016 revisited[J]. 2018, 179(1):R19-R29. |
| [4] | 中华医学会内分泌学分会肾上腺学组. 原发性醛固酮增多症诊断治疗的专家共识[J]. 中华内分泌代谢杂志, 2016, 32(3):188-195. |
| [5] | 吴昱. 醛固酮与肾素活性的比值在原发性醛固酮增多症的诊断价值研究[D]. 南宁: 广西医科大学, 2017. |
| [6] |
Kline GA, Prebtani A, Leung AA, et al. Primary aldosteronism: A common cause of resistant hypertension[J]. CMAJ, 2017, 189(22):E773-E778.
doi: 10.1503/cmaj.161486 |
| [7] |
Nishikawa T, Omura M, Satoh F, et al. Guidelines for the diagnosis and treatment of primary aldosteronism: the Japan Endocrine Society 2009[J]. Endocr J, 2011, 58(9):711-721.
pmid: 21828936 |
| [8] |
Young WF, Stanson AW, Thompson GB, et al. Role for adrenal venous sampling in primary aldosteronism[J]. Surgery, 2004, 136(6):1227-1235.
doi: 10.1016/j.surg.2004.06.051 |
| [9] |
Kerstens MN, Kobold AC, Volmer M, et al. Reference values for aldosterone-renin ratios in normotensive individuals and effect of changes in dietary sodium consumption[J]. Clin Chem, 2011, 57(11):1607-1611.
doi: 10.1373/clinchem.2011.165662 pmid: 21865483 |
| [10] |
Burton TJ, Mackenzie IS, Balan K, et al. Evaluation of the sensitivity and specificity of (11) C-metomidate positron emission tomography (PET)-CT for lateralizing aldosterone secretion by Conn’s adenomas[J]. J Clin Endocrinol Metab, 2012, 97(1):100-109.
doi: 10.1210/jc.2011-1537 |
| [11] |
Lenders J, Eisenhofer G, Reincke M. Subtyping of patients with primary aldosteronism: An update[J]. Horm Metab Res, 2017, 49(12):922-928.
doi: 10.1055/s-0043-122602 |
| [12] |
Shackleton C. Clinical steroid mass spectrometry: A 45-year history culminating in HPLC-MS/MS becoming an essential tool for patient diagnosis[J]. J Steroid Biochem Mol Biol, 2010, 121(3-5):481-490.
doi: 10.1016/j.jsbmb.2010.02.017 |
| [13] |
Biglieri EG, Schambelan M. The significance of elevated levels of plasma 18-hydroxycorticosterone in patients with primary aldosteronism[J]. J Clin Endocrinol Metab, 1979, 49(1):87-91.
doi: 10.1210/jcem-49-1-87 |
| [14] |
Auchus RJ, Chandler DW, Singeetham S, et al. Measurement of 18-hydroxycorticosterone during adrenal vein sampling for primary aldosteronism[J]. J Clin Endocrinol Metab, 2007, 92(7):2648-2651.
doi: 10.1210/jc.2006-2631 |
| [15] | 胡枫湫, 黄娟, 黄慧. 原发性醛固酮增多症诊断性试验在醛固酮瘤诊断中的临床应用与评价[J]. 四川大学学报(医学版), 2018, 49(3):469-473. |
| [1] | 皇甫宇超,杜依青,于路平,徐涛. 原发性醛固酮增多症术后高血压未治愈的危险因素[J]. 北京大学学报(医学版), 2022, 54(4): 686-691. |
| [2] | 王薇,蔡林,高莹,郭晓蕙,张俊清. 原发性醛固酮增多症术后持续性重度高钾血症1例[J]. 北京大学学报(医学版), 2022, 54(2): 376-380. |
| [3] | 安文成,闫慧娴,邓正照,陈芳,欧小虹,金红心,黄薇. 原发性醛固酮增多症肾上腺切除术后慢性肾功能不全1例[J]. 北京大学学报(医学版), 2021, 53(6): 1201-1204. |
|
||
