北京大学学报(医学版) ›› 2024, Vol. 56 ›› Issue (4): 667-672. doi: 10.19723/j.issn.1671-167X.2024.04.020
肾部分切除术治疗囊性肾癌的功能学和肿瘤学结果:单中心回顾性研究
舒帆,郝一昌,张展奕,邓绍晖,张洪宪,刘磊,王国良,田晓军,赵磊,马潞林,张树栋*( )
)
- 北京大学第三医院泌尿外科,北京 100191
Functional and oncologic outcomes of partial nephrectomy for cystic renal cell carcinoma: A single-center retrospective study
Fan SHU,Yichang HAO,Zhanyi ZHANG,Shaohui DENG,Hongxian ZHANG,Lei LIU,Guoliang WANG,Xiaojun TIAN,Lei ZHAO,Lulin MA,Shudong ZHANG*()
- Department of Urology, Peking University Third Hospital, Beijing 100191, China
摘要:
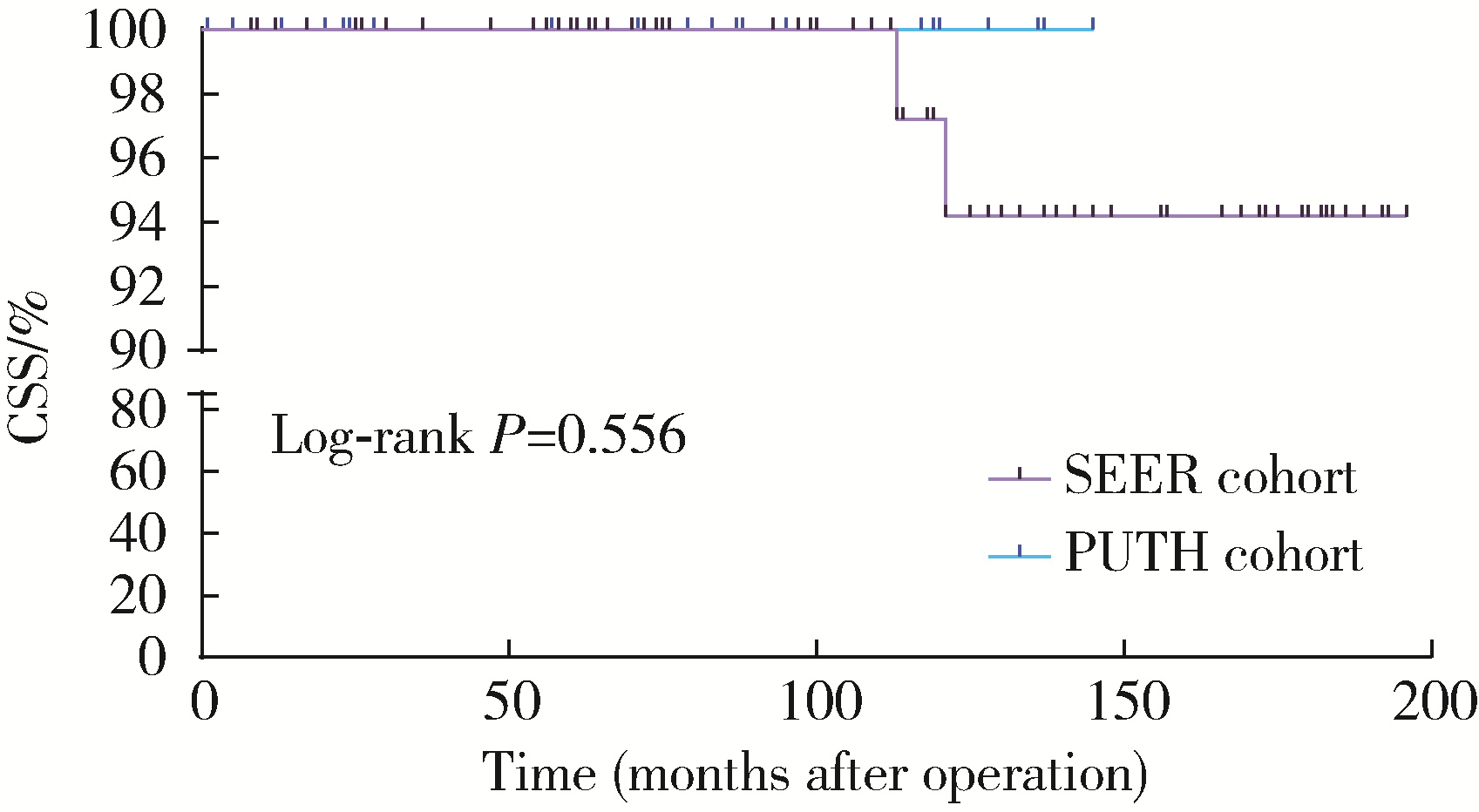
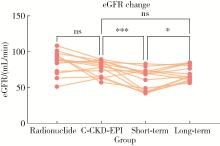
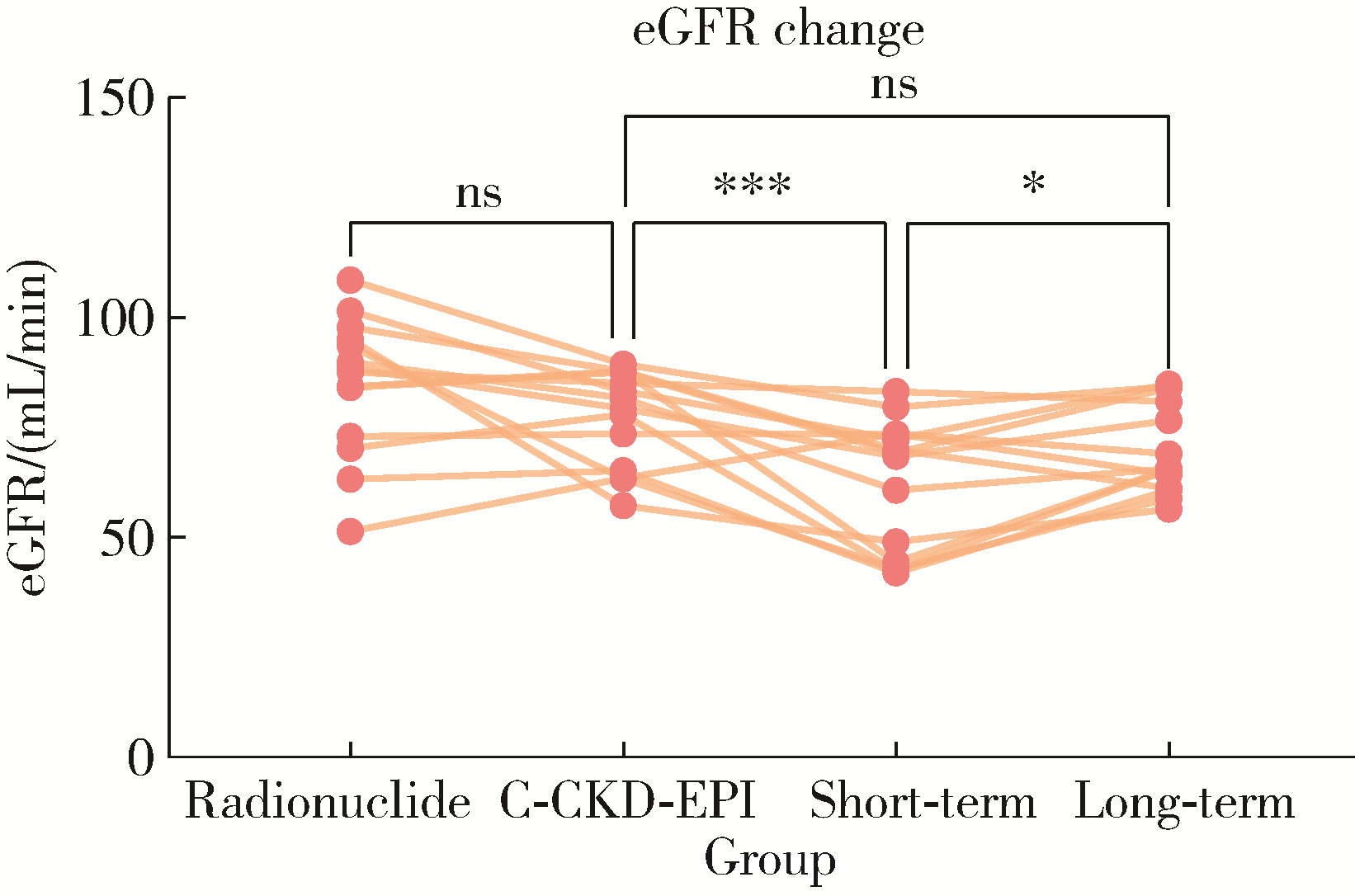
目的: 分析单中心肾部分切除术治疗囊性肾癌的结果,并将其与监测、流行病学和最终结果(Surveillance, Epidemiology, and End Results, SEER)数据库进行对比,探究术后肾功能和肿瘤学结局。方法: 纳入2010—2023年就诊于北京大学第三医院(Peking University Third Hospital, PUTH)泌尿外科行肾部分切除术的囊性肾癌患者,收集临床资料并统计基线特征。分别采用肾动态显像和加入了中国种族系数的慢性肾脏病流行病学协作组(Chinese Coefficients for Chronic Kidney Disease Epidemiology Collaboration,C-CKD-EPI)公式测定估算肾小球滤过率(estimated glomerular filtration rate, eGFR), 并绘制肾功能的变化曲线,对患者进行随访,记录生存状态。纳入SEER数据库中2000—2020年的囊性肾癌病例,进行倾向性评分匹配(propensity score matching, PSM)以平衡与PUTH患者数据的差异,采用Kaplan-Meier方法描绘PUTH队列和SEER队列的肿瘤特异性生存率(cancer-specific survival, CSS)曲线。结果: PUTH患者队列和SEER数据库中的患者队列分别纳入了38例和385例患者,PSM后各筛选出31例和72例,患者的基线特征仅在肿瘤直径上差异有统计学意义(P=0.042)。PSM后在CSS上差异无统计学意义(P=0.556),SEER队列的中位随访时间为112.5个月,10年生存率为97.2%,PUTH队列的中位随访时间为57.0个月、10年生存率为100.0%。肾动态显像测定的eGFR与基于肌酐估算的结果差异无统计学意义(P=0.073);术前、术后短期、术后长期之间的eGFR差异有统计学意义(P<0.001),具体为术后短期肾功能下降,术后长期肾功能恢复。结论: 肾部分切除术治疗囊性肾癌是安全可行的,具有较好的肾功能和肿瘤学结局。
中图分类号:
- R737.11

| 1 |
Bray F , Ferlay J , Soerjomataram I , et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2018, 68 (6): 394- 424.
doi: 10.3322/caac.21492 |
| 2 | Kuroda N , Ohe C , Mikami S , et al. Multilocular cystic renal cell carcinoma with focus on clinical and pathobiological aspects[J]. Histol Histopathol, 2012, 27 (8): 969- 974. |
| 3 |
Wahal SP , Mardi K . Multilocular cystic renal cell carcinoma: A rare entity with review of literature[J]. J Lab Physicians, 2014, 6 (1): 50- 52.
doi: 10.4103/0974-2727.129093 |
| 4 |
Upfill-Brown A , Lenis AT , Faiena I , et al. Treatment utilization and overall survival in patients receiving radical nephroureterectomy versus endoscopic management for upper tract urothelial carcinoma: Evaluation of updated treatment guidelines[J]. World J Urol, 2019, 37 (6): 1157- 1164.
doi: 10.1007/s00345-018-2506-1 |
| 5 |
Yagisawa T , Takagi T , Yoshida K , et al. Surgical outcomes of robot-assisted laparoscopic partial nephrectomy for cystic renal cell carcinoma[J]. J Robot Surg, 2022, 16 (3): 649- 654.
doi: 10.1007/s11701-021-01292-7 |
| 6 |
Lin W , Yang Z , Yan L , et al. Comparison of partial nephrectomy and radical nephrectomy for cystic renal cell carcinoma: A SEER-based and retrospective study[J]. Sci Rep, 2023, 13 (1): 8052.
doi: 10.1038/s41598-023-34950-x |
| 7 |
Wang L , Deng JY , Li KP , et al. Perioperative and oncological outcomes of robot-assisted laparoscopic partial nephrectomy for cystic and solid renal masses: Evidence from controlled trials[J]. Asian J Surg, 2024, 47 (1): 16- 24.
doi: 10.1016/j.asjsur.2023.08.048 |
| 8 |
Yang M , Zou Y , Lu T , et al. Revised Equations to estimate glomerular filtration rate from serum creatinine and cystatin C in China[J]. Kidney Blood Press Res, 2019, 44 (4): 553- 564.
doi: 10.1159/000500460 |
| 9 |
Hartman DS , Davis CJ, Jr , Johns T , et al. Cystic renal cell carcinoma[J]. Urology, 1986, 28 (2): 145- 153.
doi: 10.1016/0090-4295(86)90109-3 |
| 10 |
Bielsa O , Lloreta J , Gelabert-Mas A . Cystic renal cell carcinoma: pathological features, survival and implications for treatment[J]. Br J Urol, 1998, 82 (1): 16- 20.
doi: 10.1046/j.1464-410x.1998.00689.x |
| 11 |
Corica FA , Iczkowski KA , Cheng L , et al. Cystic renal cell carcinoma is cured by resection: A study of 24 cases with long-term followup[J]. J Urol, 1999, 161 (2): 408- 411.
doi: 10.1016/S0022-5347(01)61903-7 |
| 12 |
Koga S , Nishikido M , Hayashi T , et al. Outcome of surgery in cystic renal cell carcinoma[J]. Urology, 2000, 56 (1): 67- 70.
doi: 10.1016/S0090-4295(00)00540-9 |
| 13 | Winters BR , Gore JL , Holt SK , et al. Cystic renal cell carcinoma carries an excellent prognosis regardless of tumor size[J]. Urol Oncol, 2015, 33 (12): 505. e509- 505. e513. |
| 14 | Tretiakova M , Mehta V , Kocherginsky M , et al. Predominantly cystic clear cell renal cell carcinoma and multilocular cystic renal neoplasm of low malignant potential form a low-grade spectrum[J]. Virchows Arch, 2018, 473 (1): 85- 93. |
| 15 | Lee J , Song C , Lee D , et al. Differential contribution of the factors determining long-term renal function after partial nephrectomy over time[J]. Urol Oncol, 2021, 39 (3): 196. e115- 196. e120. |
| 16 |
Park JJ , Jeong BC , Kim CK , et al. Postoperative outcome of cystic renal cell carcinoma defined on preoperative imaging: A retrospective study[J]. J Urol, 2017, 197 (4): 991- 997.
doi: 10.1016/j.juro.2016.10.055 |
| 17 |
Zhang S , Qin Z , Bi H , et al. A "3S+f" nephrometry score system to predict the clinical outcomes of laparoscopic nephron-sparing surgery[J]. Front Oncol, 2022, 12, 922082.
doi: 10.3389/fonc.2022.922082 |
| [1] | 周泽臻, 葛力源, 张帆, 邓绍晖, 颜野, 张洪宪, 王国良, 刘磊, 黄毅, 张树栋. 病理T3a期肾细胞癌肾部分切除与根治性肾切除的回顾性匹配研究[J]. 北京大学学报(医学版), 2025, 57(4): 704-710. |
| [2] | 陈克伟,刘茁,邓绍晖,张帆,叶剑飞,王国良,张树栋. 肾血管平滑肌脂肪瘤伴下腔静脉瘤栓的临床诊治[J]. 北京大学学报(医学版), 2024, 56(4): 617-623. |
| [3] | 邱敏,宗有龙,王滨帅,杨斌,徐楚潇,孙争辉,陆敏,赵磊,卢剑,刘承,田晓军,马潞林. 腹腔镜肾部分切除术治疗中高复杂程度肾肿瘤的效果[J]. 北京大学学报(医学版), 2023, 55(5): 833-837. |
| [4] | 周鑫,李文智. 肾细胞癌极致保肾时代的冷思考[J]. 北京大学学报(医学版), 2022, 54(4): 595-598. |
| [5] | 梁银华,祖雄兵,程序,刘龙飞. 肾蒂旋转法辅助治疗后腹腔镜下腹侧肾肿瘤的肾部分切除术[J]. 北京大学学报(医学版), 2017, 49(4): 608-612. |
| [6] | 刘萌, 付占立, 邸丽娟, 张建华, 范岩, 张旭初, 王荣福. 利尿肾动态显像在单侧肾盂输尿管连接部狭窄患者的手术或保守治疗中的应用[J]. 北京大学学报(医学版), 2015, 47(4): 638-642. |
| [7] | 周利群,郑卫. 中心型肾肿瘤的腹腔镜肾部分切除术[J]. 北京大学学报(医学版), 2013, 45(4): 509-. |
|
||
