北京大学学报(医学版) ›› 2024, Vol. 56 ›› Issue (4): 673-679. doi: 10.19723/j.issn.1671-167X.2024.04.021
非转移性T3a肾细胞癌患者3年肿瘤特异性生存期预测
周泽臻,邓绍晖,颜野,张帆,郝一昌,葛力源,张洪宪,王国良,张树栋*( )
)
- 北京大学第三医院泌尿外科,北京 100191
Predicting the 3-year tumor-specific survival in patients with T3a non-metastatic renal cell carcinoma
Zezhen ZHOU,Shaohui DENG,Ye YAN,Fan ZHANG,Yichang HAO,Liyuan GE,Hongxian ZHANG,Guoliang WANG,Shudong ZHANG*()
- Department of Urology, Peking University Third Hospital, Beijing 100191, China
摘要:
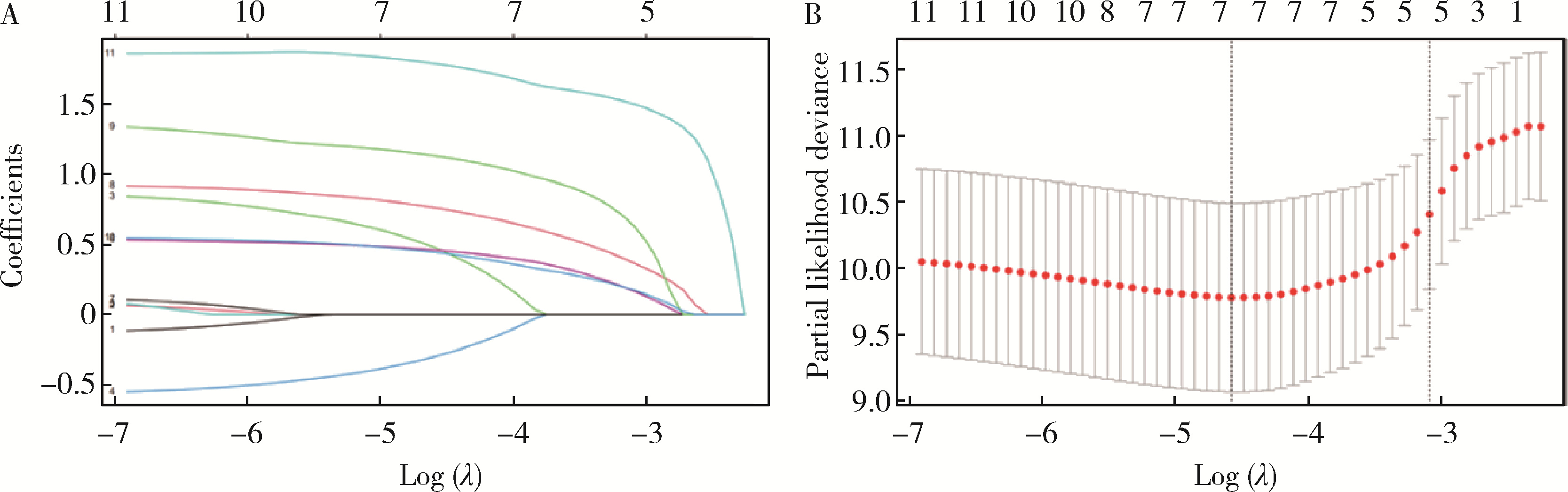
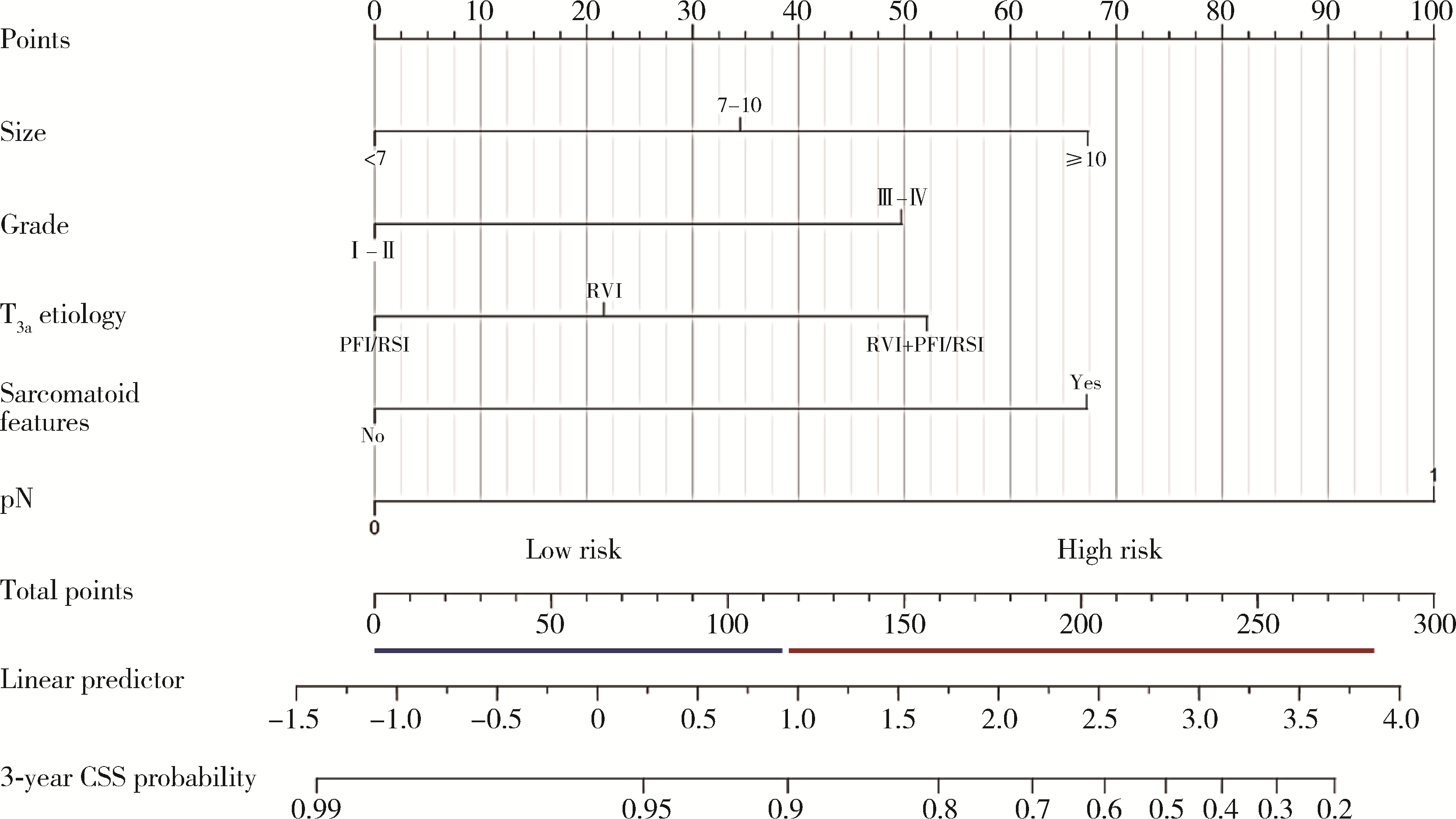
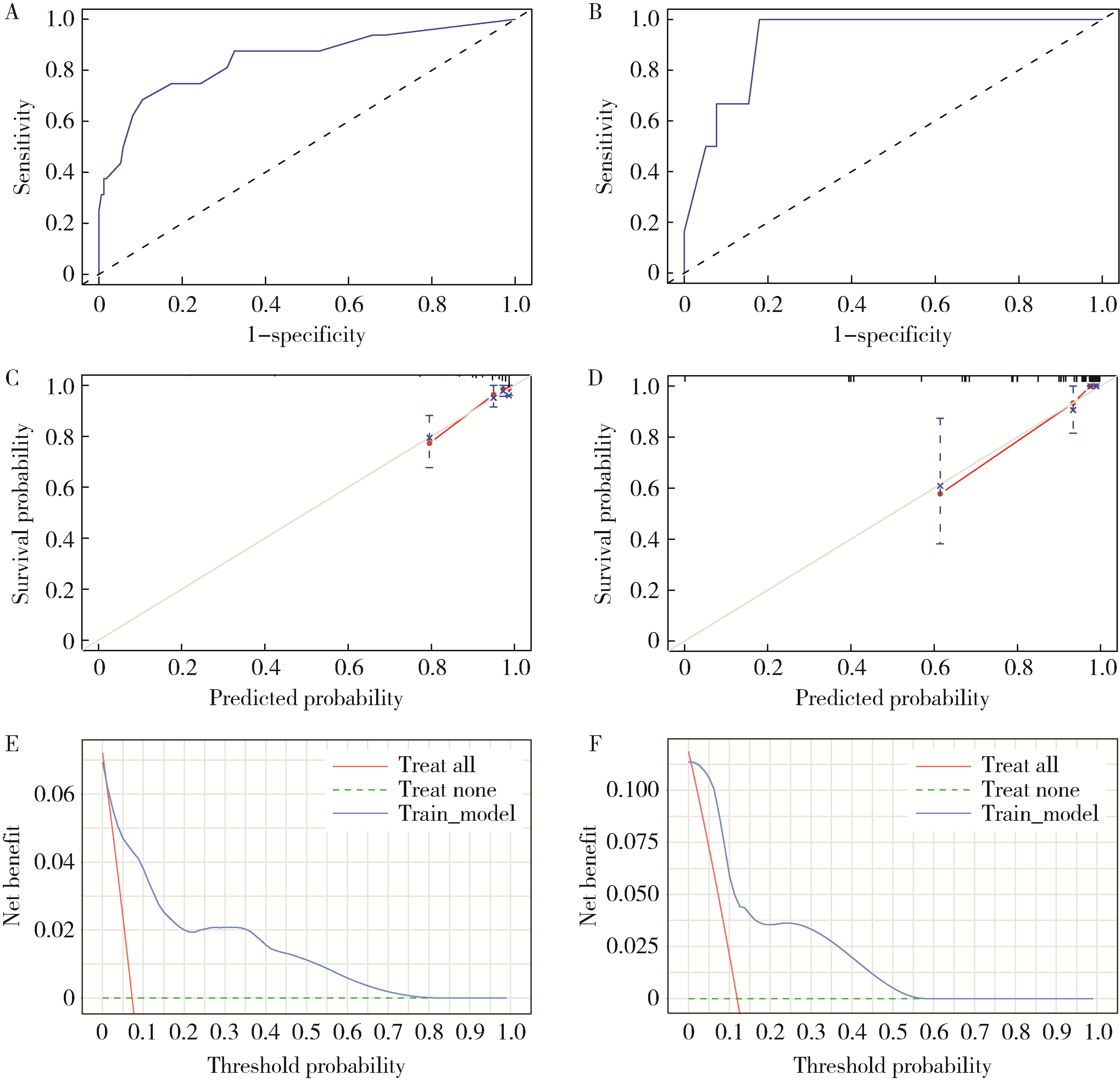
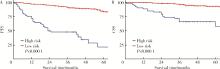
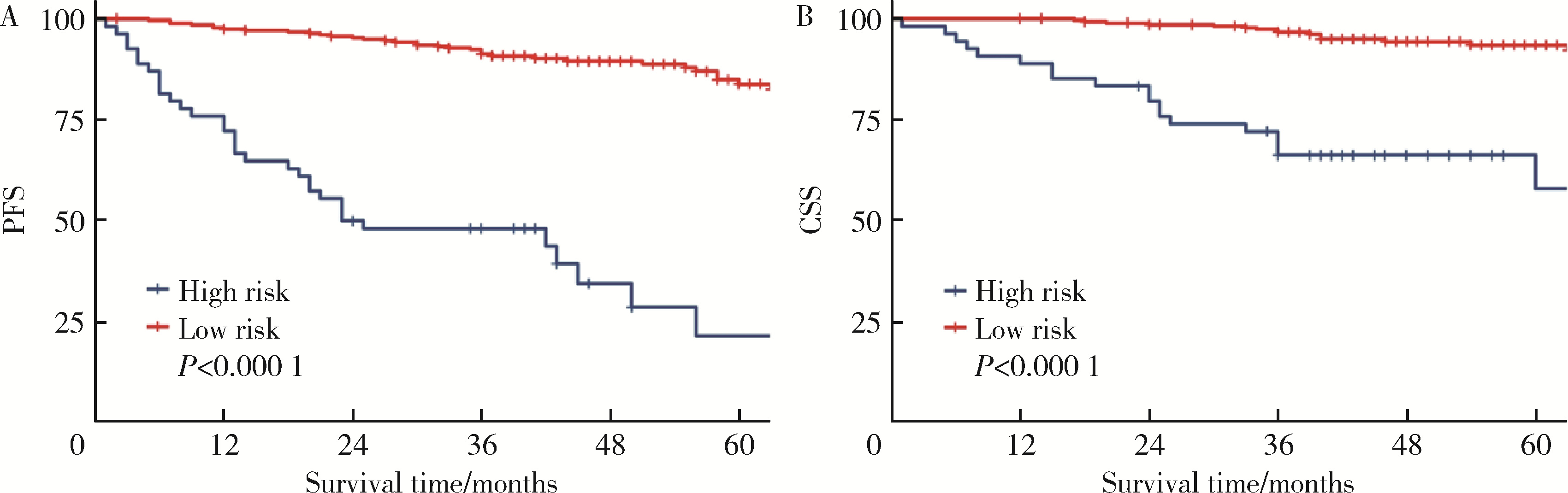
目的: 预测非转移性T3a肾细胞癌患者术后3年肿瘤特异性生存期(cancer specific survival, CSS)。方法: 选择2013年3月至2021年2月在北京大学第三医院泌尿外科行手术治疗且术后组织病理学诊断证实为T3aN0-1M0的肾细胞癌患者的病例资料进行回顾性分析,共收集到符合要求的患者336例,以4 ∶ 1的比例随机划分为训练队列(268例)和内部验证队列(68例)。采用双向Lasso回归筛选变量绘制预测T3aN0-1M0肾细胞癌患者术后3年CSS的列线图。利用一致性指数(C指数)、时间依赖性ROC曲线下面积(area under the curve,AUC)、校准曲线、决策曲线(decision curve analysis, DCA)来评估列线图的判别和校准能力及临床效益。根据列线图得分划分危险分层,并用Kaplan-Meier生存分析和Log-rank检验比较不同危险分层患者的无进展生存期(progress free survival, PFS)和CSS。结果: 训练队列和验证队列的基线资料组间差异均无统计学意义(P>0.05)。根据Lasso回归筛选结果,最终纳入肿瘤最大径、组织学分级、肉瘤样变、T3a特征、淋巴结转移5个变量构建列线图。列线图的训练队列和内部验证队列的一致性指数分别为0.808(0.708~0.907)、0.903(0.838~0.969);3年肿瘤特异性生存期的AUC分别为0.843(0.725~0.961)、0.923(0.844~1.002);各队列的校准曲线均显示实际CSS与预测概率之间具有高度的一致性;各队列的DCA曲线均显示列线图在临床上具有良好的净效益;两个队列共计336例患者,其中肿瘤特异性死亡35例,术后复发69例。根据列线图将0~117分的患者划分为低危组,119-284分的患者划分为高危组,其中低危组(282例)肿瘤特异性死亡16例,术后复发36例,高危组(54例)肿瘤特异性死亡19例,术后复发33例。低危组和高危组的PFS和CSS差异有统计学意义(P<0.000 1)。结论: 构建并验证了预测非转移性T3a肾细胞癌患者术后3年CSS的列线图预测模型,可协助临床精准评估此类患者的远期预后。
中图分类号:
- R737.11


| 1 |
Elkassem AA , Allen BC , Sharbidre KG , et al. Update on the role of imaging in clinical staging and restaging of renal cell carcinoma based on the AJCC 8th edition, from the AJR special series on cancer staging[J]. AJR Am J Roentgenol, 2021, 217 (3): 541- 555.
doi: 10.2214/AJR.21.25493 |
| 2 |
Guo P , Wang Y , Han Y , et al. Development and validation of a nomogram to predict postoperative cancer-specific survival of patients with nonmetastatic T3a renal cell carcinoma[J]. Urol Oncol, 2021, 39 (12): 835.e19- 835.e27.
doi: 10.1016/j.urolonc.2021.06.014 |
| 3 |
Musso G , Fallara G , Rosiello G , et al. Differential prognostic value of extrarenal involvement in patients with non-metastatic renal cell cancer[J]. Clin Genitourin Cancer, 2023, 21 (4): e279- e285.e1.
doi: 10.1016/j.clgc.2023.02.008 |
| 4 |
Shah PH , Lyon TD , Lohse CM , et al. Prognostic evaluation of perinephric fat, renal sinus fat, and renal vein invasion for patients with pathological stage T3a clear-cell renal cell carcinoma[J]. BJU Int, 2019, 123 (2): 270- 276.
doi: 10.1111/bju.14523 |
| 5 |
Li L , Shi L , Zhang J , et al. The critical impact of tumor size in predicting cancer special survival for T3aM0M0 renal cell carcinoma: A proposal of an alternative T3aN0M0 stage[J]. Cancer Med, 2021, 10 (2): 605- 614.
doi: 10.1002/cam4.3629 |
| 6 |
Lam JS , Klatte T , Patard JJ , et al. Prognostic relevance of tumour size in T3a renal cell carcinoma: A multicentre experience[J]. Eur Urol, 2007, 52 (1): 155- 162.
doi: 10.1016/j.eururo.2007.01.106 |
| 7 |
Tan WS , Koelker M , Campain N , et al. Comparison of long-term outcomes for young and healthy patients with cT1a and cT3a renal cell carcinoma treated with partial nephrectomy[J]. Eur Urol Focus, 2023, 9 (2): 333- 335.
doi: 10.1016/j.euf.2022.09.018 |
| 8 | Chung DY , Kang DH , Kim JW , et al. Comparison of oncologic outcomes between partial nephrectomy and radical nephrectomy in patients who were upstaged from cT1 renal tumor to pT3a renal cell carcinoma: An updated systematic review and meta-analysis[J]. Ther Adv Urol, 2020, 12, 1756287220981508. |
| 9 |
Deng H , Fan Y , Yuan F , et al. Partial nephrectomy provides equivalent oncologic outcomes and better renal function preservation than radical nephrectomy for pathological T3a renal cell carcinoma: A meta-analysis[J]. Int Braz J Urol, 2021, 47 (1): 46- 60.
doi: 10.1590/s1677-5538.ibju.2020.0167 |
| 10 |
Liu H , Kong QF , Li J , et al. A meta-analysis for comparison of partial nephrectomy vs. radical nephrectomy in patients with pT3a renal cell carcinoma[J]. Transl Androl Urol, 2021, 10 (3): 1170- 1178.
doi: 10.21037/tau-20-1262 |
| 11 |
Liu Z , Yang Z , Li J , et al. Partial versus radical nephrectomy for the treatment of pT3aN0M0 renal cell carcinoma: A propensity score analysis[J]. Asian J Surg, 2023, 46 (9): 3607- 3613.
doi: 10.1016/j.asjsur.2023.04.058 |
| [1] | 彭博, 刘芳芳, 杨伟, 徐瑞平, 陈蕾, 李保中, 王新家, 柯骥, 杨文蕾, 何煜, 刘震, 侯波林, 张利群, 林妙萍, 张立新, 张凡, 蔡奋, 许铧文, 刘萌飞, 刘英, 潘雅琪, 何忠虎, 柯杨. 围术期高血糖与食管切除术后食管鳞癌不良预后相关性[J]. 北京大学学报(医学版), 2026, 58(3): 567-574. |
| [2] | 舒帆, 葛力源, 邓汉彰, 殷昊明, 欧俊永, 邓绍晖, 郝一昌, 陆敏, 张展奕, 段佩辰, 张树栋. 预后不良的肾细胞癌伴淋巴结转移的分子特征[J]. 北京大学学报(医学版), 2026, 58(3): 631-640. |
| [3] | 王楠楠, 袁大晋, 朱昱冰, 丁磊. 结直肠癌根治术后肝转移风险多中心列线图预测模型的构建与验证[J]. 北京大学学报(医学版), 2026, 58(2): 290-300. |
| [4] | 张铃福, 陈明, 赵小宇, 王港, 崔龙, 凌晓锋, 王立新, 徐智, 郭丽梅, 侯纯升. 原发灶局限于胆囊壁内胆囊癌大体分型及其与预后和癌前病变的相关性[J]. 北京大学学报(医学版), 2026, 58(1): 184-189. |
| [5] | 高雅静, 李正芳, 马梦思, 武丽君. SII和SIRI对白塞病葡萄膜炎的风险预测及疾病活动度和预后的评估[J]. 北京大学学报(医学版), 2025, 57(6): 1067-1073. |
| [6] | 李博闻, 张强, 孙益鑫. 儿童及青年漏斗胸患者Nuss术后发生脊柱侧弯的风险预测模型建立及验证[J]. 北京大学学报(医学版), 2025, 57(5): 941-946. |
| [7] | 郭博达, 陆敏, 王国良, 张洪宪, 刘磊, 侯小飞, 赵磊, 田晓军, 张树栋. 肾透明细胞癌与非透明细胞癌伴静脉癌栓患者的临床病理特征及预后比较[J]. 北京大学学报(医学版), 2025, 57(4): 644-649. |
| [8] | 张展奕, 陆敏, 孙悦皓, 董靖晗, 侯小飞, 肖春雷, 王国良, 田晓军, 马潞林, 张洪宪, 张树栋. TFE3重排肾细胞癌合并静脉癌栓患者的临床病理特征及生存分析[J]. 北京大学学报(医学版), 2025, 57(4): 650-661. |
| [9] | 周泽臻, 葛力源, 张帆, 邓绍晖, 颜野, 张洪宪, 王国良, 刘磊, 黄毅, 张树栋. 病理T3a期肾细胞癌肾部分切除与根治性肾切除的回顾性匹配研究[J]. 北京大学学报(医学版), 2025, 57(4): 704-710. |
| [10] | 李伟浩, 李晶, 张学民, 李伟, 李清乐, 张小明. 术中回收式自体输血对颈动脉体瘤切除术后肿瘤预后的影响[J]. 北京大学学报(医学版), 2025, 57(2): 272-276. |
| [11] | 毛雅晴, 陈震, 于尧, 章文博, 刘洋, 彭歆. 2型糖尿病对口腔鳞状细胞癌患者预后的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1089-1096. |
| [12] | 刘园梅, 傅义程, 郝靖欣, 张福春, 刘慧琳. 老年髋部骨折患者住院期间发生术后心力衰竭的列线图预测模型的构建及验证[J]. 北京大学学报(医学版), 2024, 56(5): 874-883. |
| [13] | 李志存, 吴天俣, 梁磊, 范宇, 孟一森, 张骞. 穿刺活检单针阳性前列腺癌术后病理升级的危险因素分析及列线图模型构建[J]. 北京大学学报(医学版), 2024, 56(5): 896-901. |
| [14] | 欧俊永,倪坤明,马潞林,王国良,颜野,杨斌,李庚午,宋昊东,陆敏,叶剑飞,张树栋. 肌层浸润性膀胱癌合并中高危前列腺癌患者的预后因素[J]. 北京大学学报(医学版), 2024, 56(4): 582-588. |
| [15] | 刘帅,刘磊,刘茁,张帆,马潞林,田晓军,侯小飞,王国良,赵磊,张树栋. 伴静脉癌栓的肾上腺皮质癌的临床治疗及预后[J]. 北京大学学报(医学版), 2024, 56(4): 624-630. |
|
||
