北京大学学报(医学版) ›› 2024, Vol. 56 ›› Issue (4): 624-630. doi: 10.19723/j.issn.1671-167X.2024.04.013
伴静脉癌栓的肾上腺皮质癌的临床治疗及预后
刘帅,刘磊,刘茁,张帆,马潞林,田晓军,侯小飞,王国良,赵磊,张树栋*( )
)
- 北京大学第三医院泌尿外科, 北京 100191
Clinical treatment and prognosis of adrenocortical carcinoma with venous tumor thrombus
Shuai LIU,Lei LIU,Zhuo LIU,Fan ZHANG,Lulin MA,Xiaojun TIAN,Xiaofei HOU,Guoliang WANG,Lei ZHAO,Shudong ZHANG*()
- Department of Urology, Peking University Third Hospital, Beijing 100191, China
摘要:
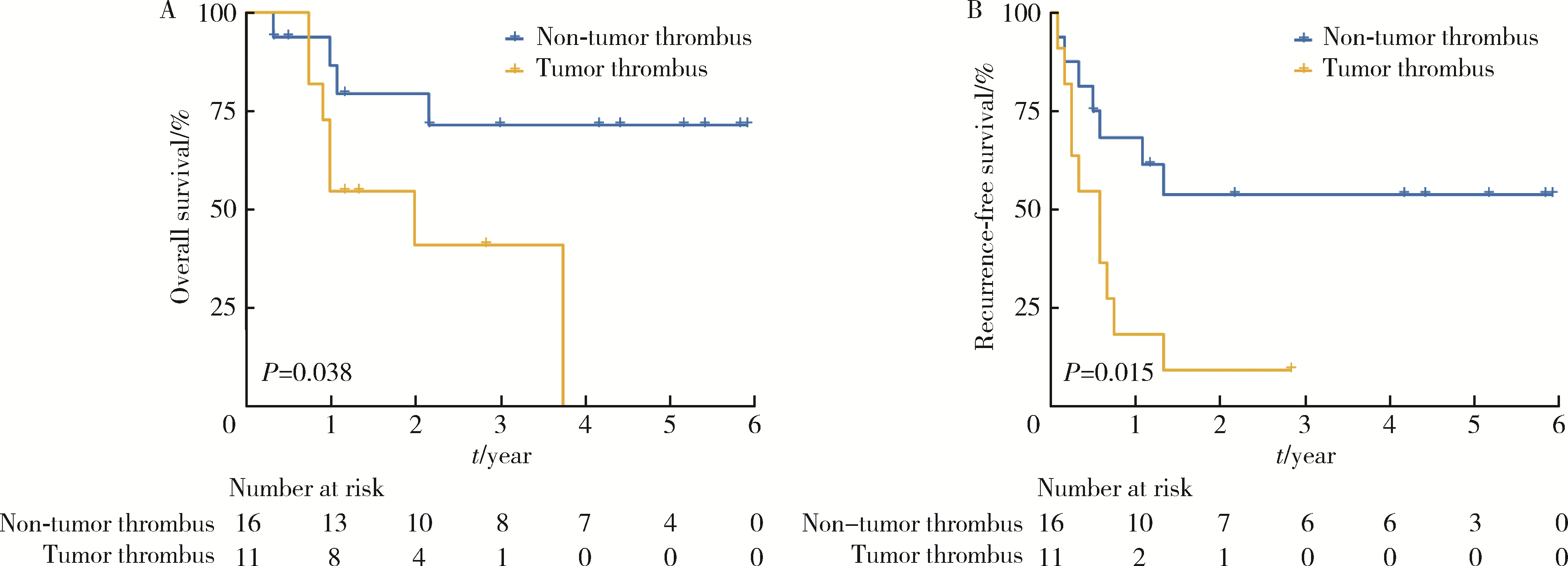
目的: 分析肾上腺皮质癌伴静脉癌栓患者的临床病理特征、预后,并总结手术治疗经验。方法: 回顾性分析北京大学第三医院泌尿外科2018—2023年接受手术治疗的肾上腺皮质癌患者的相关数据,将其分为伴静脉癌栓组和不伴静脉癌栓组。采用Wilcoxon秩和检验比较定量变量,卡方检验/Fisher精确检验比较分类变量,采用Kaplan-Meier法计算生存率。结果: 共纳入27例肾上腺皮质癌患者,其中11例(40.7%)伴静脉癌栓,包括8例女性,3例男性,中位年龄49(36,58)岁,中位体重指数26.0(24.1,30.4) kg/m2;7例初诊时有症状,6例有高血压病史,2例皮质醇水平增高;中位肿瘤直径9.4(6.5,12.5) cm。3例肿瘤侧别为左侧,其中1例局限在左肾上腺中央静脉未侵入左肾静脉,2例癌栓生长达肝下下腔静脉;8例肿瘤侧别为右侧,其中1例在右肾上腺中央静脉未侵入下腔静脉,4例侵入肝下下腔静脉,3例生长达肝后下腔静脉。10例患者为欧洲肾上腺肿瘤研究协作网(European Network for the Study of Adrenal Tumors,ENSAT)临床分期Ⅲ期,1例为Ⅳ期。手术方式为开放手术6例,单纯腹腔镜手术者4例,机器人辅助腹腔镜手术1例;2例切除同侧肾脏;中位手术时间332(261,440) min,术中中位出血量900(700,2 200) mL,术后中位住院时间9(5,10) d;中位生存时间24.0个月,中位复发时间7.0个月,16例不伴静脉癌栓患者均未达到中位生存时间和中位复发时间。与不伴静脉癌栓组相比,静脉癌栓组有更差的3年总体生存(overall survival,OS)率(71.4% vs. 40.9%;Log-rank,P=0.038)和2年无复发生存(recurrence-free survival,RFS)率(53.7% vs. 9.1%;Log-rank,P=0.015)。结论: 肾上腺皮质癌伴静脉癌栓患者预后较差,肾上腺肿瘤切除术和静脉癌栓取出术治疗该疾病安全有效。
中图分类号:
- R699.3

| 1 |
Calissendorff J , Calissendorff F , Falhammar H . Adrenocortical cancer: Mortality, hormone secretion, proliferation and urine ste-roids: Experience from a single centre spanning three decades[J]. BMC Endocr Disord, 2016, 16, 15.
doi: 10.1186/s12902-016-0095-9 |
| 2 |
De Filpo G , Mannelli M , Canu L . Adrenocortical carcinoma: Current treatment options[J]. Curr Opin Oncol, 2021, 33 (1): 16- 22.
doi: 10.1097/CCO.0000000000000695 |
| 3 |
Brönimann S , Garstka N , Remzi M . Treatment of adrenocortical carcinoma: Oncological and endocrine outcomes[J]. Curr Opin Urol, 2023, 33 (1): 50- 58.
doi: 10.1097/MOU.0000000000001045 |
| 4 |
Xu WH , Wu J , Wang J , et al. Screening and identification of potential prognostic biomarkers in adrenocortical carcinoma[J]. Front Genet, 2019, 10, 821.
doi: 10.3389/fgene.2019.00821 |
| 5 | 邓建华, 李汉忠, 纪志刚, 等. 肾上腺皮质癌的综合治疗[J]. 北京大学学报(医学版), 2019, 51 (2): 298- 301. |
| 6 |
Quinones-Baldrich W , Alktaifi A , Eilber F , et al. Inferior vena cava resection and reconstruction for retroperitoneal tumor excision[J]. J Vasc Surg, 2012, 55 (5): 1386- 1393.
doi: 10.1016/j.jvs.2011.11.054 |
| 7 |
Schwarzbach MH , Hormann Y , Hinz U , et al. Clinical results of surgery for retroperitoneal sarcoma with major blood vessel involvement[J]. J Vasc Surg, 2006, 44 (1): 46- 55.
doi: 10.1016/j.jvs.2006.03.001 |
| 8 |
Nooromid MJ , Ju MH , Havelka GE , et al. Fifteen-year expe-rience with renal cell carcinoma with associated venous tumor thrombus[J]. Surgery, 2016, 160 (4): 915- 923.
doi: 10.1016/j.surg.2016.06.029 |
| 9 |
Shao P , Li J , Qin C , et al. Laparoscopic radical nephrectomy and inferior vena cava thrombectomy in the treatment of renal cell carcinoma[J]. Eur Urol, 2015, 68 (1): 115- 122.
doi: 10.1016/j.eururo.2014.12.011 |
| 10 |
Agochukwu N , Shuch B . Clinical management of renal cell carcinoma with venous tumor thrombus[J]. World J Urol, 2014, 32 (3): 581- 589.
doi: 10.1007/s00345-014-1276-7 |
| 11 |
Fairweather M , Raut CP . Nephrectomy for retroperitoneal sarcoma: Stay calm and (cautiously) carry on[J]. Ann Surg Oncol, 2021, 28 (3): 1275- 1277.
doi: 10.1245/s10434-020-09293-w |
| 12 |
Liu Z , Ge L , Liu L , et al. Clinical experience and management strategy of retroperitoneal tumor with venous tumor thrombus involvement[J]. Front Oncol, 2022, 12, 873729.
doi: 10.3389/fonc.2022.873729 |
| 13 | Jannello LMI, Incesu RB, Morra S, et al. The European Network for the Study of Adrenal Tumors staging system (2015): A United States validation[J/OL]. J Clin Endocrinol Metab, 2024: dgae047[2024-02-18]. doi: 10.1210/clinem/dgae047. |
| 14 |
Liu Z , Zhao X , Ge L , et al. Completely laparoscopic versus open radical nephrectomy and infrahepatic tumor thrombectomy: Comparison of surgical complexity and prognosis[J]. Asian J Surg, 2021, 44 (4): 641- 648.
doi: 10.1016/j.asjsur.2020.12.003 |
| 15 |
Zhang G , Li X , Sun G , et al. Clinical analysis of Kimura's di-sease in 24 cases from China[J]. BMC Surg, 2020, 20 (1): 1.
doi: 10.1186/s12893-019-0673-7 |
| 16 |
Liu Z , Li Y , Zhang Y , et al. PUTH grading system for urinary tumor with supradiaphragmatic tumor thrombus: Different surgical techniques for different tumor characteristics[J]. Front Oncol, 2022, 11, 735145.
doi: 10.3389/fonc.2021.735145 |
| 17 |
Blute ML , Leibovich BC , Lohse CM , et al. The Mayo clinic experience with surgical management, complications and outcome for patients with renal cell carcinoma and venous tumour thrombus[J]. BJU Int, 2004, 94 (1): 33- 41.
doi: 10.1111/j.1464-410X.2004.04897.x |
| 18 |
Laan DV , Thiels CA , Glasgow A , et al. Adrenocortical carcinoma with inferior vena cava tumor thrombus[J]. Surgery, 2017, 161 (1): 240- 248.
doi: 10.1016/j.surg.2016.07.040 |
| 19 |
Piardi T , Lhuaire M , Memeo R , et al. Laparoscopic Pringle maneuver: How we do it?[J]. Hepatobiliary Surg Nutr, 2016, 5 (4): 345- 349.
doi: 10.21037/hbsn.2015.11.01 |
| 20 |
Fiore M , Colombo C , Locati P , et al. Surgical technique, morbi-dity, and outcome of primary retroperitoneal sarcoma involving inferior vena cava[J]. Ann Surg Oncol, 2012, 19 (2): 511- 518.
doi: 10.1245/s10434-011-1954-2 |
| 21 | 刘磊, 王国良, 马潞林, 等. 肾上腺区巨大肿瘤合并瘤栓的诊断与治疗[J]. 北京大学学报(医学版), 2019, 51 (4): 684- 688. |
| 22 |
杨华安, 郭胜杰. 肾上腺皮质癌合并静脉癌栓的手术治疗及预后[J]. 实用医学杂志, 2020, 36 (10): 1344- 1348.
doi: 10.3969/j.issn.1006-5725.2020.10.015 |
| 23 |
Zhao X , Liu Z , Zhang H , et al. PKUTHLP score: A comprehensive system to predict surgical approach in radical nephrectomy and thrombectomy[J]. Oncol Lett, 2020, 20 (1): 201- 208.
doi: 10.3892/ol.2020.11571 |
| 24 | Vuong NS , Ferriere JM , Michiels C , et al. Robot-assisted versus open surgery for radical nephrectomy with level 1-2 vena cava tumor thrombectomy: A French monocenter experience (UroCCR study #73)[J]. Minerva Urol Nephrol, 2021, 73 (4): 498- 508. |
| 25 |
Treiger BF , Humphrey LS , Peterson CV , et al. Transesophageal echocardiography in renal cell carcinoma: An accurate diagnostic technique for intracaval neoplastic extension[J]. J Urol, 1991, 145 (6): 1138- 1140.
doi: 10.1016/S0022-5347(17)38556-7 |
| [1] | 欧俊永,倪坤明,马潞林,王国良,颜野,杨斌,李庚午,宋昊东,陆敏,叶剑飞,张树栋. 肌层浸润性膀胱癌合并中高危前列腺癌患者的预后因素[J]. 北京大学学报(医学版), 2024, 56(4): 582-588. |
| [2] | 虞乐,邓绍晖,张帆,颜野,叶剑飞,张树栋. 具有低度恶性潜能的多房囊性肾肿瘤的临床病理特征及预后[J]. 北京大学学报(医学版), 2024, 56(4): 661-666. |
| [3] | 周泽臻,邓绍晖,颜野,张帆,郝一昌,葛力源,张洪宪,王国良,张树栋. 非转移性T3a肾细胞癌患者3年肿瘤特异性生存期预测[J]. 北京大学学报(医学版), 2024, 56(4): 673-679. |
| [4] | 方杨毅,李强,黄志高,陆敏,洪锴,张树栋. 睾丸鞘膜高分化乳头状间皮肿瘤1例[J]. 北京大学学报(医学版), 2024, 56(4): 741-744. |
| [5] | 曾媛媛,谢云,陈道南,王瑞兰. 脓毒症患者发生正常甲状腺性病态综合征的相关因素[J]. 北京大学学报(医学版), 2024, 56(3): 526-532. |
| [6] | 苏俊琪,王晓颖,孙志强. 舌鳞状细胞癌根治性切除术后患者预后预测列线图的构建与验证[J]. 北京大学学报(医学版), 2024, 56(1): 120-130. |
| [7] | 李建斌,吕梦娜,池强,彭一琳,刘鹏程,吴锐. 干燥综合征患者发生重症新型冠状病毒肺炎的早期预测[J]. 北京大学学报(医学版), 2023, 55(6): 1007-1012. |
| [8] | 刘欢锐,彭祥,李森林,苟欣. 基于HER-2相关基因构建风险模型用于膀胱癌生存预后评估[J]. 北京大学学报(医学版), 2023, 55(5): 793-801. |
| [9] | 薛子璇,唐世英,邱敏,刘承,田晓军,陆敏,董靖晗,马潞林,张树栋. 青年肾肿瘤伴瘤栓的临床病理特征及预后分析[J]. 北京大学学报(医学版), 2023, 55(5): 802-811. |
| [10] | 兰东,刘茁,李宇轩,王国良,田晓军,马潞林,张树栋,张洪宪. 根治性肾切除和静脉癌栓取出术大出血的危险因素[J]. 北京大学学报(医学版), 2023, 55(5): 825-832. |
| [11] | 卢汉,张建运,杨榕,徐乐,李庆祥,郭玉兴,郭传瑸. 下颌牙龈鳞状细胞癌患者预后的影响因素[J]. 北京大学学报(医学版), 2023, 55(4): 702-707. |
| [12] | 时云飞,王豪杰,刘卫平,米岚,龙孟平,刘雁飞,赖玉梅,周立新,刁新婷,李向红. 血管免疫母细胞性T细胞淋巴瘤临床与分子病理学特征分析[J]. 北京大学学报(医学版), 2023, 55(3): 521-529. |
| [13] | 朱晓娟,张虹,张爽,李东,李鑫,徐玲,李挺. 人表皮生长因子受体2低表达乳腺癌的临床病理学特征及预后[J]. 北京大学学报(医学版), 2023, 55(2): 243-253. |
| [14] | 赖玉梅,李忠武,李欢,吴艳,时云飞,周立新,楼雨彤,崔传亮. 68例肛管直肠黏膜黑色素瘤临床病理特征及预后[J]. 北京大学学报(医学版), 2023, 55(2): 262-269. |
| [15] | 沈棋,刘亿骁,何群. 肾黏液样小管状和梭形细胞癌的临床病理特点及预后[J]. 北京大学学报(医学版), 2023, 55(2): 276-282. |
| Viewed | ||||||||||||||||||||||||||||||||||||||||||||||||||
|
Full text 46
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
Abstract 182
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
Cited |
|
|||||||||||||||||||||||||||||||||||||||||||||||||
| Shared | ||||||||||||||||||||||||||||||||||||||||||||||||||
| Discussed | ||||||||||||||||||||||||||||||||||||||||||||||||||
|
||
