北京大学学报(医学版) ›› 2024, Vol. 56 ›› Issue (4): 631-635. doi: 10.19723/j.issn.1671-167X.2024.04.014
经食管超声心动图在肾切除术联合Mayo Ⅲ~Ⅳ级静脉瘤栓取栓术不同手术方式中的临床作用
杨捷1,冯杰莉1,*( ),张树栋2,马潞林2,郑清3
),张树栋2,马潞林2,郑清3
- 1. 北京大学第三医院心血管内科, 北京 100191
2. 北京大学第三医院泌尿外科, 北京 100191
3. 北京大学第三医院麻醉科, 北京 100191
Clinical effects of transesophageal echocardiography in different surgical methods for nephrectomy combined with Mayo Ⅲ-Ⅳ vena tumor thrombectomy
Jie YANG1,Jieli FENG1,*(),Shudong ZHANG2,Lulin MA2,Qing ZHENG3
- 1. Department of Cardiology, Peking University Third Hospital, Beijing 100191, China
2. Department of Urology, Peking University Third Hospital, Beijing 100191, China
3. Department of Anesthesiology, Peking University Third Hospital, Beijing 100191, China
摘要:
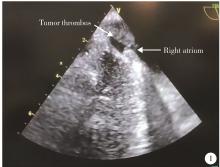
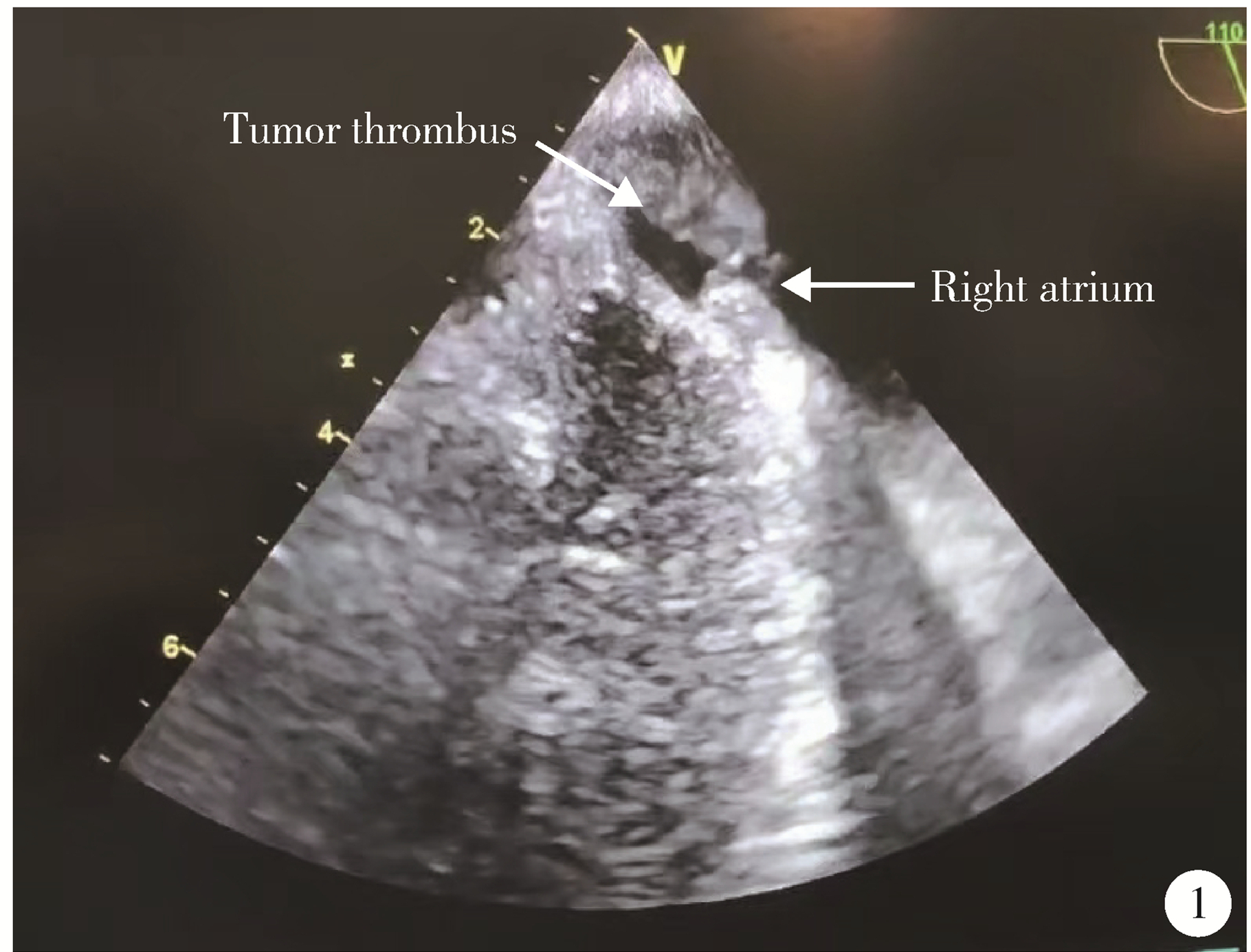
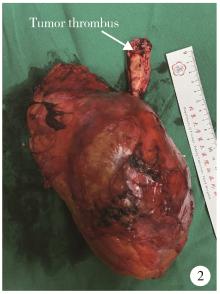
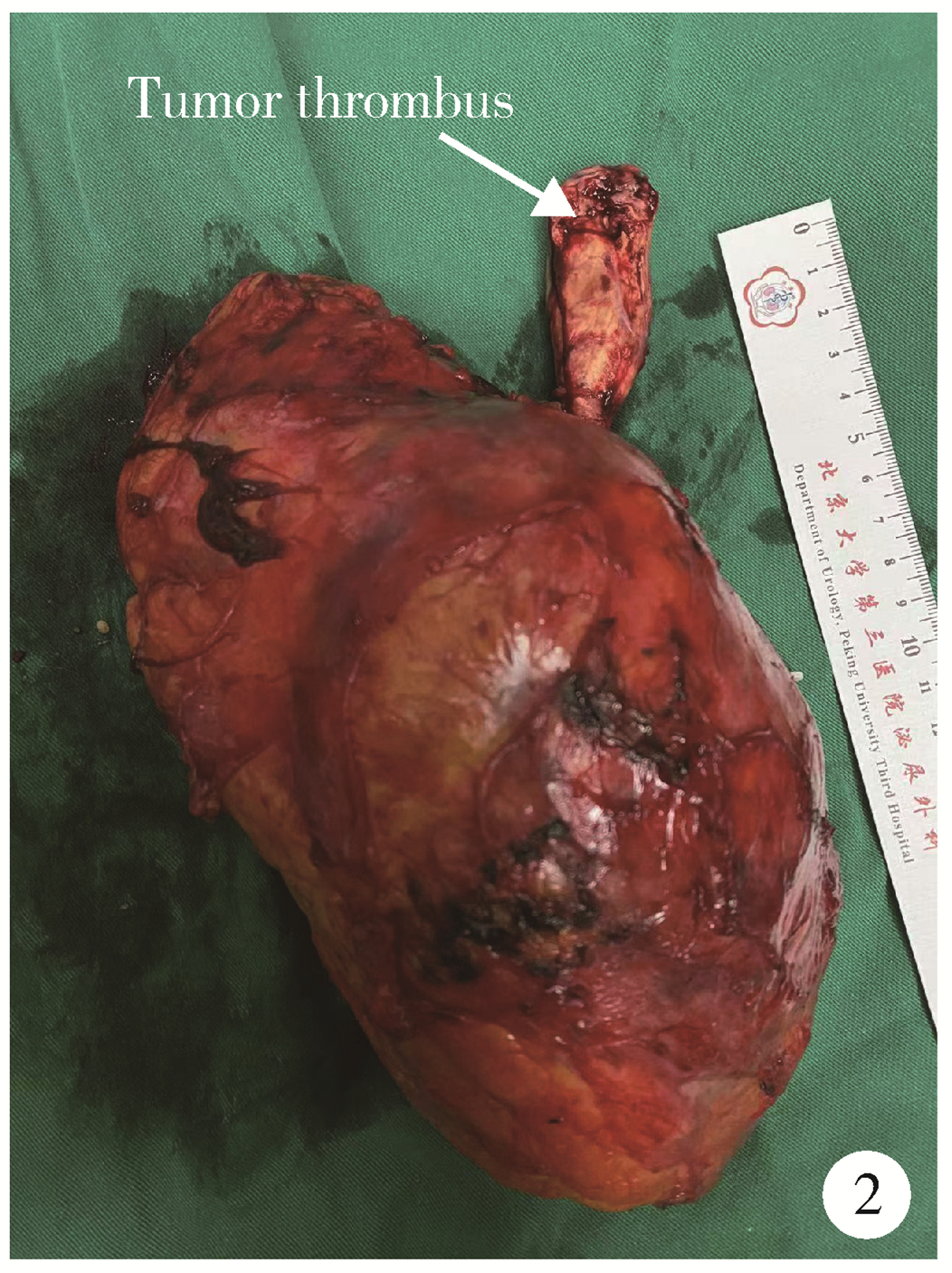
目的: 比较经食管超声心动图(transesophageal echocardiography,TEE)在肾切除术联合下腔静脉Mayo Ⅲ~Ⅳ级瘤栓取栓术不同手术方式中的临床作用。方法: 纳入2022年1月至2024年2月在北京大学第三医院行根治性肾切除联合Mayo Ⅲ~Ⅳ级瘤栓取栓手术的患者28例,其中,机器人手术16例,腹腔镜手术2例,开腹手术10例,收集患者的各项临床资料进行分析比较。结果: 机器人手术的患者中有9例采用TEE,其中7例术中TEE影像结果较术前发生变化,包括2例术中TEE提示瘤栓进入右心房,2例显示下腔静脉瘤栓由Mayo Ⅲ级升至Ⅳ级,3例提示瘤栓与下腔静脉粘连,及时调整了手术方案;开腹手术的患者中有6例采用TEE,其中4例术中TEE提示Mayo分级较术前发生变化,包括3例提示瘤栓与下腔静脉粘连,1例提示瘤栓伴血栓形成,调整了手术方案,旷置或节段性切除瘤栓;腹腔镜手术的2例患者未采用术中TEE。术中采用TEE的作用包括开腹手术术中探查结合TEE监测瘤栓切除过程,机器人手术完全通过TEE监测瘤栓脱出,术中TEE还实时监测患者循环状态和心脏功能变化。结论: 肾切除术联合Mayo Ⅲ~Ⅳ级瘤栓取栓术的不同术式中,术中TEE均可再次确定瘤栓分级、粘连程度,并实时动态跟踪取栓过程,监测患者循环状态和心脏功能变化,具有重要的辅助作用,但其临床应用仍不足,建议这类手术均采用术中TEE。
中图分类号:
- R737.11
| 1 |
中华医学会泌尿外科学分会中国肾癌联盟, 中国肾癌伴下腔静脉癌栓诊疗协作组. 肾癌伴静脉癌栓诊治专家共识[J]. 中华泌尿外科杂志, 2018, 39 (12): 881- 884.
doi: 10.3760/cma.j.issn.1000-6702.2018.12.001 |
| 2 | 马潞林, 邱敏, 田晓军, 等. 改良泌尿系统肿瘤伴静脉癌栓的诊断与治疗[M]. 北京: 北京大学医学出版社, 2024: 75- 81. |
| 3 |
赵勋, 刘茁, 马潞林. 肾癌合并Mayo Ⅳ级下腔静脉癌栓的诊治进展[J]. 中华泌尿外科杂志, 2019, 40 (6): 471- 473.
doi: 10.3760/cma.j.issn.1000-6702.2019.06.021 |
| 4 | 王迎春, 孔延亮, 刘钰苇, 等. 术前CTA评估大体积肾癌肾动静脉解剖及癌栓[J]. 中国介入影像与治疗学, 2020, 17 (9): 561- 564. |
| 5 | 马鑫, 何志嵩, 马潞林, 等. 机器人肾癌伴静脉癌栓切除术专家共识[J]. 微创泌尿外科杂志, 2023, 12 (1): 1- 7. |
| 6 |
Jurado A , Romeo A , Gueglio G , et al. Current trends in management of renal cell carcinoma with venous thrombus extension[J]. Curr Urol Rep, 2021, 22 (4): 23- 31.
doi: 10.1007/s11934-021-01036-y |
| 7 |
Yuan SM . Surgical treatment of renal cell carcinoma with inferior vena cava tumor thrombus[J]. Surg Today, 2022, 52 (8): 1125- 1133.
doi: 10.1007/s00595-021-02429-9 |
| 8 | 严旭芝, 王硕, 刘秋礼, 等. 根治性肾切除联合下腔静脉癌栓取出机器人辅助与开放手术的临床疗效对比[J]. 陆军军医大学学报, 2023, 45 (20): 2099- 2105. |
| 9 |
彭程, 黄庆波, 陈勇辉, 等. 肾癌伴Mayo Ⅳ级下腔静脉瘤栓不同术式疗效的多中心回顾性研究[J]. 中华泌尿外科杂志, 2022, 43 (5): 324- 329.
doi: 10.3760/cma.j.cn112330-20220317-00121 |
| 10 |
Bissada NK , Yakout HH , Babanouri A , et al. Longterm expe-rience with management of renal cell carcinoma involving the inferior vena cava[J]. Urology, 2003, 61 (1): 89- 92.
doi: 10.1016/S0090-4295(02)02119-2 |
| 11 | 李丽伟, 刘茁驰, 王国良, 等. 肾癌伴下腔静脉瘤栓合并血栓的多种影像学比较[J]. 北京大学学报(医学版), 2019, 51 (4): 678- 683. |
| 12 | 贾江华, 李旭泽, 王凤, 等. 经食道超声心动图在肾癌伴下腔静脉癌栓手术治疗中的应用[J]. 中国医学科学院学报, 2023, 45 (1): 28- 32. |
| 13 |
Meersch M , Schmidt C , Zarbock A . Echophysiology: The transesophageal echo probe as a noninvasive Swan-Ganz catheter[J]. Curr Opin Anaesthesiol, 2016, 29 (1): 36- 45.
doi: 10.1097/ACO.0000000000000277 |
| 14 |
Hahn RT , Abraham T , Adams MS , et al. Guidelines for perfor-ming a comprehensive transesophageal echocardiographic examination: Recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists[J]. J Am Soc Echocardiogr, 2013, 26 (9): 921- 964.
doi: 10.1016/j.echo.2013.07.009 |
| [1] | 张启鸣, 陈泽波, 田雨, 潘大猛, 刘磊, 张洪宪, 赵磊, 张树栋, 马潞林, 侯小飞. 机器人辅助腹腔镜移植肾切除术经验总结[J]. 北京大学学报(医学版), 2025, 57(4): 666-669. |
| [2] | 周泽臻, 葛力源, 张帆, 邓绍晖, 颜野, 张洪宪, 王国良, 刘磊, 黄毅, 张树栋. 病理T3a期肾细胞癌肾部分切除与根治性肾切除的回顾性匹配研究[J]. 北京大学学报(医学版), 2025, 57(4): 704-710. |
| [3] | 庄金满,李天润,李选,栾景源,王昌明,冯琦琛,韩金涛. Rotarex旋切导管在股腘动脉狭窄合并血栓形成中的应用[J]. 北京大学学报(医学版), 2023, 55(2): 328-332. |
| [4] | 张铨,宋海峰,马冰磊,张喆楠,周朝晖,李傲林,刘军,梁磊,朱时雨,张骞. 术前预后营养指数可作为预测非转移性肾细胞癌预后的指标[J]. 北京大学学报(医学版), 2023, 55(1): 149-155. |
| [5] | 周利群,徐纯如. 机器人时代中央型肾肿瘤的手术治疗策略[J]. 北京大学学报(医学版), 2022, 54(4): 587-591. |
| [6] | 庄金满,李天润,李选,栾景源,王昌明,冯琦琛,韩金涛. Rotarex经皮机械性血栓切除装置在急性下肢缺血中的应用[J]. 北京大学学报(医学版), 2021, 53(6): 1159-1162. |
| [7] | 韩松辰,黄子雄,刘慧鑫,徐涛. 单侧肾细胞癌根治性切除术后的肾功能代偿[J]. 北京大学学报(医学版), 2021, 53(4): 680-685. |
| [8] | 李新飞, 彭意吉, 余霄腾, 熊盛炜, 程嗣达, 丁光璞, 杨昆霖, 唐琦, 米悦, 吴静云, 张鹏, 谢家馨, 郝瀚, 王鹤, 邱建星, 杨建, 李学松, 周利群. 肾部分切除术前CT三维可视化评估标准的初步探究[J]. 北京大学学报(医学版), 2021, 53(3): 613-622. |
| [9] | 叶雄俊,刘军,安立哲,熊六林,徐涛,黄晓波. 麦氏点斜切口在全腹腔镜下肾输尿管全长切除术中的应用[J]. 北京大学学报(医学版), 2018, 50(4): 762-封三. |
| [10] | 赵磊, 马潞林, 张洪宪, 侯小飞, 刘磊, 付燕, 寇允更, 宋一萌. 后腹腔镜活体供肾切取193例[J]. 北京大学学报(医学版), 2017, 49(5): 867-871. |
| [11] | 彭鼎,李学松,张崔建,杨恺惟,唐琦,张雷,余霄腾,何志嵩,周利群. T3N0M0期肾细胞癌患者预后相关因素分析:单中心182例患者回顾性研究[J]. 北京大学学报(医学版), 2016, 48(5): 806-811. |
| [12] | 马潞林, 宋诗雨. 开放手术治疗肾细胞癌伴下腔静脉癌栓[J]. 北京大学学报(医学版), 2015, 47(4): 566-568. |
| [13] | 邱敏, 卢剑, 马潞林, 颜野, 张树栋. 后腹腔镜肾部分切除术治疗囊性肾瘤1例[J]. 北京大学学报(医学版), 2014, 46(4): 650-652. |
| [14] | 张树栋, 马潞林, 黄毅, 张洪宪, 刘可, 邱敏. 改良Pfannenstiel切口取肾的经腹途径腹腔镜肾癌根治术[J]. 北京大学学报(医学版), 2014, 46(4): 638-641. |
| [15] | 杨洋, 肖云翔, 周利群, 何志嵩, 金杰. 手术治疗肾癌根治术后孤立局部复发病灶的长期预后分析[J]. 北京大学学报(医学版), 2014, 46(4): 528-531. |
|
||
