北京大学学报(医学版) ›› 2025, Vol. 57 ›› Issue (2): 284-290. doi: 10.19723/j.issn.1671-167X.2025.02.010
链球菌感染与过敏性紫癜肾炎患儿肾损害的相关性
王紫薇1, 李闵1, 高慧1,2, 邓芳1,2,3,*( )
)
- 1. 安徽医科大学第一附属医院儿科,合肥 230032
2. 出生人口健康教育部重点实验室,合肥 230032
3. 安徽省立儿童医院儿童肾脏内科,合肥 230051
Correlation between streptococcal infection and renal damage in children with Henoch-Schönlein purpura nephritis
Ziwei WANG1, Min LI1, Hui GAO1,2, Fang DENG1,2,3,*()
- 1. Department of Pediatrics, the First Affiliated Hospital of Anhui Medical University, Hefei 230032, China
2. Key Laboratory of Ministry of Education for Birth Population Health, Hefei 230032, China
3. Department of Nephrology, Anhui Provincial Children's Hospital, Hefei 230051, China
摘要:
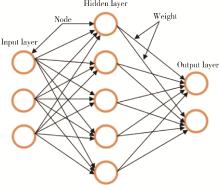
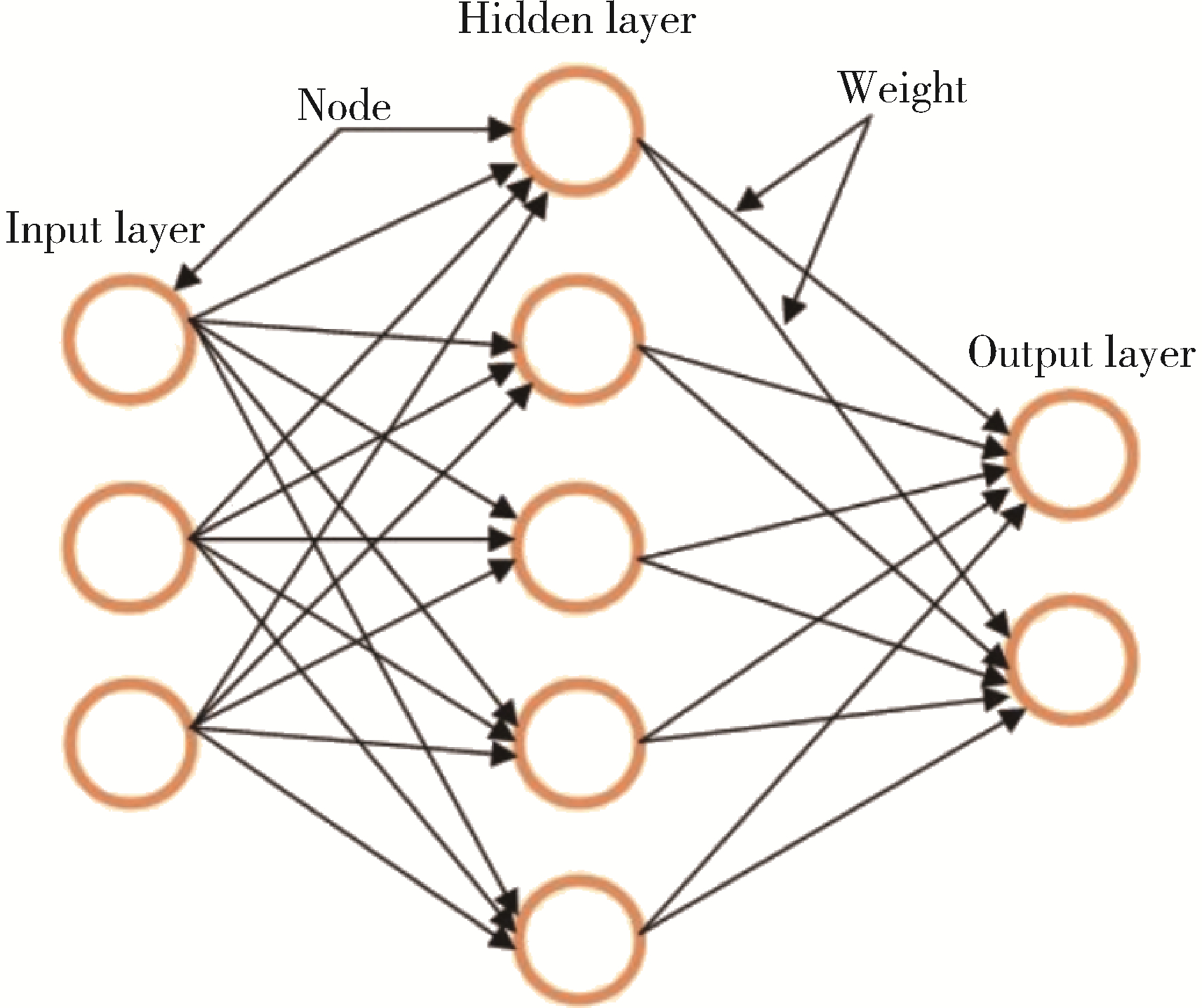
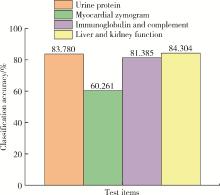
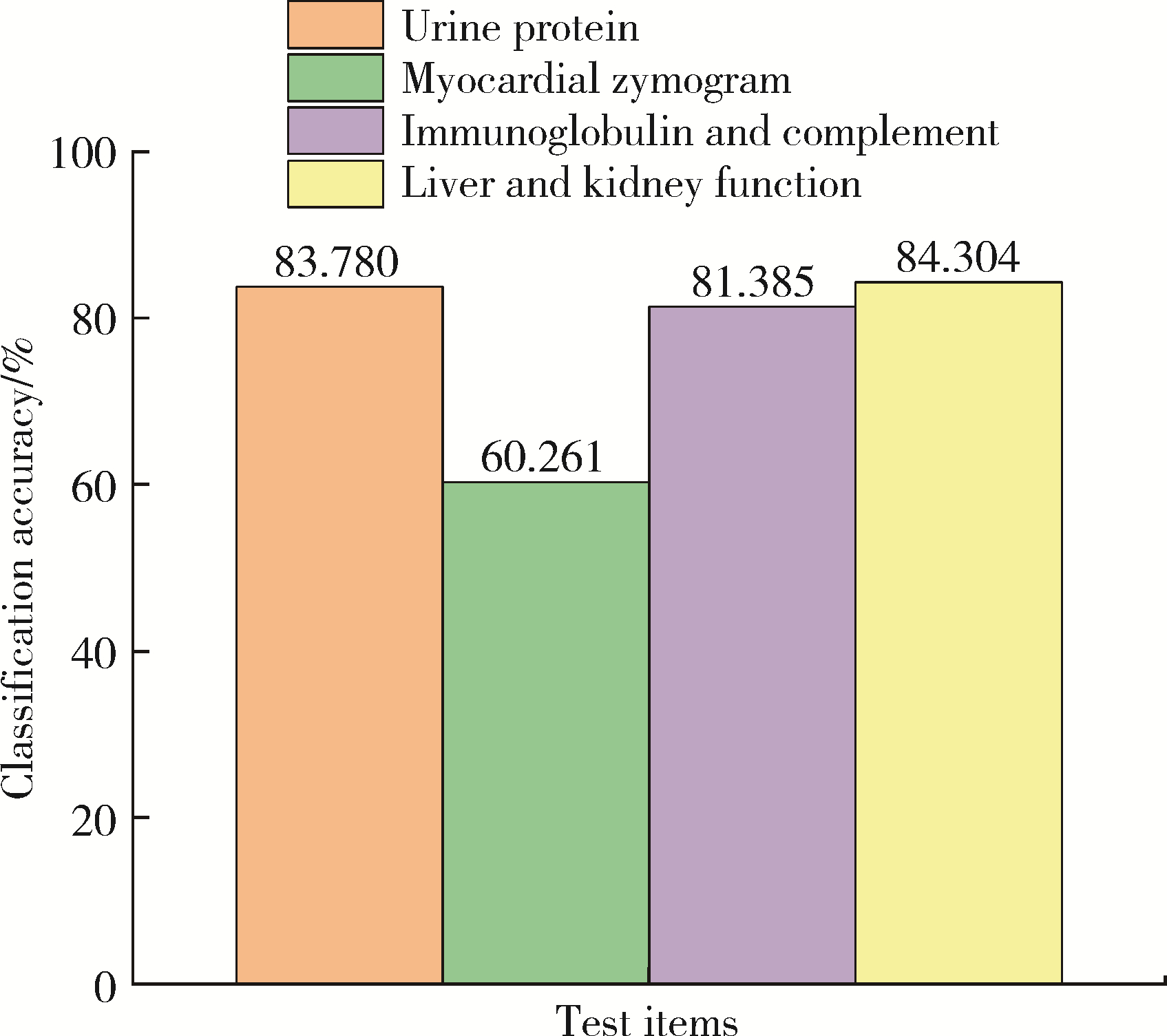
目的: 探讨链球菌(Streptococcus)感染是否有可能加重过敏性紫癜肾炎患儿的肾损害及可能机制。方法: 回顾性分析2015年7月至2019年12月在安徽医科大学第一附属医院确诊为过敏性紫癜肾炎的485例儿童的临床资料。根据出院诊断是否合并链球菌感染分为两组, 合并链球菌感染组(实验组)91例患儿, 对照组394例患儿。通过人工神经网络初步挑选合适的测试项目, 再采用SPSS 23.0统计软件进行数据分析。结果: 两组患儿在尿蛋白、肝肾功能、免疫球蛋白和补体的检测项目上的差异均有统计学意义, 其中抗链球菌溶血素O与IgG(Spearman r=-0.328)、纤维蛋白降解产物(Spearman r=-0.207)、总蛋白(Spearman r=-0.202)和球蛋白(Spearman r=-0.223)均呈轻度相关性。两组患儿在平均年龄(P=0.001)、IgG(P<0.001)、纤维蛋白降解产物(P=0.019)、血清总蛋白(P<0.001)、球蛋白(P<0.001)、IgA(P<0.001)、IgM(P=0.003)、补体C3(P=0.016)、补体C4(P=0.002)、白蛋白/球蛋白比例(P=0.007)、血清碱性磷酸酶(P=0.036)和估计肾小球滤过率(estimated glomerular filtration rate, eGFR, P=0.039)的平均水平上差异均有统计学意义。为研究过敏性紫癜肾炎患儿肾损伤的危险因素, 将抗链球菌溶血素O、年龄、免疫球蛋白和补体作为自变量, 尿蛋白检测参数和肝肾功能作为因变量做Logistic回归分析, 年龄≤10岁和低补体血症可能是过敏性紫癜肾炎患儿加重肾损害的危险因素。结论: 链球菌感染可能会加重过敏性紫癜肾炎患儿的肾损害, 其中低补体血症、炎症、纤维蛋白溶解和凝血异常可能起重要作用。合并链球菌感染的患儿临床上应及时进行抗感染治疗, 出院后应定期随访。
中图分类号:
- R726.9
| 1 |
Hetland LE , Susrud KS , Lindahl KH , et al. Henoch-Schönlein purpura: A literature review[J]. Acta Derm Venereol, 2017, 97 (10): 1160- 1166.
doi: 10.2340/00015555-2733 |
| 2 |
Aalberse J , Dolman K , Ramnath G , et al. Henoch-Schönlein purpura in children: An epidemiological study among Dutch paediatricians on incidence and diagnostic criteria[J]. Ann Rheum Dis, 2007, 66 (12): 1648- 1650.
doi: 10.1136/ard.2006.069187 |
| 3 |
Arslansoyu Çamlar S , Soylu A , Akil I· , et al. Henoch-Schönlein purpura, post-streptococcal glomerulonephritis and acute rheumatic carditis after group A β-haemolytic streptococcal infection[J]. Paediatr Int Child Health, 2018, 38 (1): 73- 75.
doi: 10.1080/20469047.2017.1284394 |
| 4 |
al-Sheyyab M , Batieha A , el-Shanti H , et al. Henoch-Schönlein purpura and streptococcal infection: A prospective case-control study[J]. Ann Trop Paediatr, 1999, 19 (3): 253- 255.
doi: 10.1080/02724939992329 |
| 5 | Chan H , Tang YL , Lv XH , et al. Risk factors associated with renal involvement in childhood Henoch-Schönlein purpura: A meta-analysis[J]. PLoS One, 2016, 11 (11): 1- 21. |
| 6 | 曹芳, 邓芳, 董扬, 等. 血清胱抑素C水平在儿童过敏性紫癜肾损害评价中的意义[J]. 安徽医科大学学报, 2014, 49 (10): 1517- 1520. |
| 7 | 寻劢, 李志辉, 段翠蓉, 等. 五种常见病原体感染与紫癜性肾炎患儿肾小管-间质损伤的相关性研究[J]. 中国中西医结合肾病杂志, 2014, 15 (3): 216- 218. |
| 8 |
Szeto CC , Choi PC , To KF , et al. Grading of acute and chronic renal lesions in Henoch-Schönlein purpura[J]. Mod Pathol, 2001, 14 (7): 635- 640.
doi: 10.1038/modpathol.3880364 |
| 9 | Kawasaki Y , Suzuki J , Sakai N , et al. Clinical and pathological features of children with Henoch-Schönlein purpura nephritis: Risk factors associated with poor prognosis[J]. Clin Nephrol, 2003, 60 (3): 153- 160. |
| 10 | Renganathan V . Overview of artificial neural network models in the biomedical domain[J]. Bratisl Lek Listy, 2019, 120 (7): 536- 540. |
| 11 |
Koskela M , Ylinen E , Autio-Harmainen H , et al. Prediction of renal outcome in Henoch-Schönlein nephritis based on biopsy findings[J]. Pediatr Nephrol, 2020, 35 (4): 659- 668.
doi: 10.1007/s00467-019-04415-3 |
| 12 | 彭启迪, 袁丽萍, 邓芳, 等. 酸敏感离子通道在过敏性紫癜肾炎和IgA肾病肾组织中的表达及意义[J]. 安徽医科大学学报, 2016, 51 (4): 578- 582. |
| 13 | 李文安, 刘凯, 江帆, 等. 急性失代偿性心力衰竭患者血清碱性磷酸酶与肾功能恶化的相关性研究[J]. 中国全科医学, 2018, 21 (7): 818- 821. |
| 14 | Bérubé MD , Blais N , Lanthier S . Neurologic manifestations of Henoch-Schönlein purpura[J]. Handb Clin Neurol, 2014, 120, 1101- 1111. |
| 15 | 钦云峰, 闵芳梅. 紫癜性肾炎儿童凝血和纤溶系统的变化特点及其临床意义[J]. 中国基层医药, 2019, 26 (23): 2903- 2906. |
| 16 | Shao WX , Ye Q , Wang XJ . Application value of laboratory indexes in the differential diagnosis of Henoch-Schönlein purpura[J]. Z Rheumatol, 2017, 76 (4): 351- 356. |
| 17 | Delbet JD , Hogan J , Aoun B , et al. Clinical outcomes in children with Henoch-Schönlein purpura nephritis without crescents[J]. Pediatr Nephrol, 2017, 32 (7): 1193- 1199. |
| [1] | 赵亚云, 倪梦凡, 李雪, 王蓓, 程功, 何菁, 金月波. 利妥昔单抗治疗原发性干燥综合征肾损害的临床疗效和安全性[J]. 北京大学学报(医学版), 2025, 57(6): 1051-1060. |
| [2] | 李宗瀚, 黄洋阅, 李宁, 李明磊, 宋宏程, 张潍平, 刘超. 国产单孔蛇形臂机器人手术系统在儿童肾盂成形术中的应用[J]. 北京大学学报(医学版), 2025, 57(4): 662-665. |
| [3] | 赵兆, 张维宇, 杨文博, 张勇杰, 张晓鹏, 赵慧颖, 周刚, 王强. 低龄、低体重儿童肾移植2例[J]. 北京大学学报(医学版), 2025, 57(4): 803-807. |
| [4] | 张依航, 蔡珊, 陈子玥, 刘云飞, 党佳佳, 师嫡, 李佳欣, 黄天彧, 宋逸. 基于RE-AIM框架儿童青少年近视与肥胖共病综合干预实施性研究结局指标的构建[J]. 北京大学学报(医学版), 2025, 57(3): 436-441. |
| [5] | 唐孟利, 刘扬, 秦冉, 郭欣, 李宏田. 我国10省幼儿园5~6岁儿童近视和近视前期流行特征[J]. 北京大学学报(医学版), 2025, 57(3): 442-447. |
| [6] | 刘光旭, 张良, 赵厚宇, 邓思危, 杨君婷, 李宁, 马瑞, 何艳, 许国章, 刘志科, 詹思延. 2015—2021年宁波市6岁以下儿童热性惊厥的流行病学特征[J]. 北京大学学报(医学版), 2025, 57(3): 584-591. |
| [7] | 李琳, 廖津津. 应用ROC曲线评估久坐行为对儿童青少年视力不良的预测价值[J]. 北京大学学报(医学版), 2025, 57(3): 614-619. |
| [8] | 邓敏婷, 王楠, 夏斌, 赵玉鸣, 朱俊霞. 儿童及青少年挫入恒前牙自行再萌出的相关影响因素[J]. 北京大学学报(医学版), 2025, 57(1): 148-153. |
| [9] | 杨颖婷, 李若竹, 窦桂丽, 雷玥, 夏斌. iRoot BP Plus用于年轻恒牙外伤部分牙髓切断治疗的临床随机对照研究[J]. 北京大学学报(医学版), 2024, 56(6): 1083-1088. |
| [10] | 赵双云, 邹思雨, 李雪莹, 沈丽娟, 周虹. 中文版口腔健康素养量表简版(HeLD-14)在学龄前儿童家长中应用的信度和效度评价[J]. 北京大学学报(医学版), 2024, 56(5): 828-832. |
| [11] | 陈心心, 唐哲, 乔艳春, 荣文笙. 北京市密云区4岁儿童患龋状况及其与龋活跃性检测的相关性[J]. 北京大学学报(医学版), 2024, 56(5): 833-838. |
| [12] | 岳芷涵,韩娜,鲍筝,吕瑾莨,周天一,计岳龙,王辉,刘珏,王海俊. 儿童早期体重指数轨迹与超重风险关联的前瞻性队列研究[J]. 北京大学学报(医学版), 2024, 56(3): 390-396. |
| [13] | 费秀文,刘斯,汪波,董爱梅. 成人及儿童组织坏死性淋巴结炎临床特征及治疗[J]. 北京大学学报(医学版), 2024, 56(3): 533-540. |
| [14] | 俞光岩. 儿童唾液腺疾病[J]. 北京大学学报(医学版), 2024, 56(1): 1-3. |
| [15] | 闫晓晋,刘云飞,马宁,党佳佳,张京舒,钟盼亮,胡佩瑾,宋逸,马军. 《中国儿童发展纲要(2011-2020年)》实施期间中小学生营养不良率变化及其政策效应分析[J]. 北京大学学报(医学版), 2023, 55(4): 593-599. |
|
||
