北京大学学报(医学版) ›› 2026, Vol. 58 ›› Issue (2): 359-364. doi: 10.19723/j.issn.1671-167X.2026.02.021
超显微淋巴管-静脉吻合术治疗肢体淋巴水肿: 基于临床分期与吲哚菁绿分型的疗效分析
武竞衡1,*( ), 薛云皓1, 陈山林1, 郭银涛2, 刘云涛2, 张维2
), 薛云皓1, 陈山林1, 郭银涛2, 刘云涛2, 张维2
- 1. 首都医科大学附属北京积水潭医院手外科, 北京 100035
2. 郑州大学附属郑州中心医院手显微外科, 郑州 450007
Super microsurgical lymphaticovenular anastomosis for limb lymphedema: An outcome analysis based on clinical stage and indocyanine green pattern
Jingheng WU1,*(), Yunhao XUE1, Shanlin CHEN1, Yintao GUO2, Yuntao LIU2, Wei ZHANG2
- 1. Department of Hand Surgery, Beijing Jishuitan Hospital, Capital Medical University, Beijing 100035, China
2. Department of Hand and Microsurgery, Zhengzhou Central Hospital Affiliated to Zhengzhou University, Zhengzhou 450007, China
摘要:
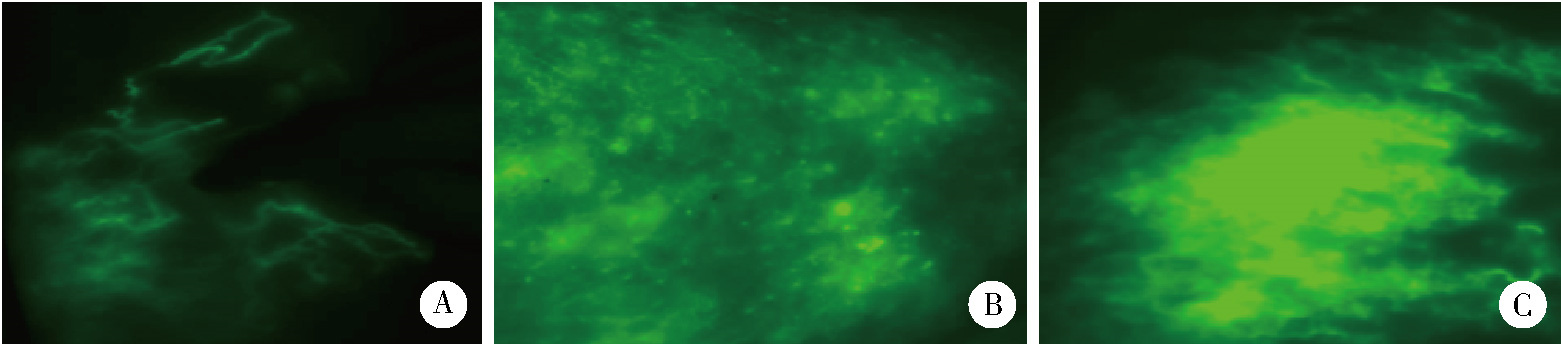
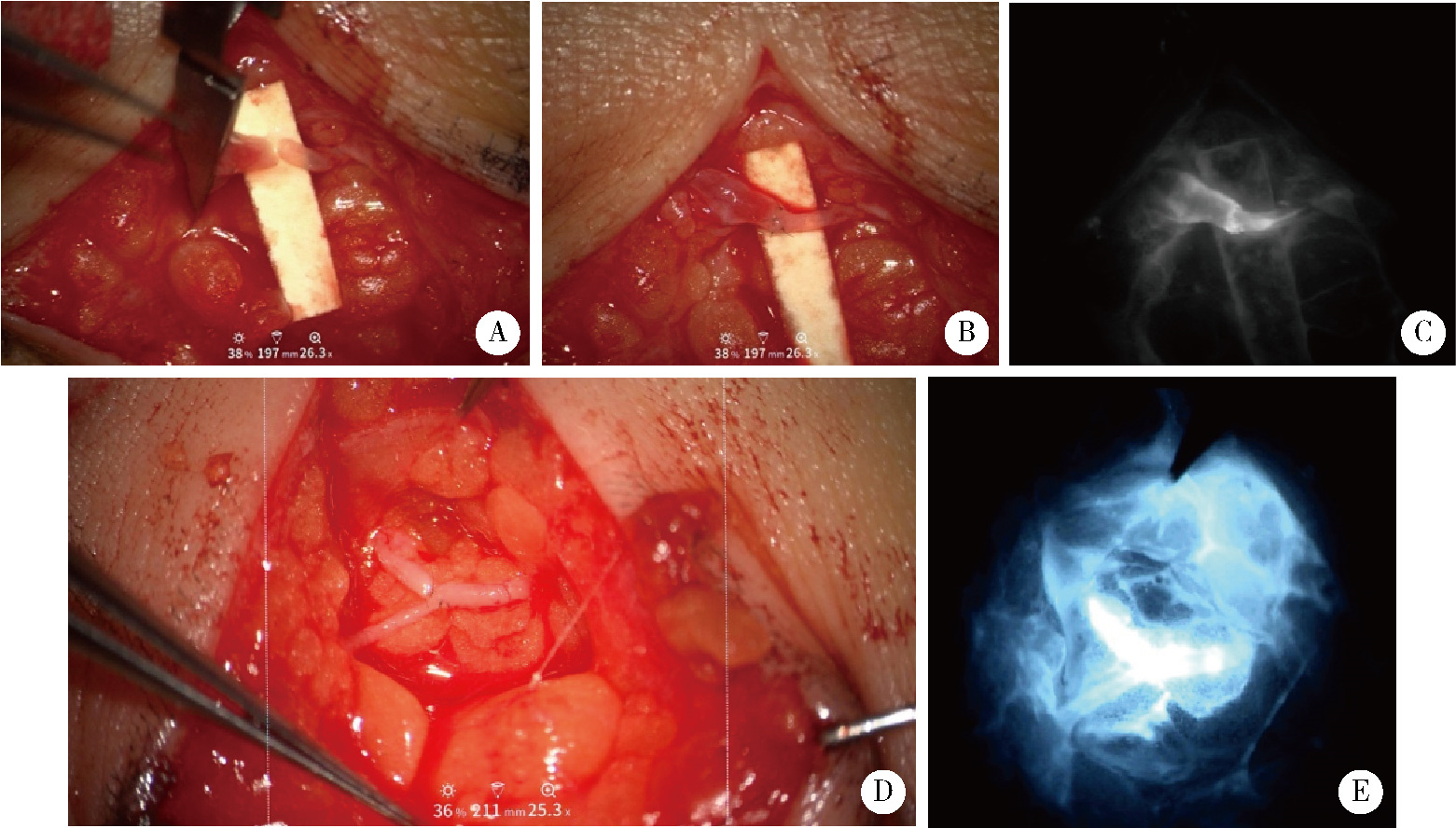
目的: 依据国际淋巴学会(International Society of Lymphology, ISL)分期及吲哚菁绿(indocyanine green, ICG)淋巴造影Yamamoto标准分型,探讨超显微淋巴管-静脉吻合术(lymphaticovenular anastomosis, LVA)治疗肢体淋巴水肿的疗效差异,为手术适应证选择提供循证依据。方法: 回顾性分析2023年12月至2025年4月收治的32例单侧肢体淋巴水肿患者。术前按ISL标准分为Ⅰ~Ⅱ期(30例)和Ⅲ期(2例);按照ICG造影Yamamoto标准分型分为飞溅型(6例)、星尘型(14例)、弥漫型(12例)。术后6个月肢体体积减少率(percentage reduction of limb volume, %REV)和肢体周径减少情况作为主要观察指标,吻合口通畅率、蜂窝织炎复发率、压力袜降级率、患者满意度作为次要观察指标。采用单因素方差分析和Bonferroni校正比较ISLⅠ~Ⅱ期与ICG不同分型间的% REV;效应量用Cohen’ s d值;用多元线性回归分析% REV的独立影响因素。结果: (1) ISL分期疗效:Ⅰ~Ⅱ期患者整体%REV为53%±9%,其中Ⅰ期为63%±8%,Ⅱ期为50%±7%,Ⅲ期% REV为36%±5%(描述性结果);(2) ICG分型疗效:飞溅型%REV为63%±6%,星尘型%REV为56%±7%,弥漫型%REV为36%±4%,差异具有统计学意义(P < 0.001,d=3.5);(3) 弥漫型与ISL Ⅲ期存在临床观察到的疗效衰减趋势;吻合口1年通畅率92.2%,蜂窝织炎复发率由28.1%降至0.0%(P=0.01);26例(81.3%)有压力袜降级,满意度96.9%。结论: LVA疗效与ISL分期及ICG分型密切相关;ICG飞溅型/ISL Ⅱ期及以内患者% REV可>55%,应作为LVA治疗的首选适应证;ICG弥漫型/ISLⅢ期患者需联合脂肪抽吸或血管化淋巴结移植等辅助治疗以优化疗效;术前ICG淋巴造影联合ISL分期评估,可为LVA手术适应证的选择及治疗方案的制定提供可靠依据。
中图分类号:
- R622.4




| 1 |
Cheville AL, McLaughlin SA, Glaser GE, et al. Cancer related lymphedema[J/OL]. BMJ, 2025, 390(2025-07-03)[2025-09-10]. https://pubmed.ncbi.nlm.nih.gov/41065270.
|
| 2 |
doi: 10.1002/micr.22115 |
| 3 |
doi: 10.1097/PRS.0000000000009247 |
| 4 |
doi: 10.1055/a-2530-5875 |
| 5 |
doi: 10.1007/s12032-024-02421-6 |
| 6 |
doi: 10.1080/17434440.2024.2419476 |
| 7 |
doi: 10.1055/s-2003-40575 |
| 8 |
doi: 10.1002/micr.1025 |
| 9 |
doi: 10.1016/j.bjps.2012.05.026 |
| 10 |
doi: 10.1055/s-0032-1311691 |
| 11 |
doi: 10.1097/01.sap.0000120319.89926.07 |
| 12 |
doi: 10.1097/PRS.0b013e3182268da8 |
| 13 |
doi: 10.1097/PRS.0b013e31820cf5c6 |
| 14 |
doi: 10.1002/micr.20980 |
| 15 |
doi: 10.1002/bjs.9588 |
| [1] | 钟剑球,曾沛英,王庆文. 类风湿关节炎合并淋巴水肿2例及文献回顾[J]. 北京大学学报(医学版), 2020, 52(6): 1157-1161. |
|
||
