北京大学学报(医学版) ›› 2026, Vol. 58 ›› Issue (3): 446-454. doi: 10.19723/j.issn.1671-167X.2026.03.002
基于层次-K均值混合聚类法的中国人乳头瘤病毒疫苗双边国际合作优先程度评估
吴音格, 黄旸木*( )
)
- 北京大学公共卫生学院全球卫生学系, 北京 100191
Evaluation of bilateral vaccine cooperation priority countries on Chinese human papillomavirus vaccine using hierarchical K-means hybrid clustering
Yinge WU, Yangmu HUANG*()
- Department of Global Health, Peking University School of Public Health, Beijing 100191, China
摘要:
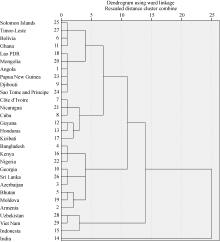
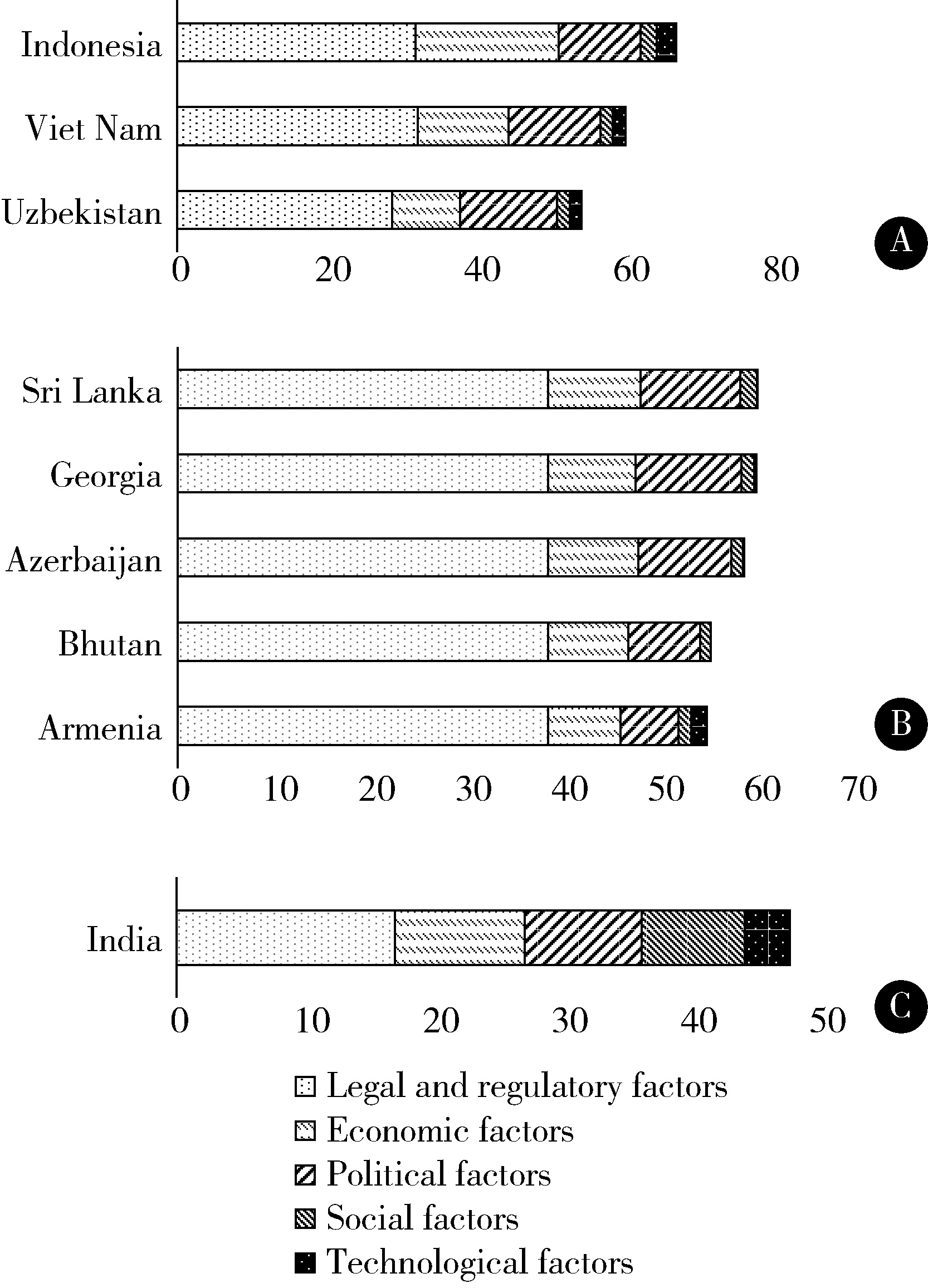
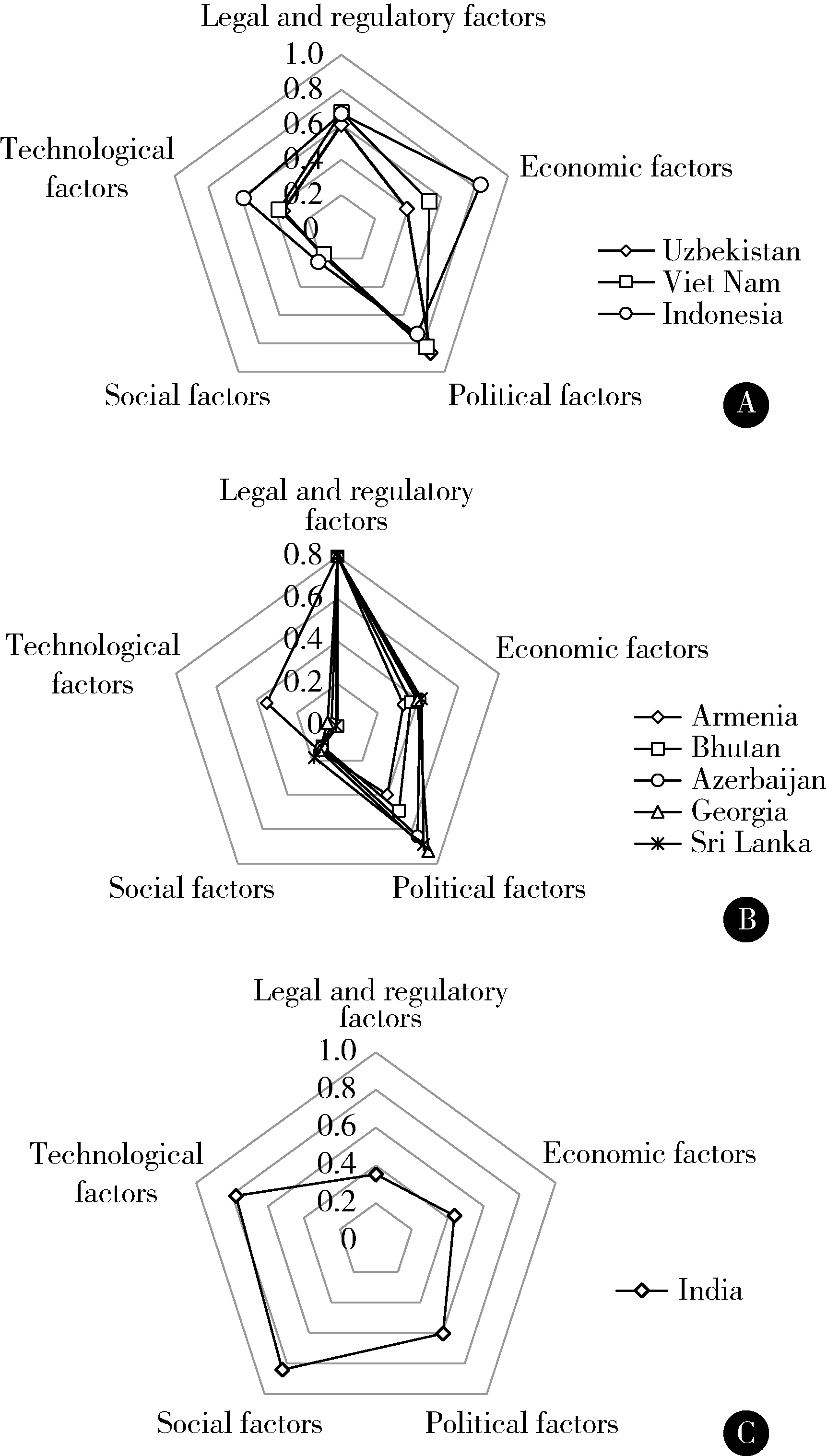
目的: 评估中国人乳头瘤病毒(human papillomavirus,HPV)疫苗双边国际合作中的优先国家及对应的合作方式,为优化中国的HPV疫苗合作策略提供参考与借鉴。方法: 借助已建立完成的中国国际疫苗合作优先国家筛选指标体系,使用加权评分法对处于全球疫苗免疫联盟第三、第四援助阶段29个国家的HPV疫苗合作优先程度进行评分和排序。基于一级指标得分情况运用层次聚类和K均值聚类结合的层次-K均值混合聚类法进行分析。结果: 评分排序中,排名前10的国家大多为亚洲国家,非洲国家排名较靠后。29个国家在HPV疫苗合作中可分为3个类别:技术转移优先型、基础援助型、高壁垒潜力型。技术转移优先型国家有3个,为印度尼西亚、越南和乌兹别克斯坦,该类别在经济、科技和政治因素上得分较高,有良好的支付能力和疫苗进口规模,具有一定的疫苗研发、生产能力,政治稳定性较强,推荐优先开展合作;基础援助型国家有25个,各因素得分接近平均水平,多为人口较少或低收入国家,适合通过援助和优惠采购开展合作;高壁垒潜力型国家有1个,为印度,其在社会因素和科技因素上得分较高,但法律及规章因素得分极低,提示HPV疫苗需求量大,具有成规模的疫苗产业基础,疫苗产品注册壁垒高,开展合作难度大。建议与印度尼西亚开展优惠价格成品出口、疫苗临床试验方面的合作,同时探索授权生产、技术转移的合作;与越南开展疫苗临床试验的合作;与乌兹别克斯坦开展授权生产、技术转移方面的合作。结论: 中国开展HPV疫苗双边国际合作的优先国家为印度尼西亚、越南和乌兹别克斯坦这类技术转移优先型国家,应以涵盖成品出口、临床试验、授权生产与技术转移的方式与其开展合作。
中图分类号:
- R186

| 1 |
doi: 10.1016/S2214-109X(19)30488-7 |
| 2 |
World Health Organization. Global strategy to accelerate the elimination of cervical cancer as a public health problem[R]. Geneva: World Health Organization, 2020.
|
| 3 |
doi: 10.1016/j.eclinm.2021.100836 |
| 4 |
doi: 10.1016/j.vaccine.2018.06.012 |
| 5 |
doi: 10.1016/j.vaccine.2021.01.036 |
| 6 |
|
| 7 |
doi: 10.1016/S1473-3099(23)00275-X |
| 8 |
doi: 10.1016/j.vaccine.2023.10.041 |
| 9 |
Bown CP, Snyder CM, Staiger RW. Vaccine supply chain resilience and international cooperation[R]. Hanover: Dartmouth College Economics Department, 2022.
|
| 10 |
doi: 10.1111/aspp.12643 |
| 11 |
doi: 10.1371/journal.pgph.0000036 |
| 12 |
吴音格, 崔宇煊, 黄旸木. 中国国际疫苗合作优先国家筛选指标体系构建研究[J]. 中国卫生政策研究, 2024, 17 (9): 60- 67.
|
| 13 |
王谋, 康文梅, 张莹. 应对气候变化南南合作优先合作国家选择方法探讨[J]. 气候变化研究进展, 2021, 17 (6): 744- 751.
|
| 14 |
王怀豫, 肖尧, 李奕辰, 等. "一带一路"建设背景下中国与东盟国家农业科技合作的选择机制[J]. 科技管理研究, 2022, 42 (16): 35- 44.
|
| 15 |
|
| 16 |
Chen TS, Tsai TH, Chen YT, et al. A combined K-means and hierarchical clustering method for improving the clustering efficiency of microarray[C]//2005 International Symposium on Intelligent Signal Processing and Communication Systems. Piscataway, USA: IEEE, 2006: 405-408.
|
| 17 |
Gavi. Eligibility & Co-financing policies[EB/OL]. (2025-06-18)[2025-09-15]. https://www.gavi.org/programmes-impact/programmatic-policies/eligibility-co-financing-policies.
|
| 18 |
李文超, 周勇, 夏士雄. 一种新的基于层次和K-means方法的聚类算法[C]//第二十六届中国控制会议论文集. 张家界: 中国自动化学会控制理论专业委员会, 2007: 2331-2335.
|
| 19 |
胡伟. 改进的层次K均值聚类算法[J]. 计算机工程与应用, 2013, 49 (2): 157- 159.
|
| 20 |
World Health Organization. IA2030 Global Report 2024[EB/OL]. (2025-04-26)[2025-09-15]. https://www.immunizationagenda2030.org/images/documents/Immunization_Agenda_2030_Global_Progress_Report_2024_final.pdf.
|
| 21 |
|
| 22 |
doi: 10.1016/j.pvr.2017.09.001 |
| 23 |
Kurniawati E, Madu L. Indonesia' s efforts to overcome COVID-19 pandemic through international cooperation[C]//Proceedings of the RSF conference series: Business, management and social sciences. Bandung, Indonesia: Research Synergy Foundation, 2021: 242-246.
|
| 24 |
|
| 25 |
MSD in Indonesia. MSD and Bio Farma sign a framework agreement for technology transfer partnership to locally manufacture human papillomavirus (HPV) vaccine in Indonesia[EB/OL]. (2022-12-13)[2025-09-15]. https://www.msd-indonesia.com/news/msd-and-bio-farma-sign-a-framework-agreement-for-technology-transfer-partnership-to-locally-manufacture-human-papillomavirus-hpv-vaccine-in-indonesia/#:~:text=JAKARTA%2C%20INDONESIA%2C%20December%2013th,of%20HPV%20vaccine%20in%20Indonesia.
|
| 26 |
doi: 10.31557/APJCP.2025.26.2.421 |
| 27 |
doi: 10.1016/S1473-3099(20)30860-4 |
| 28 |
doi: 10.3390/ijerph17093144 |
| 29 |
World Health Organization. WHO adds an HPV vaccine for single-dose use[EB/OL]. (2024-10-04)[2025-09-15]. https://www.who.int/news/item/04-10-2024-who-adds-an-hpv-vaccine-for-single-dose-use.
|
| 30 |
Gavi. Detailed product profiles[EB/OL]. (2025-07-13)[2025-09-15]. https://www.gavi.org/news/document-library/detailed-product-profiles.
|
| 31 |
|
| 32 |
doi: 10.1080/21645515.2020.1740559 |
| 33 |
|
| 34 |
|
| 35 |
|
| 36 |
UNICEF. Gavi Shipments 2025 Plan-Vaccines & Devices-All Regions[EB/OL]. (2025-08-28)[2025-09-15]. https://www.unicef.org/supply/media/24271/file/Gavi-shipments-Aug-2025.pdf.
|
| [1] | 林文灏, 谢阳, 王芳晴, 王淑盈, 刘香君, 胡凡磊, 贾园. 基于B细胞单细胞转录组测序的干燥综合征分子分型[J]. 北京大学学报(医学版), 2025, 57(6): 1032-1041. |
| [2] | 陈龙, 任明辉. 《国际卫生条例(2005)》修正案在中国适用的挑战及展望[J]. 北京大学学报(医学版), 2025, 57(3): 411-416. |
| [3] | 蔡文心,李仕成,刘一鸣,梁如玉,李静,郭建萍,胡凡磊,孙晓麟,李春,刘栩,叶华,邓立宗,李茹,栗占国. 类风湿关节炎临床分层及其特征的横断面研究[J]. 北京大学学报(医学版), 2022, 54(6): 1068-1073. |
| [4] | 那宾*, 许天民, 林久祥. Procrusts重叠以及多元统计应用于安氏Ⅱ类错牙合颅面分类的研究[J]. 北京大学学报(医学版), 2009, 41(1): 71-75. |
| [5] | 韩冰, 许天民, 林久祥. 普通坐标和procrusts重叠标准化坐标对安氏Ⅰ类错(牙合)进行聚类和判别分析的对比研究[J]. 北京大学学报(医学版), 2007, 39(1): 54-59. |
|
||
