北京大学学报(医学版) ›› 2026, Vol. 58 ›› Issue (3): 455-463. doi: 10.19723/j.issn.1671-167X.2026.03.003
基于中国家庭追踪调查的居民主观认知、收入变化与就医点选择转移的关联
许春春1, 简伟研1,2,*( )
)
- 1. 北京大学公共卫生学院卫生政策与管理学系, 北京 100191
2. 国家卫生健康委员会卫生体系改革与治理研究重点实验室, 北京 100191
Associations of subjective perceptions and income change with transitions in usual source of care among Chinese residents: A study based on China Family Panel Studies
Chunchun XU1, Weiyan JIAN1,2,*()
- 1. Department of Health Policy and Management, Peking University School of Public Health, Beijing 100191, China
2. Key Laboratory of Health System Reform and Governance, National Health Commission, Beijing 100191, China
摘要:
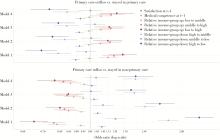
目的: 基于中国家庭追踪调查(China Family Panel Studies,CFPS)数据,描述中国成年人通常就医点结构变化和主观认知变化,并分析主观认知和收入变化与就医点选择转移的关联。方法: 本研究为回顾性纵向观察研究,使用CFPS 2012、2014、2016、2018、2020、2022年六轮调查的成年人数据。先描述3类通常就医点(基层、医院、诊所)构成的时间趋势,以及居民对医疗机构主观认知与居民相对收入变化的时间趋势;再构建相邻两轮调查人-期样本,在“基线为基层”和“基线为非基层”两组中分别分析基层流出与流入。核心解释变量为上一轮调查满意度、医疗水平评价及相对收入变化情况;其中收入变化变量根据同一轮调查的同一省份样本内相对收入组的变化构造。描述分析采用横截面权重;主回归为未加权二分类Logistic模型,并按个体进行聚类稳健标准误估计,报告优势比(odds ratio, OR)、95%置信区间(confidence interval, CI)和P值。结果: 六轮调查数据合并后共纳入135 986条记录、34 010名个体。2012—2022年通常选择基层医疗机构就医的居民占比由43.49%降至30.34%,医院占比由34.06%升至46.81%;其中基层占比在2012—2018年下降更快(43.49%降至33.72%),2018年后继续下降但降幅趋缓(33.72%降至30.34%)。在相邻两轮调查中,基层流出比例由35.47%升至45.22%,基层流入比例由30.09%降至19.60%,基层就医流出增加和流入减少并行。2012—2022年,居民对基层、医院、诊所三类机构主观认知持续提升,但基层与医院的相对差距在医疗水平方面有所扩大,基层相对诊所的主观认知从微弱领先转为明显落后。相对收入不变的居民占比由50.64%升至60.33%。多因素回归显示,对基层医疗服务的满意度每提高1分,基层流出的优势比下降7.5%(OR=0.925,P < 0.001);对非基层医疗机构医疗水平的评价每提高1分,基层流入的优势比下降5.3%(OR=0.947,P < 0.001)。与相对收入组不变者相比,相对收入组上移者,特别是从低收入组升至高收入组者,表现为更高的基层流出优势比和更低的基层流入优势比(流出OR=1.166;流入OR=0.840);相对收入组下移者,特别是从高收入组降至低收入组者,则表现为更低的基层流出优势比和更高的基层流入优势比(流出OR=0.785;流入OR=1.371)。结论: 我国基层就医利用持续下降,且基层流出增加和基层流入减少同时存在。居民主观认知在基层流出与流入中的关注点并不相同:前者更多与满意度相关,后者更多与医疗水平判断相关。相对收入组上移人群对基层的利用倾向相对较弱。分级诊疗政策应同步关注“导入基层”和“留在基层”,以连续照护体验稳定存量,以能力建设和制度安排吸引增量,并通过支付激励提升基层吸引力。
中图分类号:
- R197.1
| 1 |
中华人民共和国国务院办公厅. 国务院办公厅关于推进分级诊疗制度建设的指导意见[EB/OL]. (2015-09-11)[2026-02-23]. https://www.gov.cn/zhengce/content/2015-09/11/content_10158.htm.
|
| 2 |
doi: 10.1016/S0140-6736(17)33109-4 |
| 3 |
doi: 10.1002/hcs2.14 |
| 4 |
doi: 10.1186/s12913-021-06790-w |
| 5 |
doi: 10.1136/bmjph-2024-001595 |
| 6 |
doi: 10.1186/s12913-021-06908-0 |
| 7 |
陈纯, 张勇, 黄绍中, 等. 2005-2014年福建省直单位参保人群中心脑血管疾病患者门诊就诊机构及费用分布的概况及分析[J]. 中国全科医学, 2017, 20 (24): 3008- 3014.
|
| 8 |
doi: 10.1080/13814788.2024.2308740 |
| 9 |
|
| 10 |
doi: 10.1093/heapro/daae115 |
| 11 |
汪晓露, 黄哲, 钱艳娟, 等. 分级诊疗背景下社区居民全科医疗服务需求与就诊意向机构研究[J]. 中国全科医学, 2021, 24 (7): 805- 811.
|
| 12 |
孙华君, 田慧, 杜汋. 家庭医生签约服务对居民就诊行为的影响: 基于倾向得分匹配的实证研究[J]. 中国全科医学, 2020, 23 (19): 2396- 2400.
|
| 13 |
朱玉琴, 金花, 于德华. 分级诊疗背景下多病共存患者就医机构选择行为及其影响因素研究[J]. 中国全科医学, 2023, 26 (13): 1598- 1604.
|
| 14 |
王沛, 刘军军. 基于安德森模型的多重慢病患者就医机构选择及影响因素研究[J]. 中国全科医学, 2020, 23 (25): 3154- 3159.
|
| 15 |
doi: 10.1016/S0140-6736(19)32136-1 |
| 16 |
doi: 10.1016/S0140-6736(20)30122-7 |
| 17 |
doi: 10.1016/S2468-2667(23)00254-2 |
| 18 |
doi: 10.1136/bmjgh-2020-003570 |
| 19 |
雷祎, 赵焱, 孙静. 医联体模式下北京市海淀区社区居民双向转诊现状及影响因素分析[J]. 中国全科医学, 2019, 22 (25): 3049- 3054.
|
| 20 |
陈聪, 朱海虹. 基于安德森模型的家庭医生签约2型糖尿病患者基层就诊行为影响因素研究[J]. 中国全科医学, 2025, 28 (7): 888- 892.
|
| 21 |
doi: 10.1186/s12875-024-02298-4 |
| 22 |
doi: 10.3389/fpubh.2022.800042 |
| 23 |
doi: 10.1080/13696998.2024.2421115 |
| 24 |
doi: 10.1016/j.socscimed.2023.116148 |
| 25 |
|
| 26 |
doi: 10.1186/s12875-025-02856-4 |
| 27 |
|
| 28 |
卢珊, 李月娥. Anderson医疗卫生服务利用行为模型: 指标体系的解读与操作化[J]. 中国卫生经济, 2018, 37 (9): 5- 10.
|
| 29 |
孔春燕, 赵芳. 分级诊疗视域下基层首诊意愿影响因素的联合实验研究[J]. 中国全科医学, 2026, 29 (7): 851- 857.
|
| 30 |
中共中央办公厅, 国务院办公厅. 中共中央办公厅国务院办公厅印发《关于进一步完善医疗卫生服务体系的意见》[EB/OL]. (2023-03-23)[2026-02-01]. https://www.gov.cn/gongbao/content/2023/content_5750620.htm.
|
| [1] | 冉珂欣,李与涵,冯文. 远程医疗对我国公立医院运营的影响[J]. 北京大学学报(医学版), 2024, 56(3): 471-478. |
| [2] | 李志昌,侯云飞,周之伟,姜龙,张舒,林剑浩. 影响全膝关节置换术患者术前预期的患者因素[J]. 北京大学学报(医学版), 2022, 54(1): 170-176. |
| [3] | 刘向晖, 刘建彰, 谢秋菲, 康艳凤, 陈薇. 长正中牙合型总义齿的咀嚼效率和满意度的初步评价[J]. 北京大学学报(医学版), 2013, 45(1): 50-53. |
| [4] | 王富华, 谢铮, 吕敏, 邓瑛, 张拓红. 北京户籍老人免费流感疫苗接种情况及城乡差异分析[J]. 北京大学学报(医学版), 2013, 45(03): 432-436. |
| [5] | 金哲, 朱一辰, 崔万寿, 刘涛, 李维仁, 袁亦铭, 宋卫东, 辛钟成. 阴茎起勃器植入手术治疗重度勃起功能障碍的效果和患者满意度[J]. 北京大学学报(医学版), 2010, 42(4): 413-417. |
| [6] | 谢铮, 徐玲. 基于计划行动理论的我国农村居民就医行为选择分析[J]. 北京大学学报(医学版), 2010, 42(3): 270-274. |
| [7] | 史宇晖, 陈磊, 房洪军, 孙玮, 常春. 健康教育对农民参加新型农村合作医疗意愿的影响[J]. 北京大学学报(医学版), 2010, 42(3): 275-278. |
| [8] | 潘韶霞, Jocelyne Sheila FEINE, 冯海兰. 对无牙颌患者ACP分类方法临床应用的评价 [J]. 北京大学学报(医学版), 2009, 41(1): 86-89. |
|
||
