北京大学学报(医学版) ›› 2026, Vol. 58 ›› Issue (3): 464-471. doi: 10.19723/j.issn.1671-167X.2026.03.004
不同行政隶属关系公立医院绩效薪酬形成机制的差异
张雨欣1,2, 李与涵1,2, 巴特龙1,2, 蔡知昇1,2, 刘星宇1,2, 冯文1,2,*( )
)
- 1. 北京大学公共卫生学院卫生政策与管理学系, 北京 100191
2. 国家卫生健康委员会卫生体系改革与治理研究重点实验室(北京大学), 北京 100191
Differences in the formation mechanism of performance-based compensation in public hospitals with different administrative affiliations
Yuxin ZHANG1,2, Yuhan LI1,2, Telong BA1,2, Zhisheng CAI1,2, Xingyu LIU1,2, Wen FENG1,2,*()
- 1. Department of Health Policy and Management, Peking University School of Public Health, Beijing 100191, China
2. National Health Commission Key Laboratory of Health System Reform and Governance(Peking University), Beijing 100191, China
摘要:
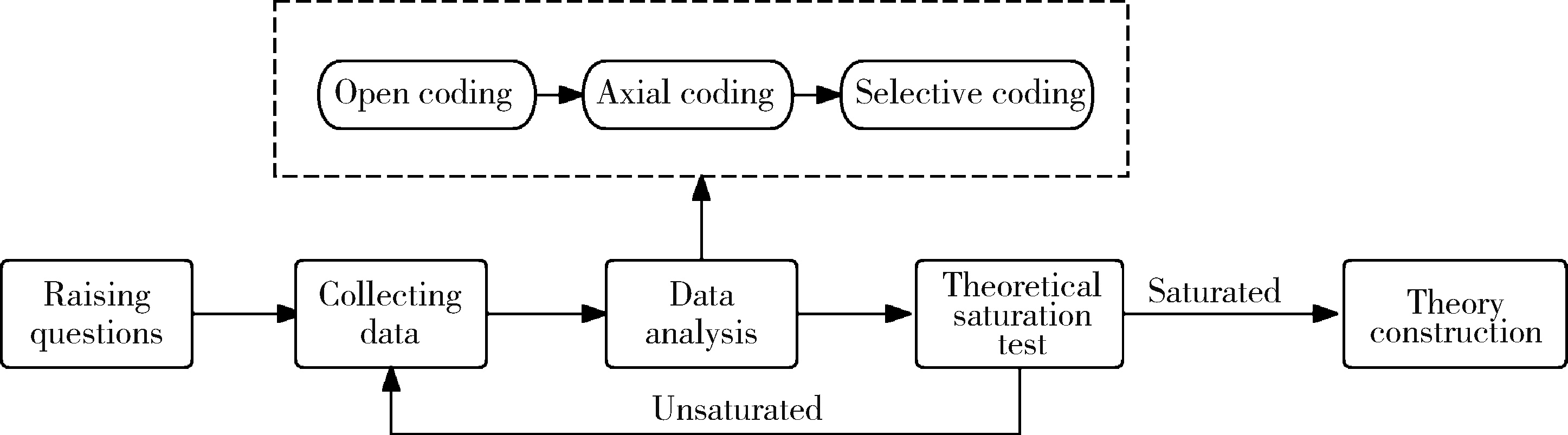
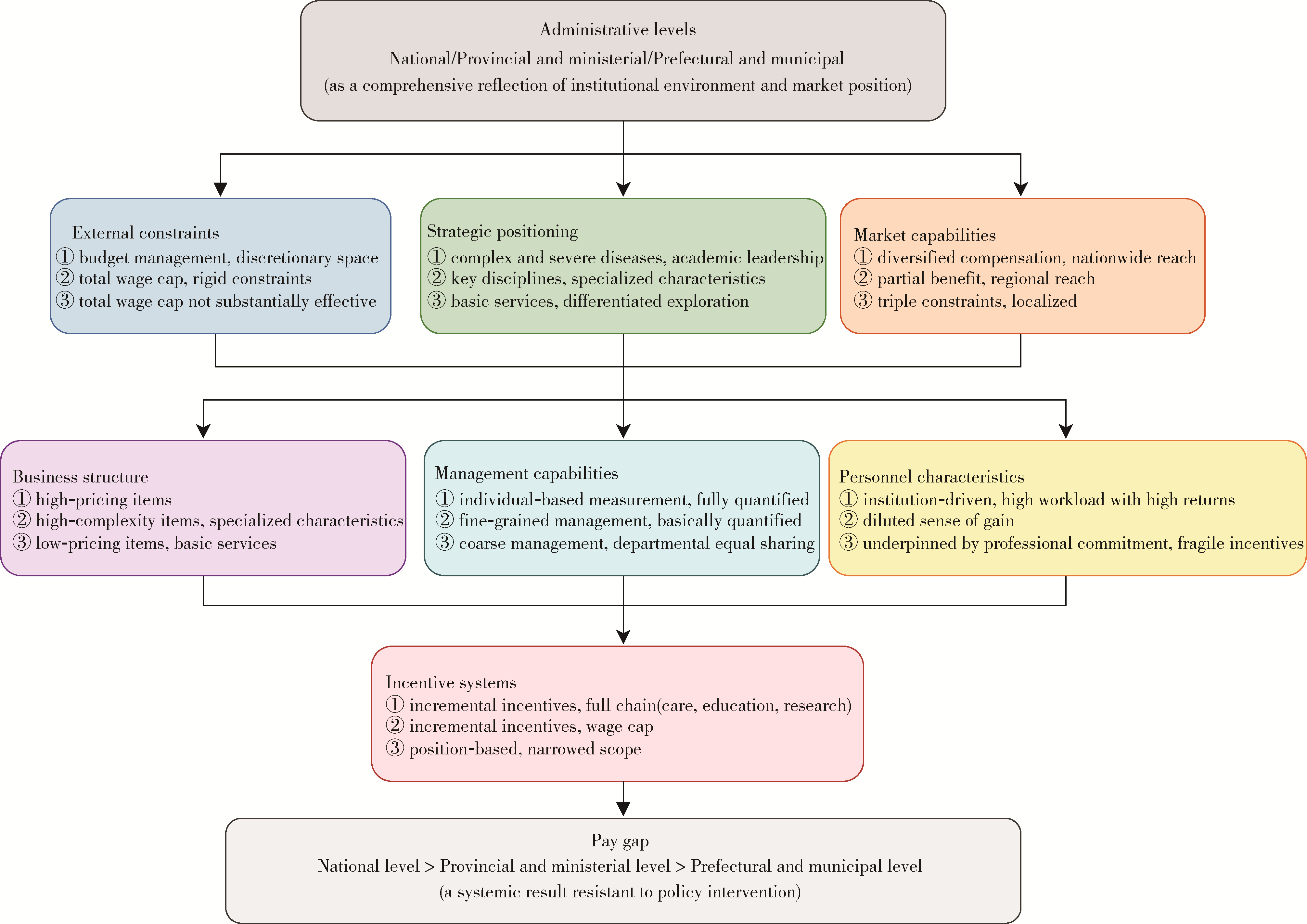
目的: 公立医院薪酬改革的目标之一是缩小公立医院的薪酬差距,本研究从不同行政层级的公立医院出发,探究绩效薪酬形成机制的差异。方法: 2024年6—11月,采用目的性抽样,对某直辖市国家级、省部级、地市级三个行政层级的14家公立医院进行43场深入访谈,采用扎根理论进行分析。结果: 通过三级编码,共提炼出7个核心范畴(外部约束、战略定位、市场能力、业务结构、激励制度、管理能力、人员特征),共同作用于公立医院的绩效薪酬分配,但其在不同层级的医院之间呈现差异。行政层级较高的公立医院或免于工资总额约束,或在总额框架内仍保留较大的可分配空间,依托高位的战略定位,形成了强大的市场能力与高溢价业务结构,采用计量到个人的增量激励模式,激励范畴覆盖医教研全链条;较低层级的公立医院则面临议价能力不足、患者来源局限、补偿途径单一的三重约束,业务结构以低溢价项目为主,不得不采用岗位履职模式,激励范畴收窄至基础质量,面临激励脆弱与人才流失的困境。结论: 不同层级公立医院在绩效薪酬决定机制上呈现结构差异,改革政策在传导过程中遭遇层级化制度环境、市场能力与管理能力的分层过滤,使其在政策下的表现不同。
中图分类号:
- R197.3


| 1 |
张利江, 王克渠, 杨皓宇, 等. 国内公立医院医生薪酬与绩效关联研究[J]. 中国医院, 2025, 29 (12): 77- 82.
|
| 2 |
路畅, 张冬青, 刘欣玥, 等. 高质量发展要求下公立医院绩效薪酬分配方式改革探讨[J]. 中国卫生经济, 2025, 44 (8): 33- 35.
|
| 3 |
高瑞欣. 公立医院临床医师绩效评价体系及应用研究——以河北省Z医院为例[D]. 石家庄: 河北经贸大学, 2015.
|
| 4 |
张志强. 基于ISM的公立医院综合绩效影响因素研究[D]. 南京: 南京中医药大学, 2016.
|
| 5 |
韩静. 临床医师工作绩效现状及其影响因素研究[D]. 遵义: 遵义医学院, 2018.
|
| 6 |
吴毅, 吴刚, 马颂歌. 扎根理论的起源、流派与应用方法述评——基于工作场所学习的案例分析[J]. 远程教育杂志, 2016 (3): 32- 41.
|
| 7 |
陈向明. 扎根理论的思路和方法[J]. 教育研究与实验, 1999 (4): 58- 63.
|
| 8 |
沈春晗, 王珩, 李念念. 安徽省县级公立医院临床医生薪酬满意度状况及其影响因素[J]. 医学与社会, 2021, 34 (9): 106- 110.
|
| 9 |
任英丽. 探析绩效考核在县级公立医院人力资源管理中的应用[J]. 乡镇企业导报, 2024 (11): 197- 199.
|
| 10 |
陈荣荣, 王冉. 县级公立医院人才绩效管理问题研究——以X医院为例[J]. 中国管理信息化, 2024, 27 (23): 133- 136.
|
| 11 |
贾瑶瑶, 刘勇. 我国公立医院薪酬结构现状分析与探讨[J]. 中国医院管理, 2021, 41 (8): 40- 42.
|
| 12 |
黄明会. 重庆: "1234"法推动二级医院高质量发展[J]. 中国卫生, 2022 (1): 76- 77.
|
| 13 |
翁辰宇. 基层政府公共政策效能非正常衰减研究[D]. 杭州: 浙江工商大学, 2013.
|
| 14 |
唐雪. 医疗服务项目价格变动对公立医院薪酬的影响[J]. 销售与管理, 2025 (32): 123- 125.
|
| 15 |
陈云, 王金海. 内蒙古公立医院医务人员绩效薪酬的影响因素研究[J]. 医学与社会, 2023, 36 (1): 123- 128.
|
| 16 |
韩丽平, 叶苹. 公立医院人力资源管理中的绩效管理问题探研——以泰州市人民医院为例[J]. 泰州职业技术学院学报, 2025, 25 (2): 42- 43.
|
| 17 |
何贤慧, 李玲. 县级三级公立医院绩效考核的研究[J]. 中国管理信息化, 2023, 26 (16): 152- 154.
|
| 18 |
吴舒婷, 林孟波, 薛芳沁. 三级医院对口帮扶县级医院的实践探索[J]. 中国医疗管理科学, 2025, 15 (1): 103- 107.
|
| [1] | 冉珂欣,李与涵,冯文. 远程医疗对我国公立医院运营的影响[J]. 北京大学学报(医学版), 2024, 56(3): 471-478. |
| [2] | 景日泽,章湖洋,徐婷婷,张鲁豫,方海. 北京市三级公立医院效率及其影响因素[J]. 北京大学学报(医学版), 2018, 50(3): 408-415. |
|
||
