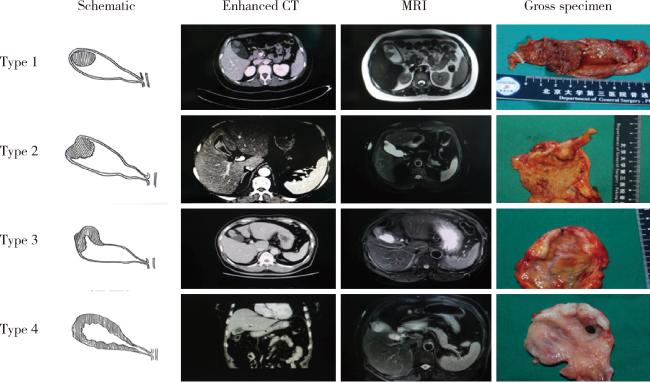
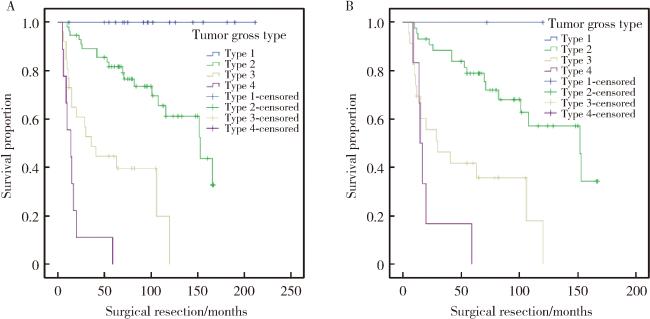
Objective: To explore the gross classification of gallbladder cancer with primary lesion confined within the gallbladder wall, and its correlation with prognosis and precancerous lesions. Methods: A retrospective study was conducted on 123 patients who were admitted to Peking University Third Hospital from January 2006 to December 2020. These patients had preoperative imaging findings suggesting that the primary lesion was confined within the gallbladder wall and had postoperative pathology of adenocarcinoma. Based on CT, MRI, or gross specimens, they were divided into the following four types: Type 1, simple intraluminal lesion: Intraluminal lesions without focal thickening of the gallbladder wall; Type 2, complex intraluminal lesion: Intraluminal lesions associated with focal thickening of the gallbladder wall and/or outer surface dimpling at the tumor base; Type 3, focal wall thickening: Circumferential focal wall thickening with heterogeneous enhancement within 2 continuous parts of the gallbladder; Type 4, diffuse wall thickening: Circumferential diffuse wall thickening extending more than 2 continuous parts of the gallbladder with heterogeneous enhancement. The clinical pathological characteristics, types of precancerous lesions, and survival status were compared among the different types. Results: Both preoperative CT/MRI and intraoperative gross specimens could serve as the basis for gross classification, with gross specimens demonstrating the highest accuracy rate. Among the 123 patients, 13 could not be classified, while the remaining 110 underwent gross classification. The gross classification of gallbladder cancer was strongly or moderately correlated with histopathological parameters such as T-stage (P < 0.001, rs=0.682), lymph node metastasis (P < 0.001, rs=0.478), tissue differentiation degree (P < 0.001, rs=0.484), nerve infiltration (P < 0.001, rs=0.490), and vascular invasion (P < 0.001, rs=0.334). The higher the classification, the more adverse histopathological parameters were observed. Additionally, the gross classification of gallbladder cancer was moderately strongly and highly strongly correlated with residual lesions after surgical treatment (P < 0.001, rs=0.328) and postoperative recurrence (P < 0.001, rs=0.619) in the patients. Survival analysis revealed that the higher the classification, the shorter the median survival time of the patients (Type 1: 96 months, Type 2: 73 months, Type 3: 30 months, Type 4: 14 months, P < 0.001). Multivariate Cox regression indicated that the gross classification of gallbladder cancer was an independent prognostic factor (HR=3.609, 95%CI: 2.177-5.983, P < 0.001). In the patients with the most heterogeneous biological behavior in stage T2, the gross classification of gallbladder cancer was also closely associated with prognosis (median survival times were 72, 70, 29, and 16 months, respectively, P < 0.001). Multivariate Cox regression further demonstrated that the gross classification of gallbladder cancer was an independent prognostic factor (HR=2.723, 95%CI: 1.566-4.736, P < 0.001). In terms of tumor origin, the gross classification of gallbladder cancer was significantly correlated with the type of precancerous lesions: Type 1 mainly originated from intracholecystic papillary neoplasm of the gallbladder, while Types 3 and 4 were mostly high-grade biliary intraepithelial neoplasm or without precancerous lesions. Analysis of the natural history of the tumor suggested that Type 1 progressed slowly, Type 4 progressed rapidly, and Type 2 exhibited greater heterogeneity. Conclusion: The gallbladder cancer with primary lesion confined within the gallbladder wall is closely related to prognosis and precancerous lesions, and can serve as an important reference for surgical decision-making and stratified management.


{kind=link}
{kind=link}
{kind=link}
{kind=link}