
1 资料与方法
1.1 患者一般资料
1.2 干预措施
1.2.1 术前准备
1.2.2 拔牙同期行MCF-ARP

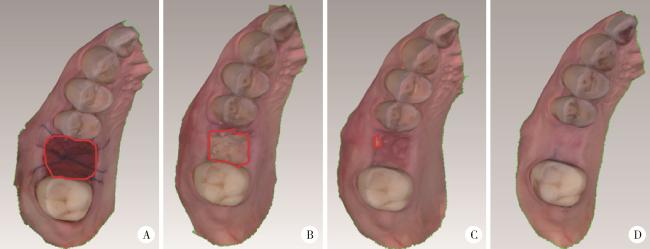
图1 微创拔牙同期分别应用DBBM或HA行MCF-ARP的手术过程Figure 1 The surgical procedure of minimally invasive tooth extraction combined with MCF-ARP using DBBM or HA A1-F1, DBBM group; A2-F2, HA group; A1 and A2, preoperative occlusal view; B1 and B2, minimally invasive tooth extraction, thorough debridement of the socket, and minimal flap reflection to expose the bone surface; C1 and C2, bone graft material placed in the socket, absorbable membrane placed between the gingival flap and the crestal bone; D1 and D2, absorbable membrane covering the bone graft material extending to the apical aspect of the contralateral crestal bone; E1 and E2, absorbable collagen sponge covering the membrane; F1 and F2, coronally repositioned flap, fixed with 4-0 non-absorbable interrupted sutures. MCF-ARP, micro crestal flap-alveolar ridge preservation; DBBM, deproteinized bovine bone mineral; HA, hydroxyapatite. |
1.2.3 随访资料的收集
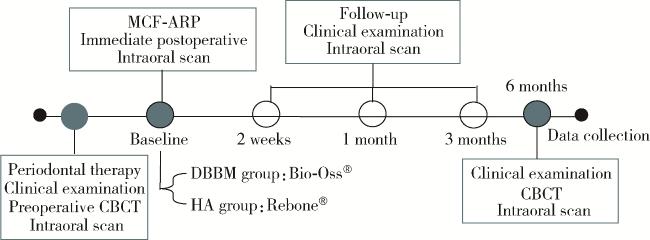
图2 数据收集流程Figure 2 Data collection MCF-ARP, micro crestal flap-alveolar ridge preservation; DBBM, deproteinized bovine bone mineral; HA, hydroxyapatite; CBCT, cone beam computed tomography. |
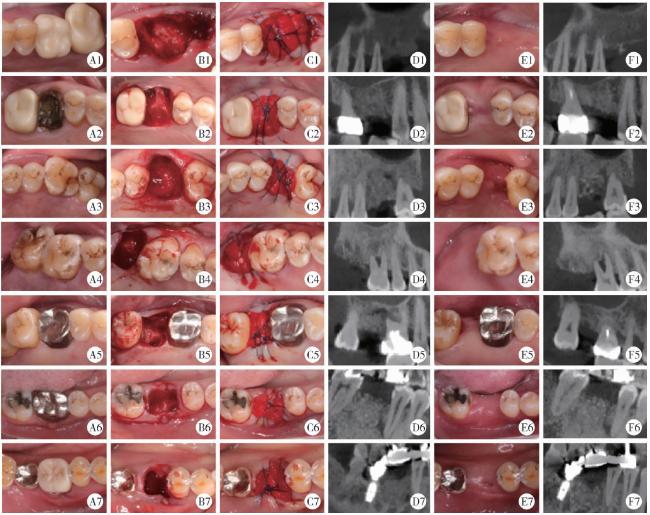
图3 DBBM组患者不同时间点的临床照片与CBCT图像Figure 3 Clinical photographs and CBCT cross-sectional images of DBBM group at different time points A1-A7, preoperative occlusal view; B1-B7, tooth socket; C1-C7, immediate postoperative occlusal view; D1-D7, immediate postoperative CBCT; E1-E7, 6 months follow-up; F1-F7; CBCT taken 6 months postoperative. Abbreviations as in Figure 2. |
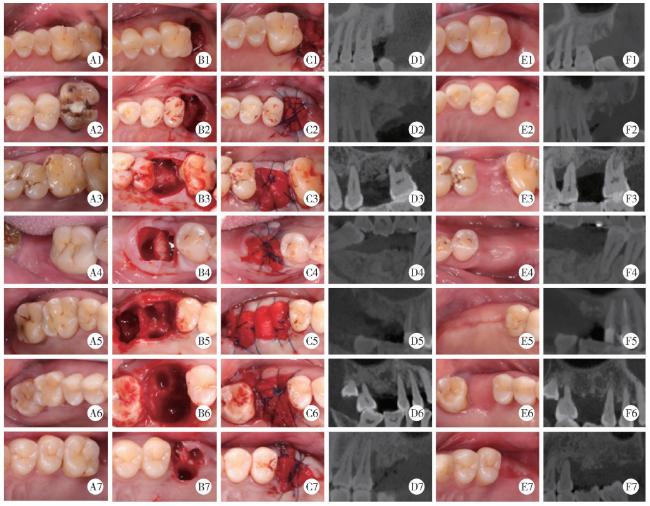
图4 HA组患者不同时间点的临床照片与CBCT图像Figure 4 Clinical photographs and CBCT cross-sectional images of HA group at different time points A1-A7, preoperative occlusal view; B1-B7, tooth socket; C1-C7, immediate postoperative occlusal view; D1-D7, immediate postoperative CBCT; E1-E7, 6 months follow-up; F1-F7; CBCT taken 6 months postoperative. Abbreviations as in Figure 2. |
1.3 测量指标
1.3.1 硬组织变化测量参数
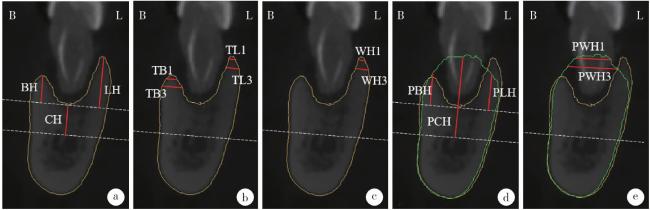
图5 CBCT影像学指标的测量Figure 5 Measurement of CBCT radiographic indicators a, height at the center of the socket (CH), buccal bone height (BH) and lingual/palatal bone height (LH); b, bone wall thicknesses at 1 mm and 3 mm apically below the buccal and lingual/palatal bone crests (TB1, TB3, TL1, TL3); c, ridge widths at 1 mm and 3 mm apically below the higher bone crests (WH1, WH3); d, postoperative height at the center of the socket (PCH), postoperative buccal bone height (PBH) and postoperative lingual/palatal bone height (PLH); e, postoperative ridge widths at 1 mm and 3 mm apically below the higher bone crests (PWH1, PWH3). Yellow curve, baseline alveolar bone contour; Green curve, 6-month postoperative alveolar bone contour. B, buccal; L, lingual; CBCT, cone beam computed tomography. |
1.3.2 牙槽嵴轮廓塌陷量的测量
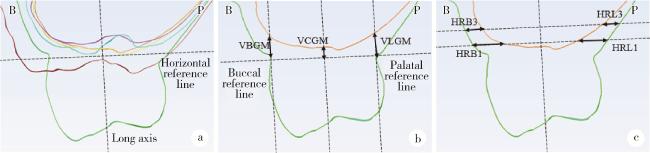
图6 口内扫描牙槽嵴轮廓指标的测量Figure 6 Measurement of alveolar ridge contour parameter by intraoral scanning a, changes in soft tissue contour at follow-up time points; b, vertical reduction of the contour on the buccal free gingival margins (VBGM), vertical reduction of the contour on the lingual/palatal free gingival margins (VLGM) and vertical reduction of the contour on the center of gingival margins (VCGM); c, horizontal reduction of the buccal or lingual/palatal contour at 1 mm, 3 mm apically (HRB1, HRB3, HRL1, HRL3). Green curve, preoperative; Red curve, immediately postoperative; Blue curve, 2 weeks postoperative; Purple curve, 1 month postoperative; Orange curve, 3 months postoperative; Yellow curve, 6 months postoperative. B, buccal; P, palatal. |
1.3.3 软组织愈合过程分析
1.4 统计学分析
2 结果
2.1 纳入患者的基线情况
表1 患者基线资料的比较Table 1 Comparison of patient baseline characteristics |
| Items | DBBM (n=7) | HA (n=7) | t/Z | P |
| Age/years | 52.29±9.90 | 53.86±11.17 | -0.28a | 0.785 |
| Gender | 0.266 | |||
| Female | 4 | 1 | ||
| Male | 3 | 6 | ||
| Tooth position | >0.999 | |||
| Maxillary | 5 | 6 | ||
| Mandibular | 2 | 1 | ||
| BH/mm | 5.32±3.69 | 4.28±4.00 | 0.51a | 0.618 |
| LH/mm | 5.85±3.97 | 4.67±3.74 | 0.57a | 0.577 |
| CH/mm | 5.08±3.53 | 3.65±2.04 | 0.93a | 0.374 |
| TB1/mm | 1.40±1.02 | 1.09±0.89 | 0.61a | 0.555 |
| TB3/mm | 1.64±1.39 | 1.65±1.60 | -0.02a | 0.987 |
| TL1/mm | 1.46±0.40 | 1.58±1.07 | -0.29a | 0.780 |
| TL3/mm | 2.07±0.79 | 2.18±1.99 | -0.13a | 0.897 |
| WH1/mm | 1.83 (1.52, 2.19) | 1.70 (1.31, 8.28) | -0.06b | 0.949 |
| WH3/mm | 6.83 (2.57, 13.26) | 5.67 (1.60, 12.77) | -0.06b | 0.949 |
Data are presented as n, ${\bar x}$±s or M (P25, P75). a, represents t value; b, represents Z value. DBBM, deproteinized bovine bone mineral; HA, hydroxyapatite; BH, buccal bone height; LH, lingual/palatal bone height; CH, height at the center of the socket; TB1, TB3, TL1, TL3, bone wall thicknesses at 1 mm and 3 mm apically below the buccal and lingual/palatal bone crests; WH1, WH3, ridge widths at 1 mm and 3 mm apically below the higher bone crests. |
2.2 硬组织指标的变化
表2 硬组织指标变化的比较Table 2 Comparison of changes in hard tissue parameter |
| Items | DBBM (n=7) | HA (n=7) | t/Z | P |
| PBH/mm | 3.45±4.01 | 6.11±3.38 | -1.34a | 0.204 |
| PLH/mm | 5.85±3.64 | 5.46±2.32 | 0.24a | 0.813 |
| PCH/mm | 13.61±4.07 | 10.43±5.03 | 1.30a | 0.217 |
| DBH/mm | -1.88±1.48 | 1.83±2.36 | -3.53a | 0.004* |
| DLH/mm | 0.00±3.07 | 0.89±3.34 | -0.52a | 0.615 |
| DCH/mm | 8.53±2.56 | 6.77±3.45 | 1.09a | 0.298 |
| PWH1/mm | 8.84±2.66 | 8.66±3.14 | 0.12a | 0.908 |
| PWH3/mm | 10.55±2.65 | 11.37±2.46 | -0.60a | 0.558 |
| DWH1/mm | 7.10 (4.73, 8.94) | 7.22 (-0.54, 9.58) | -0.19b | 0.848 |
| DWH3/mm | 3.13±6.10 | 4.59±5.17 | -0.48a | 0.637 |
Data are presented as ${\bar x}$±s or M (P25, P75). a, represents t value; b, represents Z value. * P < 0.05. DBBM, deproteinized bovine bone mineral; HA, hydroxyapatite; PBH, postoperative buccal bone height; PLH, postoperative lingual/palatal bone height; PCH, postoperative height at the center of the socket; DBH, DLH, DCH, difference between PBH and BH, PLH and LH, PCH and CH; PWH1, PWH3, postoperative ridge widths at 1 mm and 3 mm apically below the higher bone crests; DWH1, DWH3, difference between PWH1 and WH1, PWH3 and WH3. |
2.3 牙槽嵴轮廓塌陷量
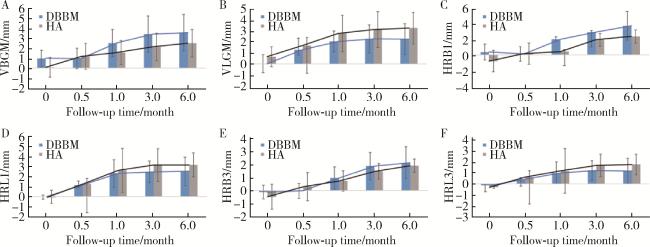
图8 两组患者各随访节点的牙槽嵴轮廓塌陷量Figure 8 Alveolar ridge contour reduction at follow-up time points of the two groups A, vertical reduction of the contour on the buccal free gingival margins (VBGM); B, vertical reduction of the contour on the lingual/palatal free gingival margins (VLGM); C, horizontal reduction of the buccal contour at 1 mm apically (HRB1); D, horizontal reduction of the lingual/palatal contour at 1 mm apically (HRL1); E, horizontal reduction of the buccal contour at 3 mm apically (HRB3); F, horizontal reduction of the lingual/palatal contour at 3 mm apically (HRL3). DBBM, deproteinized bovine bone mineral; HA, hydroxyapatite. |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}