Journal of Peking University (Health Sciences) ›› 2026, Vol. 58 ›› Issue (1): 107-114. doi: 10.19723/j.issn.1671-167X.2026.01.014
Previous Articles Next Articles
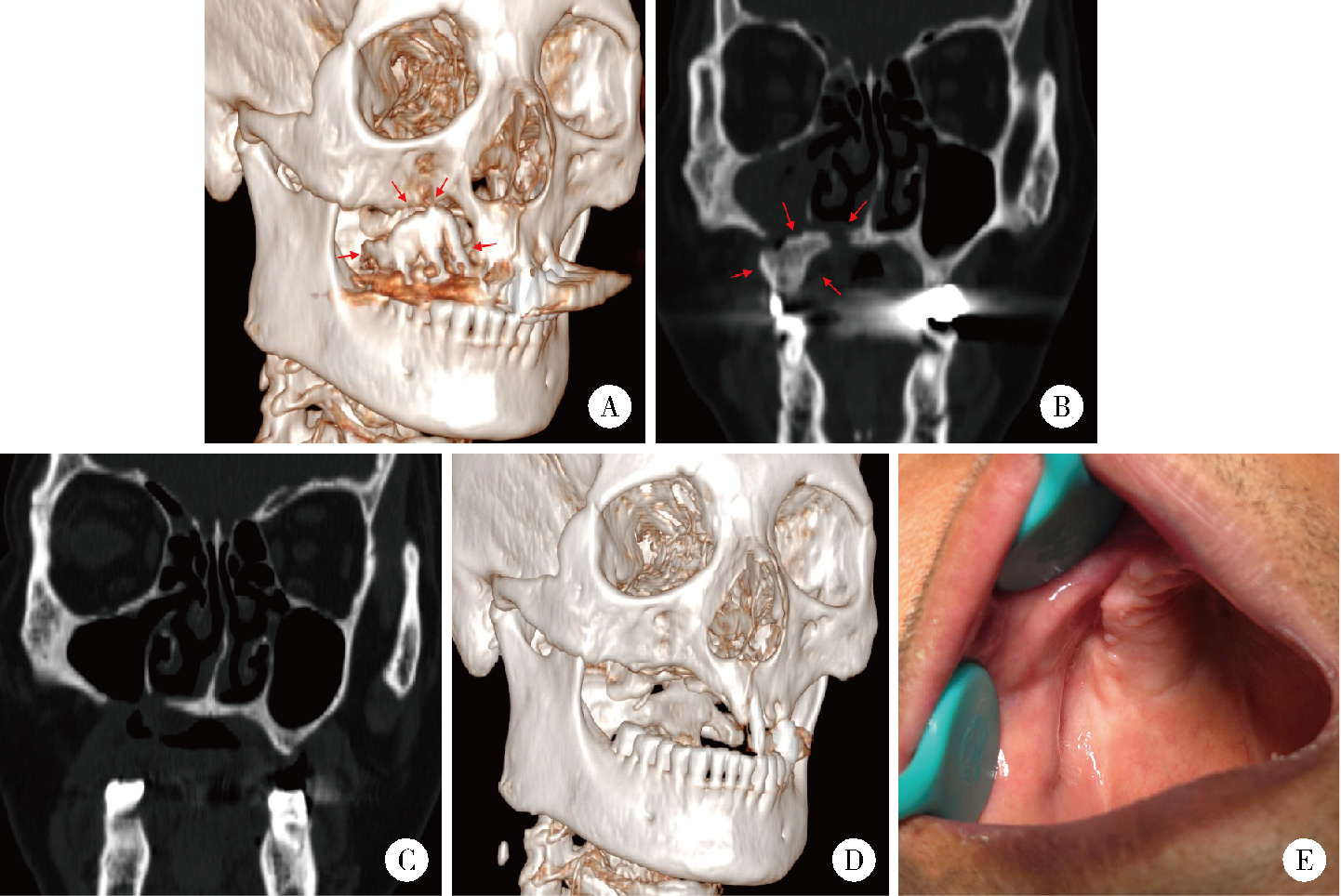
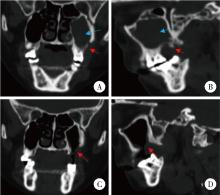
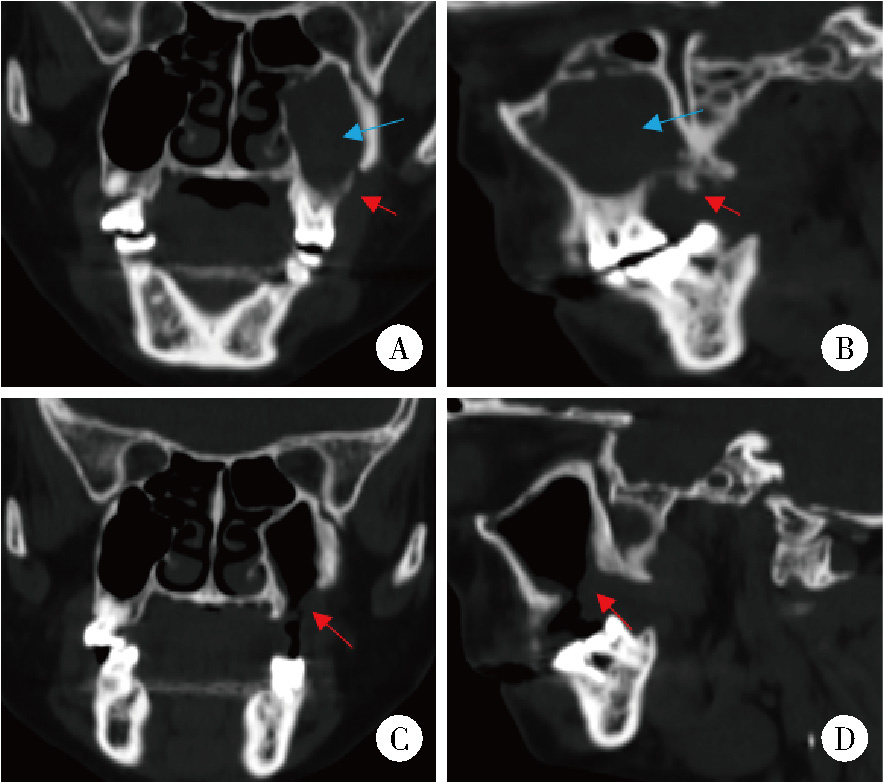
Surgical treatment outcomes of different stages of maxillary medication-related osteonecrosis of the jaw
Ebrahimi Farin1, Zhiqiang FENG2, Ebrahimi Faraz3, Weihua HAN4, Ziyang YU4, Kuankuan JIA1, Jingang AN1,*( )
)
- 1. Department of Oral and Maxillofacial Surgery, Peking University School and Hospital of Stomatology & National Center for Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Research Center of Oral Biomaterials and Digital Medical Devices, Beijing 100081, China
2. Department of Stomatology, Hebei Medical University Third Hospital, Shijiazhuang 050051, China
3. Department of Prosthodontics, Peking University School and Hospital of Stomatology, Beijing 100081, China
4. Department of Stomatology, Academy of Medical Sciences & Peking Union Medical College, Peking Union Medical College Hospital, Beijing 100730, China
CLC Number:
- R782



| 1 |
doi: 10.1136/bcr-2018-224455 |
| 2 |
doi: 10.1016/j.joms.2020.05.037 |
| 3 |
|
| 4 |
doi: 10.1111/odi.12992 |
| 5 |
doi: 10.1111/odi.13615 |
| 6 |
doi: 10.1016/j.jds.2020.12.007 |
| 7 |
doi: 10.3390/ijerph19127430 |
| 8 |
田美, 王丹妮, 罗舒艳, 等. 上颌骨药物相关性颌骨坏死的手术治疗效果初探[J]. 中华口腔医学杂志, 2021, 56 (5): 447- 451.
|
| 9 |
何悦, 陈珩, 安金刚, 等. 药物相关性颌骨坏死临床诊疗专家共识[J]. 中国口腔颌面外科杂志, 2023, 21 (4): 313- 325.
|
| 10 |
doi: 10.2214/ajr.156.2.1898819 |
| 11 |
doi: 10.1111/idj.12186 |
| 12 |
doi: 10.1016/j.joms.2022.02.008 |
| 13 |
doi: 10.1016/j.jcms.2016.05.018 |
| 14 |
doi: 10.1016/j.jcms.2016.08.001 |
| 15 |
doi: 10.1016/j.jds.2024.03.006 |
| 16 |
doi: 10.1016/j.joms.2016.12.011 |
| 17 |
doi: 10.1016/j.jcms.2020.02.017 |
| 18 |
doi: 10.3390/jcm10194480 |
| 19 |
|
| 20 |
doi: 10.1016/j.joms.2017.09.021 |
| 21 |
doi: 10.3390/jcm12154909 |
| 22 |
doi: 10.3390/ijerph192114543 |
| 23 |
doi: 10.1007/s10006-021-00973-9 |
| 24 |
doi: 10.1016/j.jcms.2018.03.005 |
| [1] | Lianfei PAN, Wenjing LI, Ruiyang WANG, Jian JIAO, Zhanqiang CAO, Li GAO, Dong SHI. Short-term efficacy and influencing factors of systemic antibiotics as an adjunct to mechanical periodontal therapy for stages Ⅲ/Ⅳ periodontitis [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 30-36. |
| [2] | Ziyang YU, Houzuo GUO, Xi JIANG, Weihua HAN, Ye LIN. Imaging study of osteogenesis in maxillary sinus segment of zygomatic implants [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 967-974. |
| [3] | Yuanyuan YANG, Shanshan ZHANG, Guangyan YU, Huijun YANG, Hongyu YANG. Clinical outcomes of partial sialoadenectomy for the treatment of benign tumors in the submandibular gland [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 334-339. |
| [4] | Ju YANG, Yue LIU, Chunna QU, Jianbin SUN, Tianying LI, Lianjie SHI. Bisphosphonates-related osteonecrosis of the jaw: A case report [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 388-392. |
| [5] | Yifan KANG, Yanjun GE, Xiaoming LV, Shang XIE, Xiaofeng SHAN, Zhigang CAI. One-stage mandibular reconstruction combining iliac flap with immediate implant-based denture [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 78-84. |
| [6] | Wenjing LI,Baozhou ZHANG,Heng LI,Liangpeng LAI,Hui DU,Ning SUN,Xiaofeng GONG,Ying LI,Yan WANG,Yong WU. Tibiotalocalcaneal arthrodesis for end-stage ankle and hindfoot arthropathy: Short- and mid-term clinical outcomes [J]. Journal of Peking University (Health Sciences), 2024, 56(2): 299-306. |
| [7] | Ying ZHOU,Ning ZHAO,Hongyuan HUANG,Qingxiang LI,Chuanbin GUO,Yuxing GUO. Left mandibular osteonecrosis following herpes zoster of the third branch of left trigeminal nerve: A case report [J]. Journal of Peking University (Health Sciences), 2024, 56(2): 366-370. |
| [8] | Chen CHEN,Yuhong LIANG. Root canal therapy of maxillary molars with atypical canals: A report of three cases [J]. Journal of Peking University (Health Sciences), 2024, 56(1): 190-195. |
| [9] | Ying ZHOU,Ning ZHAO,Hongyuan HUANG,Qingxiang LI,Chuanbin GUO,Yuxing GUO. Application of double-layer soft tissue suture closure technique in the surgical treatment of patients with mandible medication-related osteonecrosis of the jaw of early and medium stages [J]. Journal of Peking University (Health Sciences), 2024, 56(1): 51-56. |
| [10] | Sui LI,Wenjie MA,Shimin WANG,Qian DING,Yao SUN,Lei ZHANG. Trueness of different digital design methods for incisal guidance of maxillary anterior implant-supported single crowns [J]. Journal of Peking University (Health Sciences), 2024, 56(1): 81-87. |
| [11] | Xue ZOU,Xiao-juan BAI,Li-qing ZHANG. Effectiveness of tofacitinib combined with iguratimod in the treatment of difficult-to-treat moderate-to-severe rheumatoid arthritis [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 1013-1021. |
| [12] | Min QIU,You-long ZONG,Bin-shuai WANG,Bin YANG,Chu-xiao XU,Zheng-hui SUN,Min LU,Lei ZHAO,Jian LU,Cheng LIU,Xiao-jun TIAN,Lu-lin MA. Treatment outcome of laparoscopic partial nephrectomy in patients with renal tumors of moderate to high complexity [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 833-837. |
| [13] | Ying HUANG,Zhi-yuan WU,Xing-hong ZHOU,Zhi-gang CAI,Jie ZHANG. Category of facial symmetry perception after maxillary reconstruction using anterolateral thigh flap [J]. Journal of Peking University (Health Sciences), 2023, 55(4): 708-715. |
| [14] | Lei WANG,Tian-dong HAN,Wei-xing JIANG,Jun LI,Dao-xin ZHANG,Ye TIAN. Comparison of safety and effectiveness of active migration technique and in situ lithotripsy technique in the treatment of 1-2 cm upper ureteral calculi by flexible ure-teroscopy [J]. Journal of Peking University (Health Sciences), 2023, 55(3): 553-557. |
| [15] | Yu-xing GUO,Jian-yun ZHANG,Dian-can WANG,Chuan-bin GUO. Analysis of pathological characteristics of medication-related osteonecrosis of the jaw and discussion of clinical treatment strategies based on the pathological analysis results [J]. Journal of Peking University (Health Sciences), 2022, 54(6): 1190-1195. |
|
||