Journal of Peking University (Health Sciences) ›› 2022, Vol. 54 ›› Issue (6): 1079-1085. doi: 10.19723/j.issn.1671-167X.2022.06.004
Previous Articles Next Articles
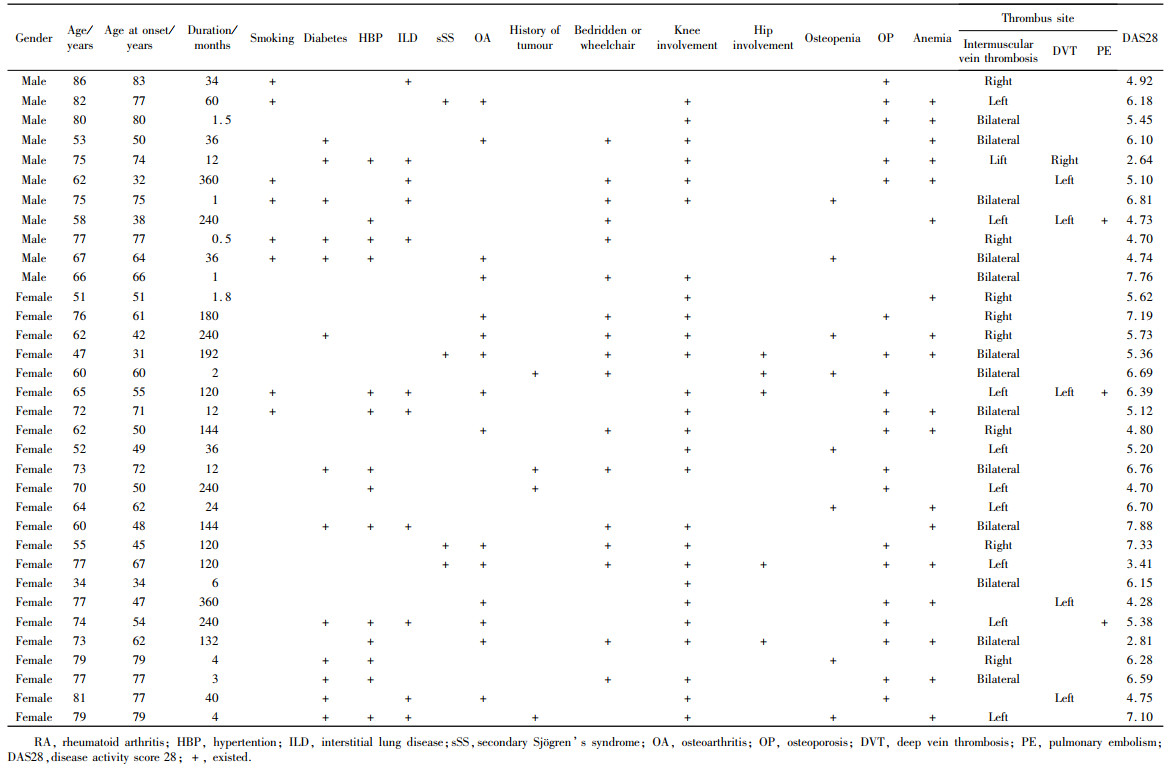
Clinical characteristics of patients with rheumatoid arthritis complicated with venous thrombosis of lower extremities
Rui LIU1,Jin-xia ZHAO1,*( ),Liang YAN1,2
),Liang YAN1,2
- 1. Department of Rheumatology and Immunology, Peking University Third Hospital, Beijing 100191, China
2. Department of Emergency, Yan'an Branch of Peking University Third Hospital (Traditional Chinese Medicine Hospital of Yan'an), Yan'an 716000, Shaanxi, China
CLC Number:
- R593.2
| 1 |
Li LY , Lu N , Avina-Galindo AM , et al. The risk and trend of pulmonary embolism and deep vein thrombosis in rheumatoid arthritis: A general population-based study[J]. Rheumatology (Oxford), 2021, 60 (1): 188- 195.
doi: 10.1093/rheumatology/keaa262 |
| 2 |
Matta F , Singala R , Yaekoub AY , et al. Risk of venous thromboembolism with rheumatoid arthritis[J]. Thromb Haemost, 2009, 101 (1): 134- 138.
doi: 10.1160/TH08-08-0551 |
| 3 |
Arnett FC , Edworthy SM , Bloch DA , et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis[J]. Arthritis Rheum, 1988, 31 (3): 315- 324.
doi: 10.1002/art.1780310302 |
| 4 |
Britsemmer K , Ursum J , Gerritsen M , et al. Validation of the 2010 ACR/EULAR classification criteria for rheumatoid arthritis: Slight improvement over the 1987 ACR criteria[J]. Ann Rheum Dis, 2011, 70 (8): 1468- 1470.
doi: 10.1136/ard.2010.148619 |
| 5 |
Chopard R , Albertsen IE , Piazza G . Diagnosis and treatment of lower extremity venous thromboembolism: A review[J]. JAMA, 2020, 324 (17): 1765- 1776.
doi: 10.1001/jama.2020.17272 |
| 6 |
Arshad N , Isaksen T , Hansen JB , et al. Time trends in incidence rates of venous thromboembolism in a large cohort recruited from the general population[J]. Eur J Epidemiol, 2017, 32 (4): 299- 305.
doi: 10.1007/s10654-017-0238-y |
| 7 |
Meng K , Hu X , Peng X , et al. Incidence of venous thromboembolism during pregnancy and the puerperium: A systematic review and meta-analysis[J]. J Matern Fetal Neonatal Med, 2015, 28 (3): 245- 253.
doi: 10.3109/14767058.2014.913130 |
| 8 | Croles FN , Nasserinejad K , Duvekot JJ , et al. Pregnancy, thrombophilia, and the risk of a first venous thrombosis: systematic review and Bayesian meta-analysis[J]. BMJ, 2017, 359, j4452. |
| 9 | Crous-Bou M , de Vivo I , Camargo CA Jr. , et al. Interactions of established risk factors and a GWAS-based genetic risk score on the risk of venous thromboembolism[J]. Thromb Haemost, 2016, 116 (4): 705- 713. |
| 10 | Heit JA , Ashrani A , Crusan DJ , et al. Reasons for the persistent incidence of venous thromboembolism[J]. ThrombHaemost, 2017, 117 (2): 390- 400. |
| 11 |
Mean M , Limacher A , Stalder O , et al. Do factor V Leiden and prothrombin G20210A mutations predict recurrent venous thromboembolism in older patients?[J]. Am J Med, 2017, 130 (10): 1220.e17- 1220.e22.
doi: 10.1016/j.amjmed.2017.05.026 |
| 12 |
Gregson J , Kaptoge S , Bolton T , et al. Cardiovascular risk factors associated with venous thromboembolism[J]. JAMA Cardiol, 2019, 4 (2): 163- 173.
doi: 10.1001/jamacardio.2018.4537 |
| 13 |
Peng YH , Lin YS , Chen CH , et al. Type 1 diabetes is associated with an increased risk of venous thromboembolism: A retrospective population-based cohort study[J]. PLoS One, 2020, 15 (1): e0226997.
doi: 10.1371/journal.pone.0226997 |
| 14 |
Riva N , Donadini MP , AgenoW . Epidemiology and pathophysiology of venous thromboembolism: Similarities with atherothrombosis and the role of inflammation[J]. Thromb Haemost, 2015, 113 (6): 1176- 1183.
doi: 10.1160/TH14-06-0563 |
| 15 |
Chen CY , Liao KM . The incidence of deep vein thrombosis in Asian patients with chronic obstructive pulmonary disease[J]. Medicine (Baltimore), 2015, 94 (44): e1741.
doi: 10.1097/MD.0000000000001741 |
| 16 |
Ogdie A , McGill NK , Shin DB , et al. Risk of venous thromboembolism in patients with psoriatic arthritis, psoriasis and rheumatoid arthritis: A general population-based cohort study[J]. Eur Heart J, 2018, 39 (39): 3608- 3614.
doi: 10.1093/eurheartj/ehx145 |
| 17 |
Lurie JM , Png CYM , Subramaniam S , et al. Virchow's triad in "silent" deep vein thrombosis[J]. J Vasc Surg Venous Lymphat Disord, 2019, 7 (5): 640- 645.
doi: 10.1016/j.jvsv.2019.02.011 |
| 18 | Broussard J , Berlinger M , Lauret D . A clot (possibly): Due to loss of TNF-α supression[J]. J La State Med Soc, 2017, 169 (2): 52. |
| 19 |
Mease P , Charles-Schoeman C , Cohen S , et al. Incidence of venous and arterial thromboembolic events reported in the tofacitinib rheumatoid arthritis, psoriasis and psoriatic arthritis development programmes and from real-world data[J]. Ann Rheum Dis, 2020, 79 (11): 1400- 1413.
doi: 10.1136/annrheumdis-2019-216761 |
| 20 |
Arshad N , Isaksen T , Hansen JB , et al. Time trends in incidence rates of venous thromboembolism in a large cohort recruited from the general population[J]. Eur J Epidemiol, 2017, 32 (4): 299- 305.
doi: 10.1007/s10654-017-0238-y |
| [1] | Hui WEI, Jingfeng ZHANG, Zhongqiang YAO, Jinxia ZHAO. Clinical characteristics and relevant factors of rheumatoid arthritis patients with anemia of chronic disease [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 307-312. |
| [2] | Tao WU, Jianzi LIN, Yafeng ZHU, Jianda MA, Peiwen JIA, Lijuan YANG, jie PAN, Yaowei ZOU, Ying YANG, Ye LU, Lie DAI. Serum inter-alpha-trypsin inhibitor heavy chain H3 is identified as a potential biomarker for myopenia in patients with rheumatoid arthritis using proteomic profiling [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1024-1031. |
| [3] | Yan DING, Lifang WANG, Chaoran LI, Zhemin LU, Lianjie SHI. Rheumatoid arthritis combined with IgG4-related disease successfully treated with rituximab: A case report [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1203-1207. |
| [4] | Ju YANG, Jing XU, Juhua DAI, Lianjie SHI. Expression of lumican protein in serum of patients with rheumatoid arthritis and its correlation with disease and immune activities [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 911-918. |
| [5] | Lianghua FENG, Lirong HONG, Yujia CHEN, Xueming CAI. Role and mechanism of ubiquitin-specific protease 35 in ferroptosis of rheumatoid arthritis-fibroblast like synoviocytes [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 919-925. |
| [6] | Peiwen JIA, Ying YANG, Yaowei ZOU, Zhiming OUYANG, Jianzi LIN, Jianda MA, Kuimin YANG, Lie DAI. Clinical characteristics of overlapping syndromes of low muscle mass in patients with rheumatoid arthritis and their impact on physical function [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1009-1016. |
| [7] | Yinji JIN, Rui LIU. Hereditary protein S deficiency in a patient with prominent mesenteric venous thrombosis: A case report [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1106-1109. |
| [8] | Doudou MA, Zhemin LU, Qian GUO, Sha ZHU, Jin GU, Yan DING, Lianjie SHI. Successful treatment of rheumatoid arthritis complicated with myasthenia gravis with low-dose rituximab: A case report [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1110-1114. |
| [9] | Rui YAN, Dan KE, Yan ZHANG, Li LI, Huanran SU, Wei CHEN, Mingxia SUN, Xiaomin LIU, Liang LUO. Diagnostic significance of serum chemokine CXCL-10 and Krebs von den lungen-6 level in patients with rheumatoid arthritis associated interstitial lung disease [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 956-962. |
| [10] | Liang ZHAO, Chenglong SHI, Ke MA, Jing ZHAO, Xiao WANG, Xiaoyan XING, Wanxing MO, Yirui LIAN, Chao GAO, Yuhui LI. Immunological characteristics of patients with anti-synthetase syndrome overlap with rheumatoid arthritis [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 972-979. |
| [11] | Yijun HAN, Xiaoli CHEN, Changhong LI, Jinxia ZHAO. Application status of methotrexate in patients with rheumatoid arthritis [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 994-1000. |
| [12] | Dongwu LIU, Jie CHEN, Mingli GAO, Jing YU. Rheumatoid arthritis with Castleman-like histopathology in lymph nodes: A case report [J]. Journal of Peking University (Health Sciences), 2024, 56(5): 928-931. |
| [13] | Huina HUANG,Jing ZHAO,Xiangge ZHAO,Ziran BAI,Xia LI,Guan WANG. Regulatory effect of lactate on peripheral blood CD4+ T cell subsets in patients with rheumatoid arthritis [J]. Journal of Peking University (Health Sciences), 2024, 56(3): 519-525. |
| [14] | Xiaofei TANG,Yonghong LI,Qiuling DING,Zhuo SUN,Yang ZHANG,Yumei WANG,Meiyi TIAN,Jian LIU. Incidence and risk factors of deep vein thrombosis in patients with rheumatoid arthritis [J]. Journal of Peking University (Health Sciences), 2024, 56(2): 279-283. |
| [15] | Xue ZOU,Xiao-juan BAI,Li-qing ZHANG. Effectiveness of tofacitinib combined with iguratimod in the treatment of difficult-to-treat moderate-to-severe rheumatoid arthritis [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 1013-1021. |
|
||