Journal of Peking University (Health Sciences) ›› 2024, Vol. 56 ›› Issue (4): 673-679. doi: 10.19723/j.issn.1671-167X.2024.04.021
Previous Articles Next Articles
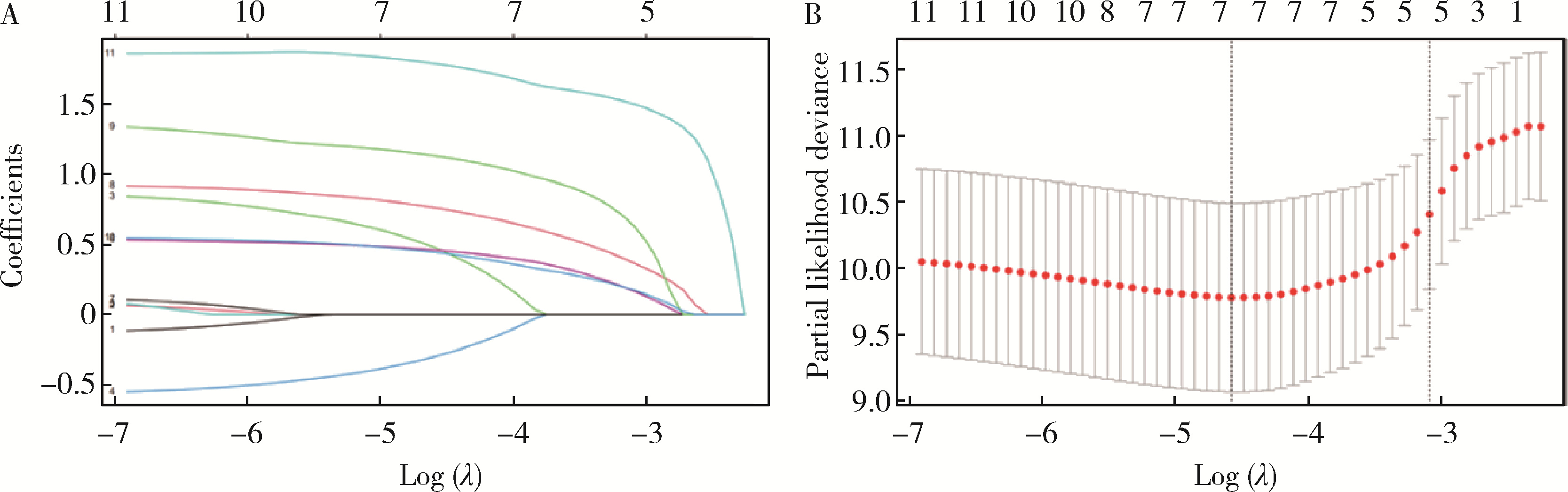
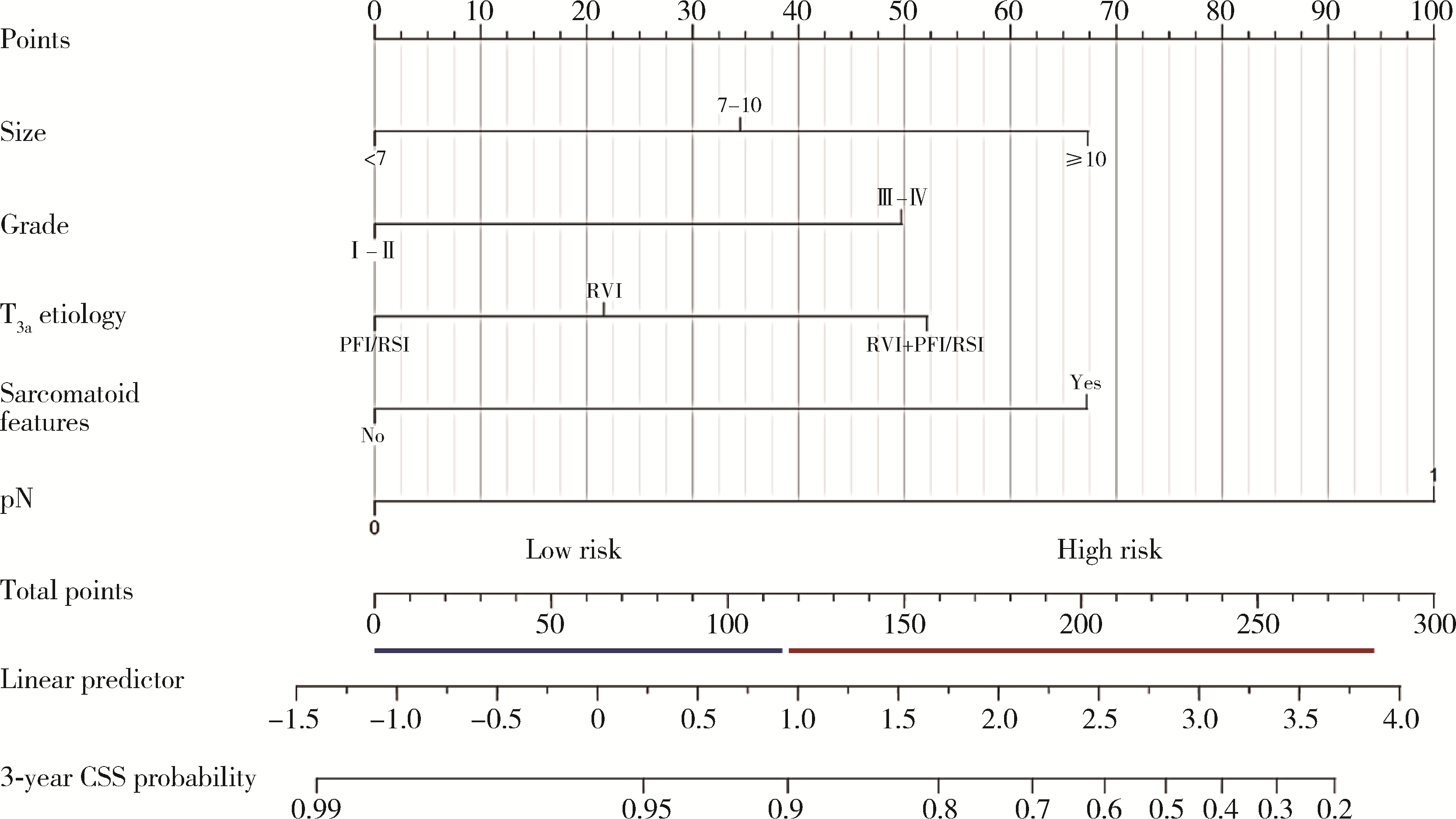
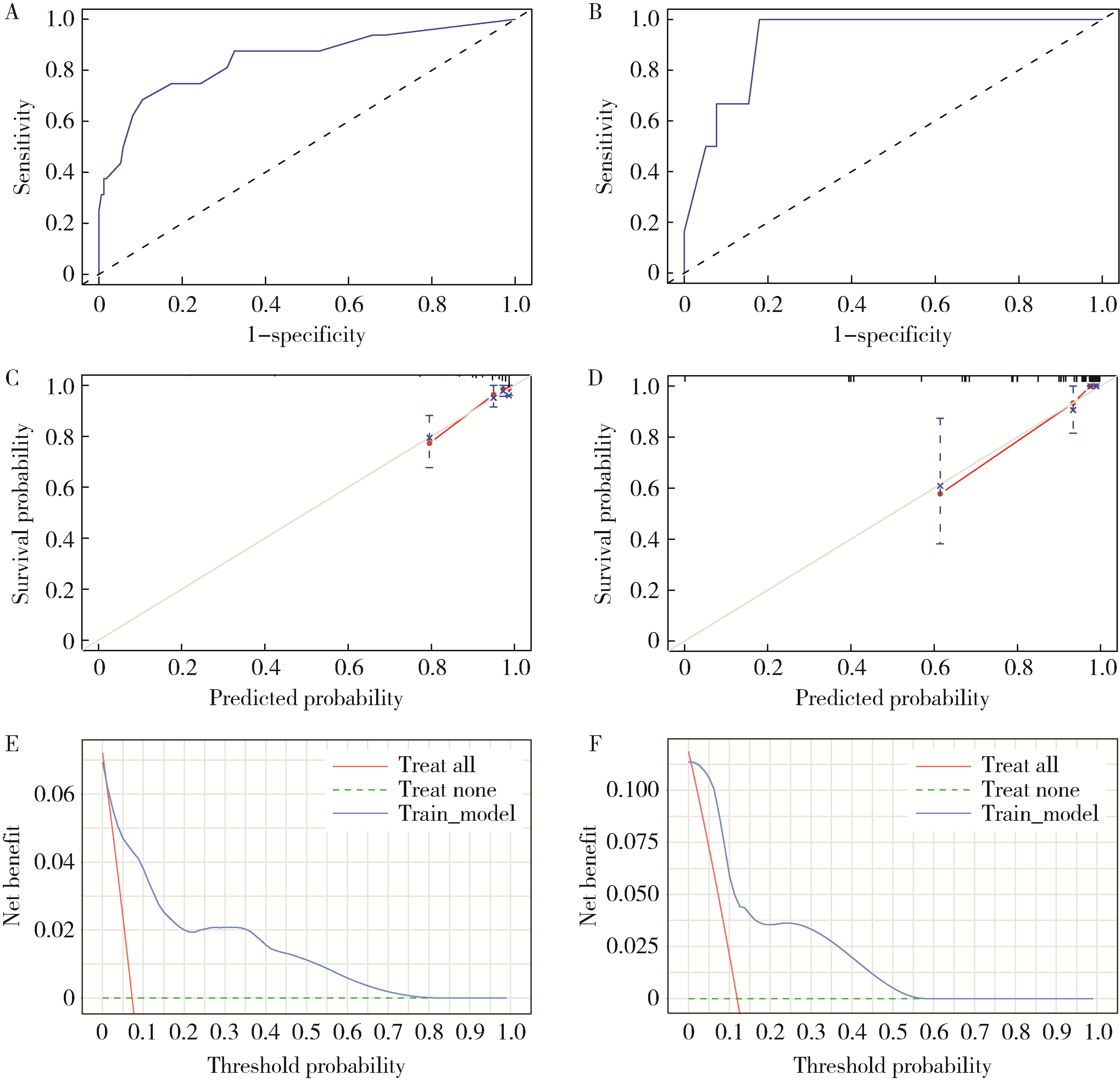
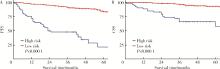
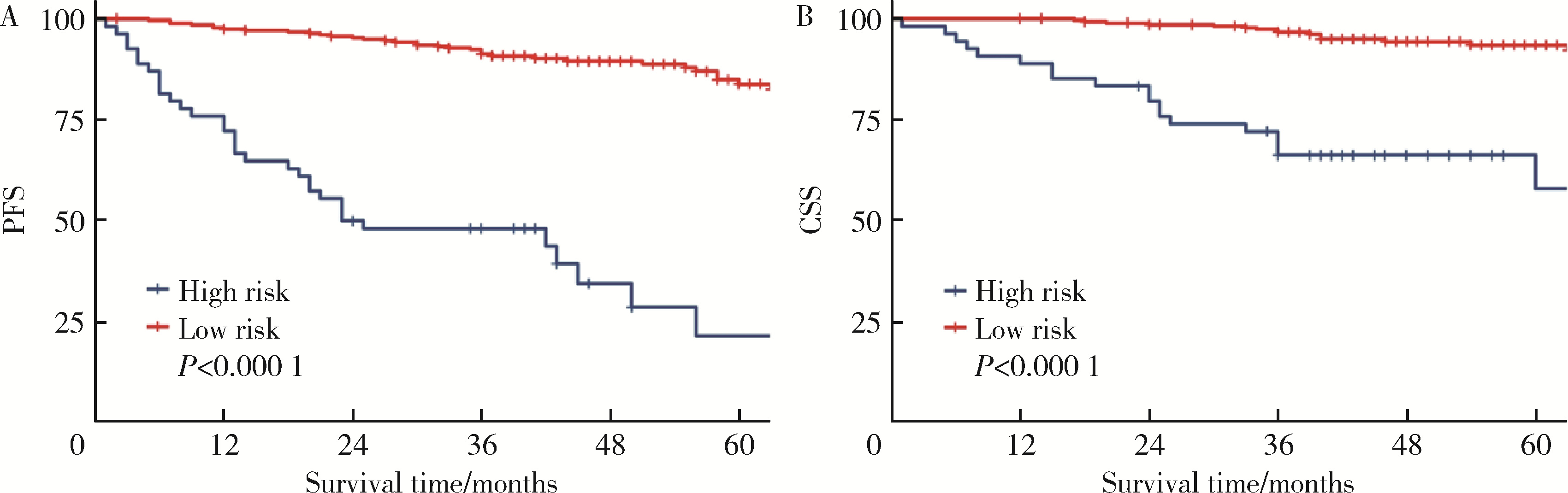
Predicting the 3-year tumor-specific survival in patients with T3a non-metastatic renal cell carcinoma
Zezhen ZHOU,Shaohui DENG,Ye YAN,Fan ZHANG,Yichang HAO,Liyuan GE,Hongxian ZHANG,Guoliang WANG,Shudong ZHANG*( )
)
- Department of Urology, Peking University Third Hospital, Beijing 100191, China
CLC Number:
- R737.11


| 1 |
Elkassem AA , Allen BC , Sharbidre KG , et al. Update on the role of imaging in clinical staging and restaging of renal cell carcinoma based on the AJCC 8th edition, from the AJR special series on cancer staging[J]. AJR Am J Roentgenol, 2021, 217 (3): 541- 555.
doi: 10.2214/AJR.21.25493 |
| 2 |
Guo P , Wang Y , Han Y , et al. Development and validation of a nomogram to predict postoperative cancer-specific survival of patients with nonmetastatic T3a renal cell carcinoma[J]. Urol Oncol, 2021, 39 (12): 835.e19- 835.e27.
doi: 10.1016/j.urolonc.2021.06.014 |
| 3 |
Musso G , Fallara G , Rosiello G , et al. Differential prognostic value of extrarenal involvement in patients with non-metastatic renal cell cancer[J]. Clin Genitourin Cancer, 2023, 21 (4): e279- e285.e1.
doi: 10.1016/j.clgc.2023.02.008 |
| 4 |
Shah PH , Lyon TD , Lohse CM , et al. Prognostic evaluation of perinephric fat, renal sinus fat, and renal vein invasion for patients with pathological stage T3a clear-cell renal cell carcinoma[J]. BJU Int, 2019, 123 (2): 270- 276.
doi: 10.1111/bju.14523 |
| 5 |
Li L , Shi L , Zhang J , et al. The critical impact of tumor size in predicting cancer special survival for T3aM0M0 renal cell carcinoma: A proposal of an alternative T3aN0M0 stage[J]. Cancer Med, 2021, 10 (2): 605- 614.
doi: 10.1002/cam4.3629 |
| 6 |
Lam JS , Klatte T , Patard JJ , et al. Prognostic relevance of tumour size in T3a renal cell carcinoma: A multicentre experience[J]. Eur Urol, 2007, 52 (1): 155- 162.
doi: 10.1016/j.eururo.2007.01.106 |
| 7 |
Tan WS , Koelker M , Campain N , et al. Comparison of long-term outcomes for young and healthy patients with cT1a and cT3a renal cell carcinoma treated with partial nephrectomy[J]. Eur Urol Focus, 2023, 9 (2): 333- 335.
doi: 10.1016/j.euf.2022.09.018 |
| 8 | Chung DY , Kang DH , Kim JW , et al. Comparison of oncologic outcomes between partial nephrectomy and radical nephrectomy in patients who were upstaged from cT1 renal tumor to pT3a renal cell carcinoma: An updated systematic review and meta-analysis[J]. Ther Adv Urol, 2020, 12, 1756287220981508. |
| 9 |
Deng H , Fan Y , Yuan F , et al. Partial nephrectomy provides equivalent oncologic outcomes and better renal function preservation than radical nephrectomy for pathological T3a renal cell carcinoma: A meta-analysis[J]. Int Braz J Urol, 2021, 47 (1): 46- 60.
doi: 10.1590/s1677-5538.ibju.2020.0167 |
| 10 |
Liu H , Kong QF , Li J , et al. A meta-analysis for comparison of partial nephrectomy vs. radical nephrectomy in patients with pT3a renal cell carcinoma[J]. Transl Androl Urol, 2021, 10 (3): 1170- 1178.
doi: 10.21037/tau-20-1262 |
| 11 |
Liu Z , Yang Z , Li J , et al. Partial versus radical nephrectomy for the treatment of pT3aN0M0 renal cell carcinoma: A propensity score analysis[J]. Asian J Surg, 2023, 46 (9): 3607- 3613.
doi: 10.1016/j.asjsur.2023.04.058 |
| [1] | Bo PENG, Fangfang LIU, Wei YANG, Ruiping XU, Lei CHEN, Baozhong LI, Xinjia WANG, Ji KE, Wenlei YANG, Yu HE, Zhen LIU, Bolin HOU, Liqun ZHANG, Miaoping LIN, Lixin ZHANG, Fan ZHANG, Fen CAI, Huawen XU, Mengfei LIU, Ying LIU, Yaqi PAN, Zhonghu HE, Yang KE. Perioperative hyperglycemia predicts poorer prognosis of esophageal squamous cell carcinoma patients treated with esophagectomy [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 567-574. |
| [2] | Fan SHU, Liyuan GE, Hanzhang DENG, Haoming YIN, Junyong OU, Shaohui DENG, Yichang HAO, Min LU, Zhanyi ZHANG, Peichen DUAN, Shudong ZHANG. Molecular characteristics for poor prognosis related renal cell carcinoma with lymph metastases [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 631-640. |
| [3] | Haoming YIN, Zijie WANG, Fan SHU, Zhanyi ZHANG, Hui LIANG, Shudong ZHANG. Expression and significance of the FABP6 long transcript in clear cell renal cell carcinoma [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 393-398. |
| [4] | Lingfu ZHANG, Ming CHEN, Xiaoyu ZHAO, Gang WANG, Long CUI, Xiaofeng LING, Lixin WANG, Zhi XU, Limei GUO, Chunsheng HOU. Gross classification of gallbladder cancer with primary lesion limited to the gallbladder wall and its correlation with prognosis and precancerous lesions [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 184-189. |
| [5] | Bowen LI, Qiang ZHANG, Yixin SUN. Establishment and validation of a risk prediction model for scoliosis after Nuss procedure in children and young adults with pectus excavatum [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 941-946. |
| [6] | Boda GUO, Min LU, Guoliang WANG, Hongxian ZHANG, Lei LIU, Xiaofei HOU, Lei ZHAO, Xiaojun TIAN, Shudong ZHANG. Clinicopathological and prognostic differences between clear cell and non-clear cell renal cell carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 644-649. |
| [7] | Zhanyi ZHANG, Min LU, Yuehao SUN, Jinghan DONG, Xiaofei HOU, Chunlei XIAO, Guoliang WANG, Xiaojun TIAN, Lulin MA, Hongxian ZHANG, Shudong ZHANG. Clinicopathological features and survival analysis of TFE3-rearranged renal cell carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 650-661. |
| [8] | Zezhen ZHOU, Liyuan GE, Fan ZHANG, Shaohui DENG, Ye YAN, Hongxian ZHANG, Guoliang WANG, Lei LIU, Yi HUANG, Shudong ZHANG. A retrospective matching study of partial nephrectomy and radical nephrectomy for pathological T3a stage renal cell carcinoma [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 704-710. |
| [9] | Weihao LI, Jing LI, Xuemin ZHANG, Wei LI, Qingle LI, Xiaoming ZHANG. Effect of intraoperative blood salvage autotransfusion on the prognosis of patients after carotid body tumor resection [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 272-276. |
| [10] | Yaqing MAO, Zhen CHEN, Yao YU, Wenbo ZHANG, Yang LIU, Xin PENG. Impact of type 2 diabetes mellitus on the prognosis of patients with oral squamous cell carcinoma [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1089-1096. |
| [11] | Yuanmei LIU, Yicheng FU, Jingxin HAO, Fuchun ZHANG, Huilin LIU. Construction and validation of a nomogram for predicting in-hospital postoperative heart failure in elderly patients with hip fracture [J]. Journal of Peking University (Health Sciences), 2024, 56(5): 874-883. |
| [12] | Zhicun LI, Tianyu WU, Lei LIANG, Yu FAN, Yisen MENG, Qian ZHANG. Risk factors analysis and nomogram model construction of postoperative pathological upgrade of prostate cancer patients with single core positive biopsy [J]. Journal of Peking University (Health Sciences), 2024, 56(5): 896-901. |
| [13] | Junyong OU,Kunming NI,Lulin MA,Guoliang WANG,Ye YAN,Bin YANG,Gengwu LI,Haodong SONG,Min LU,Jianfei YE,Shudong ZHANG. Prognostic factors of patients with muscle invasive bladder cancer with intermediate-to-high risk prostate cancer [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 582-588. |
| [14] | Shuai LIU,Lei LIU,Zhuo LIU,Fan ZHANG,Lulin MA,Xiaojun TIAN,Xiaofei HOU,Guoliang WANG,Lei ZHAO,Shudong ZHANG. Clinical treatment and prognosis of adrenocortical carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 624-630. |
| [15] | Le YU,Shaohui DENG,Fan ZHANG,Ye YAN,Jianfei YE,Shudong ZHANG. Clinicopathological characteristics and prognosis of multilocular cystic renal neoplasm of low malignant potential [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 661-666. |
|
||