Journal of Peking University (Health Sciences) ›› 2023, Vol. 55 ›› Issue (1): 13-21. doi: 10.19723/j.issn.1671-167X.2023.01.003
Previous Articles Next Articles
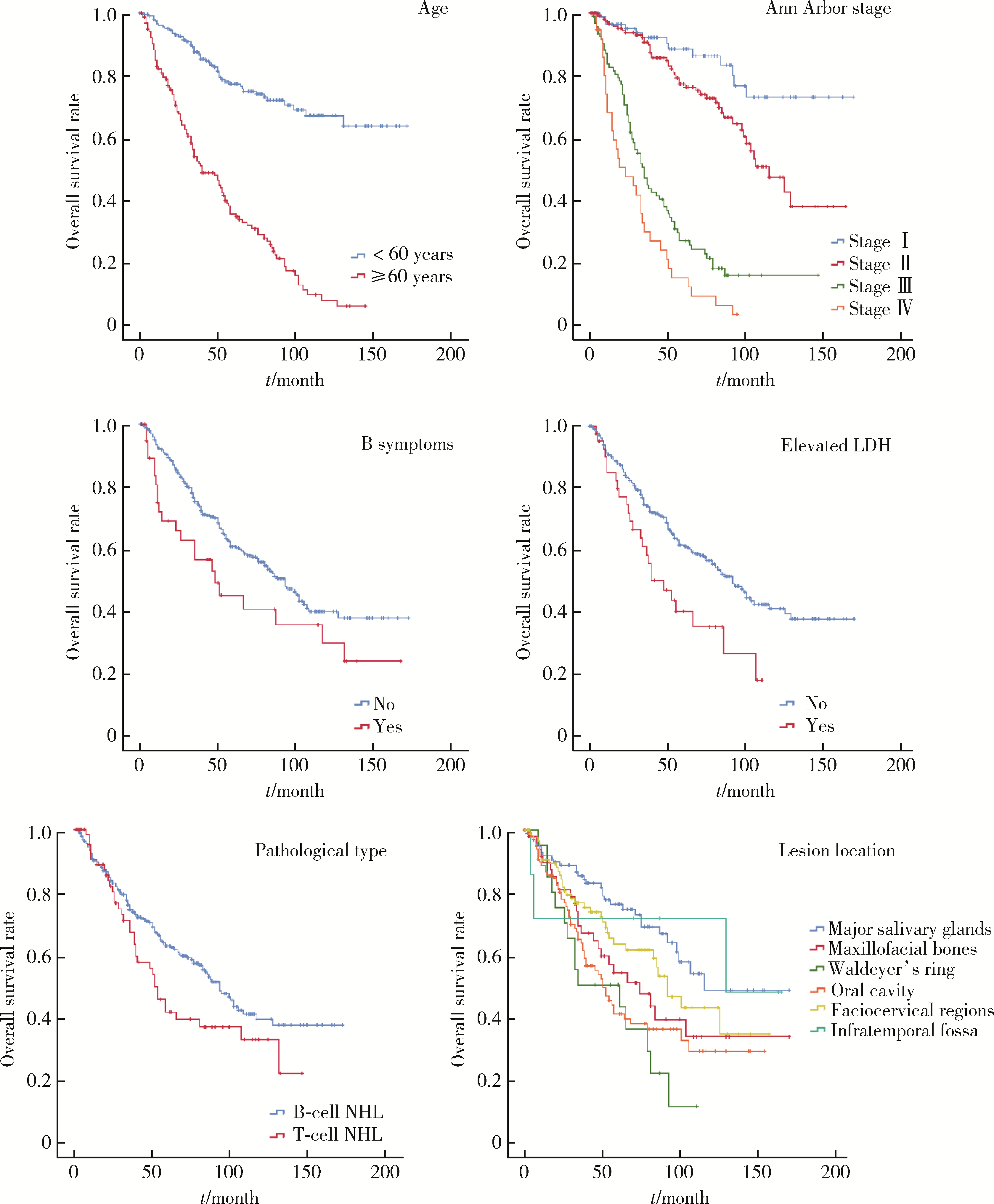
Clinicopathological characteristics and prognosis of non-Hodgkin lymphoma in oral and maxillofacial regions: An analysis of 369 cases
Qian SU1,Xin PENG1,Chuan-xiang ZHOU2,*( ),Guang-yan YU1,*()
),Guang-yan YU1,*()
- 1. Department of Oral and Maxillofacial Surgery, Peking University School and Hospital of Stomatology & National Center of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Research Center of Oral Biomaterials and Digital Medical Devices & Beijing Key Laboratory of Digital Stomato-logy & NHC Research Center of Engineering and Technology for Computerized Dentistry & NMPA Key Laboratory for Dental Materials, Beijing 100081, China
2. Department of Oral Pathology, Peking University School and Hospital of Stomatology & National Center of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Research Center of Oral Biomaterials and Digital Medical Devices & Beijing Key Laboratory of Digital Stomato-logy & NHC Research Center of Engineering and Technology for Computerized Dentistry & NMPA Key Laboratory for Dental Materials, Beijing 100081, China
CLC Number:
- R739.8



| 1 | 李小秋, 李甘地, 高子芬, 等. 中国淋巴瘤亚型分布: 国内多中心性病例10 002例分析[J]. 诊断学理论与实践, 2012, 11 (2): 111- 115. |
| 2 |
Zelenetz AD , Gordon LI , Abramson JS , et al. NCCN guidelines insights: B-cell lymphomas, version 3.2019[J]. J Natl Compr Canc Netw, 2019, 17 (6): 650- 661.
doi: 10.6004/jnccn.2019.0029 |
| 3 |
Skarin AT , Dorfman DM . Non-Hodgkin's lymphomas: Current classification and management[J]. CA Cancer J Clin, 1997, 47 (6): 351- 372.
doi: 10.3322/canjclin.47.6.351 |
| 4 | Swerdlow SH , Campo E , Harris NL , et al. WHO classification of tumours of haematopoietic and lymphoid tissues[M]. Lyon: IARC Press, 2008. |
| 5 |
Siegel RL , Miller KD , Fuchs HE , et al. Cancer satistics, 2021[J]. CA Cancer J Clin, 2021, 71 (1): 7- 33.
doi: 10.3322/caac.21654 |
| 6 |
Sung H , Ferlay J , Siegel RL , et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71 (3): 209- 249.
doi: 10.3322/caac.21660 |
| 7 |
庹吉妤, 张敏, 郑荣寿, 等. 2015年中国恶性淋巴瘤发病与死亡分析[J]. 中国肿瘤, 2021, 30 (1): 35- 40.
doi: 10.3969/j.issn.1000-8179.2021.01.726 |
| 8 |
温玉明, 代晓明, 王昌美, 等. 口腔颌面部恶性肿瘤6 539例临床病理分析[J]. 华西口腔医学杂志, 2001, 19 (5): 296- 299.
doi: 10.3321/j.issn:1000-1182.2001.05.008 |
| 9 |
Swerdlow SH , Campo E , Pileri SA , et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms[J]. Blood, 2016, 127 (20): 2375- 2390.
doi: 10.1182/blood-2016-01-643569 |
| 10 | The 2022 global patient survey on lymphoma & CLL. https://lymphomacoalition.org/wp-content/uploads/LC-2020-GPS-Global-Re-port-Final.pdf[Z]. Lymphoma Coalition, 2020. |
| 11 |
肖畅, 苏祖兰, 吴秋良, 等. 根据WHO新分类对493例非霍奇金淋巴瘤的临床病理分析[J]. 中华病理学杂志, 2005, 34 (1): 22- 27.
doi: 10.3760/j.issn:0529-5807.2005.01.007 |
| 12 |
Etemad-Moghadam S , Tirgary F , Keshavarz S , et al. Head and neck non-Hodgkin's lymphoma: A 20-year demographic study of 381 cases[J]. Int J Oral Maxillofac Surg, 2010, 39 (9): 869- 872.
doi: 10.1016/j.ijom.2010.03.029 |
| 13 |
Aoki R , Karube K , Sugita Y , et al. Distribution of malignant lymphoma in Japan: Analysis of 2 260 cases, 2001-2006[J]. Pathol Int, 2008, 58 (3): 174- 182.
doi: 10.1111/j.1440-1827.2007.02207.x |
| 14 | 杨小芸, 沈丽达, 龙庭凤, 等. 1 326例非霍奇金淋巴瘤临床病理特点分析[J]. 中华肿瘤防治杂志, 2016, 23 (9): 605- 609. |
| 15 |
Feinstein AJ , Ciarleglio MM , Cong X , et al. Parotid gland lymphoma: Prognostic analysis of 2 140 patients[J]. The Laryngoscope, 2013, 123 (5): 1199- 1203.
doi: 10.1002/lary.23901 |
| 16 | El-Naggar A , John K , Grandis J . WHO classification of head and neck tumours. WHO classification of tumours of the salivary glands[J]. Lyon: IARC Press, 2017, 160- 184. |
| 17 |
周立强, 孙燕, 谭文勇, 等. 非霍奇金淋巴瘤1 125例临床病理分析[J]. 癌症进展, 2006, 4 (5): 391- 397.
doi: 10.3969/j.issn.1672-1535.2006.05.004 |
| 18 |
Jaffe ES . Diagnosis and classification of lymphoma: Impact of technical advances[J]. Semin Hematol, 2019, 56 (1): 30- 36.
doi: 10.1053/j.seminhematol.2018.05.007 |
| 19 |
Salles G , Barrett M , Foà R , et al. Rituximab in B-cell hematologic malignancies: A review of 20 years of clinical experience[J]. Adv Ther, 2017, 34 (10): 2232- 2273.
doi: 10.1007/s12325-017-0612-x |
| 20 |
Berger GK , Mcbride A , Lawson S , et al. Brentuximab vedotin for treatment of non-Hodgkin lymphomas: A systematic review[J]. Crit Rev Oncol Hematol, 2017, 109, 42- 50.
doi: 10.1016/j.critrevonc.2016.11.009 |
| 21 |
Allemani C , Matsuda T , Di Carlo V , et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries[J]. Lancet, 2018, 391 (10125): 1023- 1075.
doi: 10.1016/S0140-6736(17)33326-3 |
| 22 | 马肖容, 徐燕, 王瑾, 等. 254例非霍奇金淋巴瘤的临床疗效与预后分析[J]. 中国实验血液学杂志, 2016, 24 (4): 1044- 1050. |
| 23 |
Cheson BD , Fisher RI , Barrington SF , et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification[J]. J Clin Oncol, 2014, 32 (27): 3059- 3068.
doi: 10.1200/JCO.2013.54.8800 |
| 24 | Chen SY , Yang Y , Qi SN , et al. Validation of nomogram-revised risk index and comparison with other models for extranodal nasal-type NK/T-cell lymphoma in the modern chemotherapy era: Indication for prognostication and clinical decision-making[J]. Leukemia, 2021, 35 (1): 130- 142. |
| 25 | Ruppert AS , Dixon JG , Salles G , et al. International prognostic indices in diffuse large B-cell lymphoma: A comparison of IPI, R-IPI, and NCCN-IPI[J]. Blood, 2020, 135 (23): 2041- 2048. |
| [1] | Bo PENG, Fangfang LIU, Wei YANG, Ruiping XU, Lei CHEN, Baozhong LI, Xinjia WANG, Ji KE, Wenlei YANG, Yu HE, Zhen LIU, Bolin HOU, Liqun ZHANG, Miaoping LIN, Lixin ZHANG, Fan ZHANG, Fen CAI, Huawen XU, Mengfei LIU, Ying LIU, Yaqi PAN, Zhonghu HE, Yang KE. Perioperative hyperglycemia predicts poorer prognosis of esophageal squamous cell carcinoma patients treated with esophagectomy [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 567-574. |
| [2] | Fan SHU, Liyuan GE, Hanzhang DENG, Haoming YIN, Junyong OU, Shaohui DENG, Yichang HAO, Min LU, Zhanyi ZHANG, Peichen DUAN, Shudong ZHANG. Molecular characteristics for poor prognosis related renal cell carcinoma with lymph metastases [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 631-640. |
| [3] | Lingfu ZHANG, Ming CHEN, Xiaoyu ZHAO, Gang WANG, Long CUI, Xiaofeng LING, Lixin WANG, Zhi XU, Limei GUO, Chunsheng HOU. Gross classification of gallbladder cancer with primary lesion limited to the gallbladder wall and its correlation with prognosis and precancerous lesions [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 184-189. |
| [4] | Xiaolin WANG, Luyao LI, Wen ZHANG, Hongyan WANG. Clinicopathological analysis of mesonephric-like adenocarcinoma in the corpusuteri: A report of 3 cases [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1208-1212. |
| [5] | Boda GUO, Min LU, Guoliang WANG, Hongxian ZHANG, Lei LIU, Xiaofei HOU, Lei ZHAO, Xiaojun TIAN, Shudong ZHANG. Clinicopathological and prognostic differences between clear cell and non-clear cell renal cell carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 644-649. |
| [6] | Weihao LI, Jing LI, Xuemin ZHANG, Wei LI, Qingle LI, Xiaoming ZHANG. Effect of intraoperative blood salvage autotransfusion on the prognosis of patients after carotid body tumor resection [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 272-276. |
| [7] | Guangyan YU, Xin PENG, Min GAO, Peng YE, Na GE, Mengqi JIA, Bingyu LI, Zunan TANG, Leihao HU, Wenbo ZHANG. Research progress in diagnosis and treatment of salivary gland tumors [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 1-6. |
| [8] | Yaqing MAO, Zhen CHEN, Yao YU, Wenbo ZHANG, Yang LIU, Xin PENG. Impact of type 2 diabetes mellitus on the prognosis of patients with oral squamous cell carcinoma [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1089-1096. |
| [9] | Junyong OU,Kunming NI,Lulin MA,Guoliang WANG,Ye YAN,Bin YANG,Gengwu LI,Haodong SONG,Min LU,Jianfei YE,Shudong ZHANG. Prognostic factors of patients with muscle invasive bladder cancer with intermediate-to-high risk prostate cancer [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 582-588. |
| [10] | Shuai LIU,Lei LIU,Zhuo LIU,Fan ZHANG,Lulin MA,Xiaojun TIAN,Xiaofei HOU,Guoliang WANG,Lei ZHAO,Shudong ZHANG. Clinical treatment and prognosis of adrenocortical carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 624-630. |
| [11] | Le YU,Shaohui DENG,Fan ZHANG,Ye YAN,Jianfei YE,Shudong ZHANG. Clinicopathological characteristics and prognosis of multilocular cystic renal neoplasm of low malignant potential [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 661-666. |
| [12] | Zezhen ZHOU,Shaohui DENG,Ye YAN,Fan ZHANG,Yichang HAO,Liyuan GE,Hongxian ZHANG,Guoliang WANG,Shudong ZHANG. Predicting the 3-year tumor-specific survival in patients with T3a non-metastatic renal cell carcinoma [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 673-679. |
| [13] | Yangyi FANG,Qiang LI,Zhigao HUANG,Min LU,Kai HONG,Shudong ZHANG. Well-differentiated papillary mesothelial tumour of the tunica vaginalis: A case report [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 741-744. |
| [14] | Yuanyuan ZENG,Yun XIE,Daonan CHEN,Ruilan WANG. Related factors of euthyroid sick syndrome in patients with sepsis [J]. Journal of Peking University (Health Sciences), 2024, 56(3): 526-532. |
| [15] | Jian-bin LI,Meng-na LYU,Qiang CHI,Yi-lin PENG,Peng-cheng LIU,Rui WU. Early prediction of severe COVID-19 in patients with Sjögren’s syndrome [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 1007-1012. |
|
||