

上尿路修复手术是针对肾盂及输尿管的先天畸形、病理狭窄、后天损伤等多种情况,进行尿路结构及功能重建的手术。根据不同病变位置及不同病变长度,应采用不同的手术方式。常见的手术方式包括肾盂成形术、输尿管-输尿管吻合术、输尿管膀胱再植术、膀胱瓣术、肠代输尿管术等[1]。随着科学技术的不断发展及手术技术的不断提高,腹腔镜及机器人辅助腹腔镜手术已经成为泌尿外科手术的主流选择。机器人辅助腹腔镜手术由于可以提供三维立体视野、利于精细腔内操作、符合人体工程学特点、学习曲线短等优势,逐步在多中心开展[2]。现对自2018年11月起由单一术者完成的108例机器人辅助腹腔镜上尿路修复手术进行总结回顾,描述手术操作技术,并报道初步结果。
1 资料与方法
1.1 临床资料
从北京大学泌尿外科研究所牵头的多中心RECUTTER(Reconstruction of Urinary Tract: Technology, Epidemiology and Result)数据库(
1.2 手术方式
对于上、中段输尿管手术,患者采取健侧45°~70°折刀斜卧位。常规消毒铺巾后,取患侧锁骨中线肋缘下1 cm小切口,置入气腹针并建立气腹至14 mmHg,于腹直肌外侧缘距气腹针约10 cm处取小切口,穿刺12 mm套管并引入机器人摄像系统。直视下分别于腋前线、锁骨中线距套管约10 cm处取2个小切口,于气腹针、腋前线、锁骨中线分别引入3个8 mm套管及机器人操作臂。根据术者需要引入1~2个助手辅助套管[4]。
对于下段输尿管手术,患者采取头低脚高截石位,于脐上5 cm做小切口,置入气腹针,建立气腹至14 mmHg,穿刺12 mm套管并引入机器人摄像系统。脐水平左右旁开约8 cm做小切口引入8 mm套管及机器人操作臂,脐下1 cm左右旁开约12 cm做小切口,患侧引入8 mm套管及机器人操作臂,健侧引入12 mm套管作为助手辅助套管。
1.2.1 改良后离断肾盂成形术 主要应用于肾盂-输尿管连接部梗阻(ureteropelvic junction obstruction,UPJO)的患者。暴露扩张的肾盂及输尿管后,于肾盂-输尿管连接部上方做一斜行2~4 cm切口,在梗阻部位以下的输尿管做横行部分切口及前壁纵行2 cm切口,保持肾盂-输尿管连接部部分连接。于肾盂及输尿管切口最低点缝合第一针后,再将连接部及梗阻段裁除,然后连续吻合后壁,置入支架管后连续吻合前壁完成缝合[5]。
图1
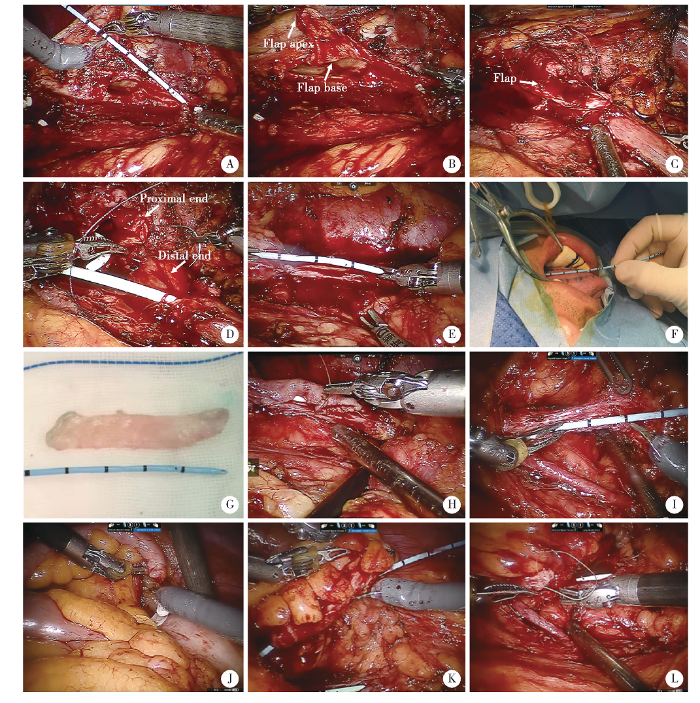
图1
肾盂瓣成形术(A~D)、舌黏膜补片修补术(E~H)及阑尾补片修补术(I~L)关键手术步骤
Figure 1
Key steps of spiral flap pyeloplasty (A-D), lingual mucosal onlay graft ureteroplasty (E-H) and appendiceal onlay flap ureteroplasty (I-L)
A, measurement of defect gap by scaled stent; B, spiral flap with 3 ∶1 ratio of length to width; C, first stitch between apex and lowest corner of ureterotomy; D, augmented anastomosis; E, measurement of defect gap by scaled DJ stent; F, mark on the ventral surface of the tongue; G, the harvested graft; H, anastomosis between lingual mucosal graft and ureter in an only fashion; I, measurement of defect gap by scaled DJ stent; J, transection of appendix from base and preservation of the mesoappendix; K, detubularization along the antimesenteric border; L, anastomosis between appendiceal graft and ureter in an only fashion.
1.2.3 输尿管狭窄段切除再吻合术 主要应用于中、上段输尿管短狭窄(<2 cm)或术中探查发现可行无张力端端吻合的病例。辨认狭窄段输尿管后,分别在狭窄段上缘及下缘部分横行切开输尿管,保持狭窄段与正常输尿管之间部分连接。在远端切口处做一长约0.5~1.0 cm纵行切口,第一针缝合于近端横行切口及远端纵行切口最低点之间,然后将狭窄段完全切除并依次吻合输尿管后壁及前壁[6]。
1.2.4 输尿管狭窄切开舌黏膜补片修补及阑尾补片修补术 主要应用于中、上段输尿管长狭窄(>2 cm)的病例。舌黏膜补片修补术:术中精确测量狭窄长度(图1E),将舌头拉出口腔后于舌侧面标记裁剪区域(图1F),并于局部黏膜下注射去甲肾上腺素及利多卡因混合液,取下带有黏膜下肌层的舌黏膜补片(图1G),并将取材区域使用3-0可吸收缝线缝合。而后将舌黏膜覆盖于纵行输尿管切口上,于两边缘行连续吻合(图1H)。阑尾补片修补术:精确测量狭窄长度(图1I),在根部离断阑尾的同时保留阑尾系膜(图1J),沿对系膜缘切开阑尾形成阑尾补片(图1K),将阑尾补片覆盖于纵行输尿管切口上,于两边缘行连续吻合(图1L)[4]。对于输尿管管腔未完全闭锁的病例,仅纵行剖开狭窄段,而对于输尿管管腔完全闭锁或狭窄段完全失活的病例,则将闭锁段完全切除后先行后壁重建缝合,再将舌黏膜或阑尾补片覆盖于前壁进行吻合。
1.2.5 输尿管膀胱再植术 主要应用于下段输尿管狭窄的病例,均采用Lich-Gregoir术式。于膀胱侧后壁做约3~4 cm的切口,切开膀胱肌层至黏膜下层,并向两侧潜行分离暴露膀胱黏膜,距输尿管末端2~3 cm处将输尿管浆肌层缝合固定于膀胱切口近端浆肌层,膀胱黏膜与输尿管全层间断吻合,间断缝合切开的膀胱肌层做黏膜下隧道。根据缺损长度及吻合张力,可酌情将膀胱使用2-0可吸收线间断缝合于腰大肌上。
图2
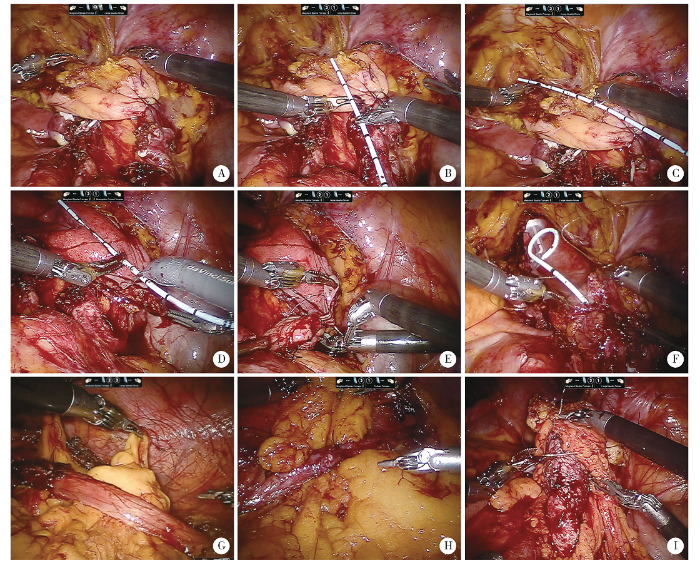
图2
膀胱悬吊翻瓣术关键手术步骤(A~F)及大网膜包裹技术应用(G~I)
Figure 2
Key steps of Boari flap-Psoas hitch (A-F) and omental wrap (G-I)
A, psoas hitch; B, measurement of defect gap by scaled DJ stent; C, predesign of Boari flap; D, Boari flap with 3 ∶1 ratio of length to width; E, anastomosis between apex and ureter; F, running sutures of the anterior wall of bladder; G, omental wrap in flap pyeloplasty; H, omental wrap in urete-roureterostomy; I, omental wrap in Boari flap.
1.2.7 体外肠管构建的回肠代输尿管术 主要应用于输尿管长段狭窄、多发狭窄且无法应用上述手术方式进行修补的病例。于机器人平台下完成输尿管游离及狭窄段切除,测量缺损长度后,断开机器人手术系统,将患者体位调为水平卧位。开腹完成体外肠道构建:绕脐做约5 cm小切口,距回盲瓣约20 cm取合适长度回肠并于近端及远端离断,然后将所取肠管的两端系膜平行于肠管切开约3 cm,以减少肠管弧度。使用稀碘伏水充分冲洗所取肠管,顺肠管蠕动方向,于远端使用3-0可吸收线外翻缝合,构建乳头,内置入输尿管支架管并以可吸收线固定于肠腔内[7]。然后重新对接机器人系统,完成肾盂代输尿管吻合及膀胱代输尿管吻合。
1.2.8 大网膜包裹 各种修复手术最后均进行大网膜包裹,即将大网膜拉至修补处并包绕输尿管或吻合口关键部位,同时将大网膜固定于腰大肌上,以加强吻合口血供、防止输尿管周围粘连(图2G、H、I)。
1.2.9 修复原则 所有修复手术均遵循“4TB”原则,即无张力(tension-free)及不漏水(watertight)的吻合、细线吻合(thin suture)、不夹持关键吻合区域(no touch of the key area)、保护血供(protecting blood supply)[8]。
1.3 观察指标
收集所有患者的术前基本信息,包括年龄、性别、患侧、狭窄位置及长度;围术期信息,包括手术方式、手术时间、术中出血量、术后住院日、围术期并发症发生情况。术后3个月、6个月患者完善泌尿系超声及肾功能检测,之后每半年一次。对患者进行门诊及电话随访,记录患者主观症状和检查结果,并与术前资料进行对比。手术成功的标准为:患者主观症状缓解或消失;泌尿系超声提示肾积水缓解或消失;肾功能有所改善或维持稳定。症状不缓解甚至加重,或影像学提示积水加重被视为手术失败。无论任何原因,如需再次留置输尿管支架管或行二次手术治疗,也被判定为手术失败。
2 结果
表1 患者临床资料
Table 1
| Items | MDP (n=53) | SFP (n=11) | UUT (n=11) | LMU (n=5) |
|---|---|---|---|---|
| Age/years, median (range) | 30 (15-64) | 29 (19-42) | 35 (17-54) | 37 (25-45) |
| Gender (Male/Female), n | 30/23 | 7/4 | 6/5 | 3/2 |
| Surgical side (Left/Right), n | 24/29 | 7/4 | 6/5 | 5/0 |
| Preoperative eGFR/[mL/(min·1.73 m2)], median (range) | 104.5 (59.7-130.5) | 118.3 (84.1-136.0) | 104.6 (60.8-118.0) | 79.0 (61.0-128.0) |
| Preoperative degree of hydronephrosis (Mild/Moderate/Severe/Nephrostomy or DJ stent), n | 12/16/18/7 | 1/2/6/2 | 1/1/4/5 | 0/0/0/5 |
| Items | AU (n=4) | UR (n=11) | BP (n=6) | IUR (n=7) |
| Age/years, median (range) | 38 (36-41) | 38 (18-65) | 52.5 (29-67) | 48 (30-53) |
| Gender (Male/Female), n | 3/1 | 2/9 | 0/6 | 5/2 |
| Surgical side (Left/Right), n | 0/4 | 5/6 | 1/5 | 3/4 |
| Preoperative eGFR/[mL/(min·1.73 m2)], median (range) | 100.6 (90.6-103.0) | 99.3 (63.1-112.8) | 77.1 (64.6-109.0) | 74.6 (59.0-117.0) |
| Preoperative degree of hydronephrosis (Mild/Moderate/Severe/Nephrostomy or DJ stent), n | 0/0/0/4 | 5/3/1/2 | 2/1/1/2 | 1/1/0/5 |
MDP, modified dismembered pyeloplasty; SFP, spiral flap pyeloplasty; UUT, ureteroureterostomy; LMU, lingual mucosa onlay graft ureteroplasty; AU, appendiceal onlay flap ureteroplasty; UR, ureteral reimplantation; BP, Boari flap-psoas hitch; IUR, ileal ureter replacement. eGFR, estimated glomerular filtration rate.
表2 不同重建手术的围术期数据及随访数据
Table 2
| Items | MDP (n=53) | SFP (n=11) | UUT (n=11) | LMU (n=5) |
|---|---|---|---|---|
| Overall operative time/min, median (range) | 141 (74-368) | 159 (110-222) | 126 (76-160) | 204 (154-250) |
| Estimated blood loss/mL, median (range) | 20 (10-350) | 50 (20-150) | 20 (10-50) | 30 (10-100) |
| Hospital stay/d, median (range) | 4 (3-19) | 5 (3-8) | 5 (4-9) | 6 (4-7) |
| Follow-up time/months, median (range) | 8 (3-17) | 7 (4-13) | 7 (3-15) | 7 (4-9) |
| Postoperative eGFR/[mL/(min·1.73 m2)], median (range) | 105.1 (58.3-139.6) | 118.5 (89.8-130.2) | 105.8 (59.2-125.3) | 71.6 (66.7-121.4) |
| Postoperative degree of hydronephrosis (None or Mild/Moderate/Severe), n | 48/4/1 | 9/2/0 | 9/2/0 | 5/0/0 |
| Overall success rate/% | 94.3 | 100.0 | 100.0 | 100.0 |
| Items | AU (n=4) | UR (n=11) | BP (n=6) | IUR (n=7) |
| Overall operative time/min, median (range) | 164 (135-211) | 149 (100-218) | 166 (137-205) | 270 (227-335) |
| Estimated blood loss/mL, median (range) | 75 (50-200) | 20 (10-50) | 45 (20-100) | 100 (10-100) |
| Hospital stay/d, median (range) | 8.5 (6-12) | 7 (5-10) | 5 (4-41) | 7 (5-26) |
| Follow-up time/months, median (range) | 8 (4-10) | 5 (3-17) | 10 (6-12) | 9 (5-12) |
| Postoperative eGFR/[mL/(min·1.73 m2)], median (range) | 105.8 (92.1-115.0) | 101.8 (79.7-114.7) | 87.4 (63.8-104.1) | 77.1 (47.6-115.4) |
| Postoperative degree of hydronephrosis (None or Mild/Moderate/Severe), n | 4/0/0 | 11/0/0 | 6/0/0 | 6/0/1 |
| Overall success rate/% | 100.0 | 90.7 | 83.3 | 85.7 |
Abbreviations as in
应用改良后离断肾盂成形术治疗UPJO 53例,其中8例为二次成形。8例患者存在异位血管,21例合并肾结石,5例合并马蹄肾,2例合并肾下垂。中位手术时间141 min(74~368 min),中位出血量20 mL(10~350 mL),中位术后住院时间4 d(3~19 d),第一例手术患者术后近端吻合口瘘,通过调整更换输尿管支架管保守治疗后好转。中位随访时间8个月(3~17个月),94.3%(50/53)患者术后症状改善且影像学提示肾积水有所缓解。
应用改良肾盂瓣成形术治疗UPJO合并近端输尿管长狭窄11例,其中8例因既往手术治疗失败行再次手术治疗。中位输尿管狭窄长度2 cm(2~5 cm),中位手术时间159 min(110~222 min),中位出血量50 mL(20~150 mL),中位术后住院时间5 d(3~8 d)。术后不全肠梗阻1例,保守治疗后好转。中位随访时间7个月(4~13个月),所有患者均有术后症状改善且影像学提示肾积水缓解。
应用输尿管狭窄段切除再吻合术治疗上段输尿管狭窄7例、中段输尿管狭窄3例、下段输尿管狭窄1例。其中7例为腔内碎石术所致狭窄,2例为子宫内膜异位症所致狭窄,1例为输尿管息肉所致狭窄,1例为腔静脉后输尿管。中位手术时间为126 min(76~160 min),中位术中出血量为20 mL(10~50 mL),中位术后住院时间为5 d(4~9 d);中位随访时间7个月(3~15个月),所有患者术后症状改善及影像学提示肾积水改善。2例子宫内膜异位症患者中的1例接受了为期6个月的促性腺激素释放激素激动剂(gonadotropin releasing hormone agonist, GnRHa)治疗,另1例患者未接受激素治疗;2例患者均无新发疼痛且肾积水缓解良好。
应用输尿管狭窄切开自体舌黏膜补片修补术治疗上段长狭窄5例,中位狭窄长度为4.5 cm(3~5 cm),中位手术时间204 min(154~250 min),中位出血量30 mL(10~100 mL),中位术后住院时间6 d(4~7 d)。应用输尿管狭窄切开阑尾补片修复术治疗上段长狭窄3例和中段长狭窄1例,中位狭窄长度为4 cm(3.5~4.5 cm)。中位手术时间为164 min(135~211 min),中位手术出血量为50 mL(50~200 mL),中位术后住院日为8.5 d(6~12 d)。术后泌尿系感染1例,抗生素治疗后好转。中位随访时间8个月(4~10个月),所有患者术后症状消失及影像学提示积水有缓解。
应用输尿管膀胱再植术治疗先天性巨输尿管2例、输尿管阴道瘘3例、膀胱输尿管反流3例、子宫内膜异位症所致输尿管狭窄1例、手术所致下段输尿管狭窄2例。中位手术时间为149 min(100~218 min),中位术中出血量为20 mL(10~50 mL),中位术后住院日7 d(5~10 d)。术后1例患者出现腹股沟区疼痛,考虑为术中膀胱腰肌悬吊导致的生殖股神经压迫所致。中位随访时间5个月(3~17个月),90.9%(10/11)患者术后症状改善,影像学提示肾积水改善,1例患者表现为反复发作的泌尿系感染,尿培养提示肠球菌感染,需要再次留置输尿管支架管。子宫内膜异位症所致狭窄的1例患者术后未接受激素治疗,该患者无新发疼痛且肾积水缓解良好。
应用术中精确测量法膀胱悬吊翻瓣术治疗输尿管下段长段狭窄6例,其中4例为既往妇科手术损伤所致狭窄,1例为钬激光碎石所致狭窄,1例为先天性狭窄。中位手术时间166 min(137~205 min),中位手术出血45 mL(20~100 mL),中位术后住院日5 d(4~41 d)。术后1例患者因输尿管支架管下滑造成吻合口瘘,导致住院时间延长,通过调整更换输尿管支架管、延长腹腔引流时间、应用抗生素等治疗后好转。中位随访时间为10个月(6~12个月),1例患者表现为反复发作的泌尿系感染,且因术后粘连性肠梗阻行手术治疗,其余患者均有症状改善及肾积水缓解。
应用改良回肠代输尿管手术治疗长段输尿管狭窄6例及输尿管多发息肉1例,中位手术时间270 min(227~335 min),中位术中出血量100 mL(10~100 mL),中位术后住院日7 d(5~26 d)。术后伤口脂肪液化1例,在局部麻醉下清创二次缝合;该患者术后住院时间为26 d。术后发热1例,经抗生素治疗后好转。中位随访时间为9个月(5~12个月),所有患者肾功能保持稳定,动态磁共振检查提示,6例患者肠代输尿管蠕动良好,无积水或仅有轻度积水,1例患者肠代输尿管远端蠕动较差,仍有重度积水。
3 讨论
3.1 改良后离断式肾盂成形术及肾盂瓣成形术
腹腔镜及机器人辅助腹腔镜Anderson-Hynes离断式肾盂成形术成功率高,且有创伤小、操作空间大、术中出血少、术后住院日短等优势[9],逐渐成为UPJO治疗的金标准。本研究中所采用的后离断式肾盂成形术,其改良目的在于降低吻合张力,避免完全离断后输尿管扭转的发生。同时将肾盂输尿管连接部区分为钳夹区域及吻合区域,钳夹区域主要为连接部及梗阻段,均为最后切除的部分,避免过度夹持需要保留的肾盂组织而破坏血供。对于合并结石的患者可于术中使用输尿管硬镜、半硬镜或者纤维输尿管镜取石[10,11],而对于合并马蹄肾、肾下垂先天泌尿系畸形的患者术中也可同时进行相应修复。本研究中由单一术者完成的机器人肾盂成形术短期随访结果满意。
肾盂瓣成形术主要适用于肾盂积水程度较重同时合并近端输尿管长狭窄的患者。从肾盂组织取材可以避免一系列使用非尿路组织(如口腔黏膜、肠管等)进行修补导致的并发症,同时具有缩小肾盂体积、构建较宽吻合口的优点。曾有研究报道最长的修复长度可达15 cm[12],本研究中修补的最长狭窄长度为5 cm,围术期数据及短期随访结果满意。大部分患者为二次成形患者,由于既往手术瘢痕及炎症粘连,容易造成长段狭窄,因而,肾盂瓣成形是二次肾盂成形手术方式的良好选择。
3.2 输尿管狭窄段切除再吻合术
对于中、上段的输尿管短段(<2 cm)狭窄及损伤来说,输尿管狭窄段切除再吻合术因其操作技术简单往往成为首选的治疗方式[13]。Sun等[14]报道了126例输尿管狭窄段切除再吻合术,平均随访时间为30个月,65例为机器人手术,61例为普通腹腔镜手术,结果显示,在手术时间、缝合时间及术后住院日上机器人组明显优于腹腔镜组,机器人组平均手术时间为126 min,平均缝合时间为27 min,平均术后住院日为4 d。我们的改良输尿管狭窄段切除再吻合术不同于传统的技术,采用一针定位后离断切除狭窄段的方式,目的在于减小后续的吻合张力同时防止输尿管扭转。本研究中的围术期结果与既往报道相似。此外,由于术中往往难以准确辨认狭窄段及确定切除长度,有相关报道使用吲哚菁绿辅助术中辨认狭窄部位[15],使用输尿管镜辅助定位狭窄段[16],这些方式均可尝试采用以准确切除狭窄段,防止切除过多正常输尿管组织导致吻合张力过大。
3.3 输尿管狭窄切开舌黏膜补片修补及阑尾补片修补术
对于上、中段的长段输尿管狭窄及损伤来说,既往多采用肠代输尿管术及自体肾移植术来处理,但均存在一定弊端。自体肾移植术对血管要求较高,且有术后血管并发症的风险[17],而肠代输尿管术则存在肠道相关并发症、酸碱平衡紊乱及黏液阻塞代输尿管等风险[18]。口腔黏膜补片治疗输尿管狭窄的技术以颊黏膜为修补材料,随后颊黏膜补片逐渐成熟应用于上、中段长段输尿管狭窄的修复中[19],但取材后会出现口腔麻木、口腔狭窄及影响唾液腺分泌等并发症[20]。而舌黏膜补片因取材方便且口腔并发症少,逐渐被泌尿外科医师所接受,并在腹腔镜手术中取得了良好的疗效[21]。本研究中接受舌黏膜补片修补术的患者术后舌创面恢复良好且狭窄修补效果良好,证实了在机器人平台中使用该技术是一种治疗上、中段输尿管长狭窄的安全有效方式。对于右侧的上、中段输尿管长狭窄来说,阑尾补片技术同样是一种值得选择的方式,阑尾系膜血供的保留更有利于吻合口愈合。Duty等[22]报道了6例腹腔镜阑尾补片修复术,平均手术时间为244 min,平均术中出血量为175 mL,平均术后住院日为3.2 d,梗阻客观缓解率为100%。根据术者长期经验总结,我们认为对于阑尾条件良好、阑尾长度合适的右侧上、中段输尿管长狭窄患者来说,可选择进行阑尾补片修补术,而对于阑尾条件差以及左侧输尿管狭窄患者来说,则可选用舌黏膜补片术进行输尿管狭窄修补。
3.4 输尿管膀胱再植术及膀胱悬吊翻瓣术
针对输尿管下段狭窄,可根据狭窄长度酌情选用输尿管膀胱再植术及膀胱悬吊翻瓣术。Lich-Gregoir法,即黏膜下隧道法,是最常用的再植方式,其抗反流效果肯定,成功率较高[23]。本研究证实了该术式在机器人平台下的可行性及有效性。腰肌悬吊及膀胱翻瓣技术可实现对长段狭窄的修补,既往报道对于 5~8 cm的损伤可采用腰肌悬吊术[24],而更长的病变则需联合膀胱翻瓣技术。本研究中采用长宽比约3 ∶1的膀胱瓣,目的在于保证良好的血供,同时使用带刻度的导管精确测量缺损长度,有利于充分利用膀胱组织、降低吻合张力、避免剩余膀胱体积过小。对于输尿管长段狭窄来说,可以将膀胱瓣术与肠代输尿管术联合应用[25],能够大大缩短所需肠管长度,降低术后肠道及代谢相关并发症。
3.5 改良回肠代输尿管术
肠代输尿管术被认为是输尿管狭窄修复的最后手段,适用于输尿管长段乃至全长狭窄的修补,其中回肠使用最多。开放肠代输尿管术和腹腔镜肠代输尿管术已被证实具有良好的成功率[17, 26]。有学者探索了机器人肠代输尿管术的应用,但多为个案报道,Ubrig等[27]报道了7例全腔内机器人肠代输尿管手术,平均手术时间328 min,中位术中出血100 mL,在3个月的随访中,所有患者均获得了良好的功能学结果。本研究采用体外肠管构建的机器人肠代输尿管手术,体外肠管构建能够更准确地测量及裁取所需肠管,降低肠道相关并发症的发生率,同时体外肠管构建避免了腹腔内感染的风险,也降低了手术操作难度;机器人平台下的精细操作利于腔内吻合。虽然需要在手术过程中反复断开及对接机器人系统,但由于体外操作的便捷性,反而缩短了总手术时长,与既往报道相比有着更短的手术时间。同时腹部5 cm小切口并不显著延长术后恢复时间。此外,我们认为代输尿管近端可直接与肾盂或输尿管吻合,远端应进行抗反流设计,乳头法操作简单,可作为首选方式。
综上所述,本研究报道了单一术者完成的108例机器人辅助腹腔镜上尿路修复手术,涉及到复杂多样的病因、较全面的狭窄情况及丰富的手术方式,对进一步形成标准化、简单化、实用化、个体化机器人上尿路修复手术提供了借鉴经验,但仍需长期随访数据及更大样本的研究。
参考文献
Ureteric reconstruction
[J].
Robotic reconstruction of the upper urinary tract
[J].
Appendiceal onlay flap ure-teroplasty for the treatment of complex ureteral strictures: Initial experience of nine patients
[J/OL].
A modified suture technique for transperitoneal laparoscopic dismembered pyeloplasty of pelviureteric junction obstruction
[J].
Modified laparoscopic partial urete-rectomy for adult ureteral fibroepithelial polyp: Technique and initial experience
[J].
Technical considerations and outcomes for ileal ureter replacement: a retrospective study in China
[J].
Robot-assisted and laparoscopic repair of ureteropelvic junction obstruction: a syste-matic review and meta-analysis
[J].
DOI:10.1016/j.eururo.2013.06.053
URL
PMID:23856037
[本文引用: 1]

CONTEXT: Over the last two decades, minimally invasive treatment options for ureteropelvic junction obstruction (UPJO) have been developed and popularized. OBJECTIVE: To critically analyze the current status of laparoscopic and robotic repair of UPJO. EVIDENCE ACQUISITION: A systematic literature review was performed in November 2012 using PubMed. Article selection proceeded according to the search strategy based on Preferred Reporting Items for Systematic Reviews and Meta-analyses criteria. EVIDENCE SYNTHESIS: Multiple series of laparoscopic pyeloplasty have demonstrated high success rates and low perioperative morbidity in pediatric and adult populations, with both the transperitoneal and retroperitoneal approaches. Data on pediatric robot-assisted pyeloplasty are increasingly becoming available. A larger number of cases have also been reported for adult patients, confirming that robotic pyeloplasty represents a viable option for either primary or secondary repair. Robot-assisted redo pyeloplasty has been mostly described in the pediatric population. Different technical variations have been implemented with the aim of tailoring the procedure to each specific case. The type of stenting, retrograde versus antegrade, continues to be debated. Internal-external stenting as well as a stentless approach have been used, especially in the pediatric population. Comparative studies demonstrate similar success and complication rates between minimally invasive and open pyeloplasty in both the adult and pediatric setting. A clear advantage in terms of hospital stay for minimally invasive over open pyeloplasty was observed only in the adult population. CONCLUSIONS: Laparoscopy represents an efficient and effective less invasive alternative to open pyeloplasty. Robotic pyeloplasty is likely to emerge as the new minimally invasive standard of care whenever robotic technology is available because its precise suturing and shorter learning curve represent unique attractive features. For both laparoscopy and robotics, the technique can be tailored to the specific case according to intraoperative findings and personal surgical experience.
A simple modification for the usage of flexible cystoscope in modified laparoscopic pyeloplasty for ure-teropelvic junction obstruction with renal calculi: A flexible guiding tube
[J].
Management for ureteral stenosis: A comparison of robot-assisted laparoscopic ureteroureterostomy and conventional laparoscopic ureteroureterostomy
[J].
Novel use of indocyanine green for intraoperative, real-time localization of ureteral stenosis during robot-assisted ureteroureterostomy
[J].
Laparoendoscopic single-site ureteroureterostomy with intraoperative retrograde ureteroscopy-assisted technique for benign proximal and middle ureteral strictures: A single-center experience
[J].
Long-term outcomes and late complications of laparoscopic nephrectomy with renal autotransplantation
[J].
Long-term results of ileal ureteric replacement: A 25-year single-centre experience
[J].
Robotic ureteral reconstruction using buccal mucosa grafts: A multi-institutional expe-rience
[J].
DOI:10.1016/j.eururo.2017.11.015
URL
PMID:29239749
[本文引用: 1]
BACKGROUND: Minimally invasive treatment of long, multifocal ureteral strictures or failed pyeloplasty is challenging. Robot-assisted buccal mucosa graft ureteroplasty (RBU) is a technique for ureteral reconstruction that avoids the morbidity of bowel interposition or autotransplantation. OBJECTIVE: To evaluate outcomes for RBU in a multi-institutional cohort of patients treated for revision ureteropelvic junction obstruction and long or multifocal ureteral stricture at three tertiary referral centers. DESIGN, SETTING, AND PARTICIPANTS: This retrospective study involved data for 19 patients treated with RBU at three high-volume centers between October 2013 and July 2016. SURGICAL PROCEDURE: RBU was performed using either an onlay graft after incising the stricture or an augmented anastomotic repair in which the ureter was transected and re-anastomosed primarily on one side, and a graft was placed on the other side. OUTCOME MEASUREMENTS AND STATISTICAL ANALYSIS: Preoperative, intraoperative, and postoperative variables and outcomes were assessed. A descriptive statistical analysis was performed. RESULTS AND LIMITATIONS: The onlay technique was used for 79%, while repair was carried out using the augmented anastomotic technique for the remaining cases. The reconstruction was reinforced with omentum in 95% of cases. The ureteral stricture location was proximal in 74% and mid in 26% of cases. A prior failed ureteral reconstruction was present in 53% of patients. The median stricture length was 4.0cm (range 2.0-8.0), operative time was 200min (range 136-397), estimated blood loss was 95ml (range 25-420), and length of stay was 2 d (range 1-15). There were no intraoperative complications. At median follow-up of 26 mo, the overall success rate was 90%. CONCLUSIONS: RBU is a feasible and effective technique for managing complex proximal and mid ureteral strictures. PATIENT SUMMARY: We studied robotic surgery for long ureteral strictures using grafts at three referral centers. Our results demonstrate that robotic buccal mucosa graft ureteroplasty is a feasible and effective technique for ureteral reconstruction.
Oral complications after buccal mucosal graft harvest for urethroplasty
[J].
Laparoscopic onlay lingual mucosal graft ureteroplasty for proximal ureteral stricture: initial experience and 9-month follow-up
[J].
DOI:10.1007/s11255-016-1289-9
URL
PMID:27115158
[本文引用: 1]
PURPOSE: We present our initial experience and 9-month outcomes of the novel technique of laparoscopic onlay lingual mucosal graft ureteroplasty for proximal ureteral stricture. MATERIALS AND METHODS: In June 2015, transperitoneal laparoscopic onlay lingual mucosal graft ureteroplasty was performed on a male patient with proximal stricture of the left ureter. The patient complained with left frank pain. Severe hydronephrosis and proximal ureteral dilatation were noted through ultrasonography and CT scan. The length of upper ureteral stricture was 30 mm including 10-mm occlusion. A 46 mm in length and 15 mm in width lingual mucosa graft was harvested from the ventral of the tongue and placed in the strictured ureter as a ventral onlay for laparoscopic ureteroplasty. Operative time, intraoperative, and postoperative complications were well recorded. Follow-up was performed with renal ultrasound, CT scan, and nuclear scan renography as well as clinical assessment of symptoms. RESULTS: The new technique was performed successful without intraoperative and postoperative complications. Neither hydronephrosis nor proximal ureteral dilatation in the left side was found through ultrasonography 3, 6, 9 months and CT scan 6 month postoperatively. The left renal function, glomerular filtration rate, had a recovery from 9.6 ml/min preoperatively to 14.0 ml/min at 6-month follow-up, and the patient has no complaints about the donor site and flank pain. CONCLUSIONS: To our knowledge, we present the initial experience with laparoscopic onlay lingual mucosal graft ureteroplasty for proximal ureteral stricture. With 9-month outcomes, the new technique appears to be an excellent option for proximal ureteral stricture.
Review of appendiceal onlay flap in the management of complex ureteric strictures in six patients
[J].
Psoas hitch and Boari flap ureteroneocystostomy
[J].
Ileal ureter replacement combined with Boari flap-Psoas hitch to treat full-length ureteral defects: Technique and initial experience
[J].
Laparoscopic assisted ileal ureter: technique, outcomes and comparison to the open procedure
[J].
DOI:10.1016/j.juro.2009.05.013
URL
PMID:19616806
[本文引用: 1]
PURPOSE: Ureteral replacement with interposition of a bowel segment has traditionally required a large incision with substantial associated morbidity and prolonged time to convalescence. During the last 7 years a technique for laparoscopic assisted ileal interposition has evolved that mimics our open approach. We present a comparative analysis of functional and perioperative outcomes between patients undergoing laparoscopic or open ileal ureter replacement at our institution. MATERIALS AND METHODS: A search of all procedures from 1980 to the present revealed 7 patients undergoing laparoscopic and 7 undergoing open ileal interposition. Functional and perioperative data from these patients are compared, and a detailed description of technique for the laparoscopic procedure is presented. RESULTS: Narcotic analgesic use in morphine equivalents (median 38.9 vs 322.2 mg, p = 0.035) and time to convalescence (median 4 vs 5.5 weeks, p = 0.03) were significantly less in the laparoscopic group. A trend toward shorter hospital stay (median 5 vs 8 days, p = 0.101) was also noted in patients in the laparoscopic group. There was no evidence of anastomotic stricture for patients in either group at last followup. CONCLUSIONS: Despite the small number of subjects involved a significant advantage was noted for postoperative recovery after laparoscopic compared to open ileal interposition. A detailed understanding of this complicated procedure can help prevent inherent pitfalls.
Functional outcome of completely intracorporeal robotic ileal ureteric replacement
[J].


{kind=link}
{kind=link}
{kind=link}
{kind=link}