北京大学学报(医学版) ›› 2023, Vol. 55 ›› Issue (1): 160-166. doi: 10.19723/j.issn.1671-167X.2023.01.025
腓骨肌萎缩症1A型患者和慢性炎性脱髓鞘性多发性神经病患者F波改变的比较
刘小璇,张朔,马妍,孙阿萍,张英爽,樊东升*( )
)
- 北京大学第三医院神经内科,北京 100191
Diagnostic value of F wave changes in patients with Charcot-Marie-Tooth1A and chronic inflammatory demyelinating polyneuropathy
Xiao-xuan LIU,Shuo ZHANG,Yan MA,A-ping SUN,Ying-shuang ZHANG,Dong-sheng FAN*()
- Department of Neurology, Peking University Third Hospital, Beijing 100191, China
摘要:
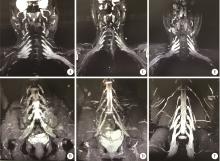
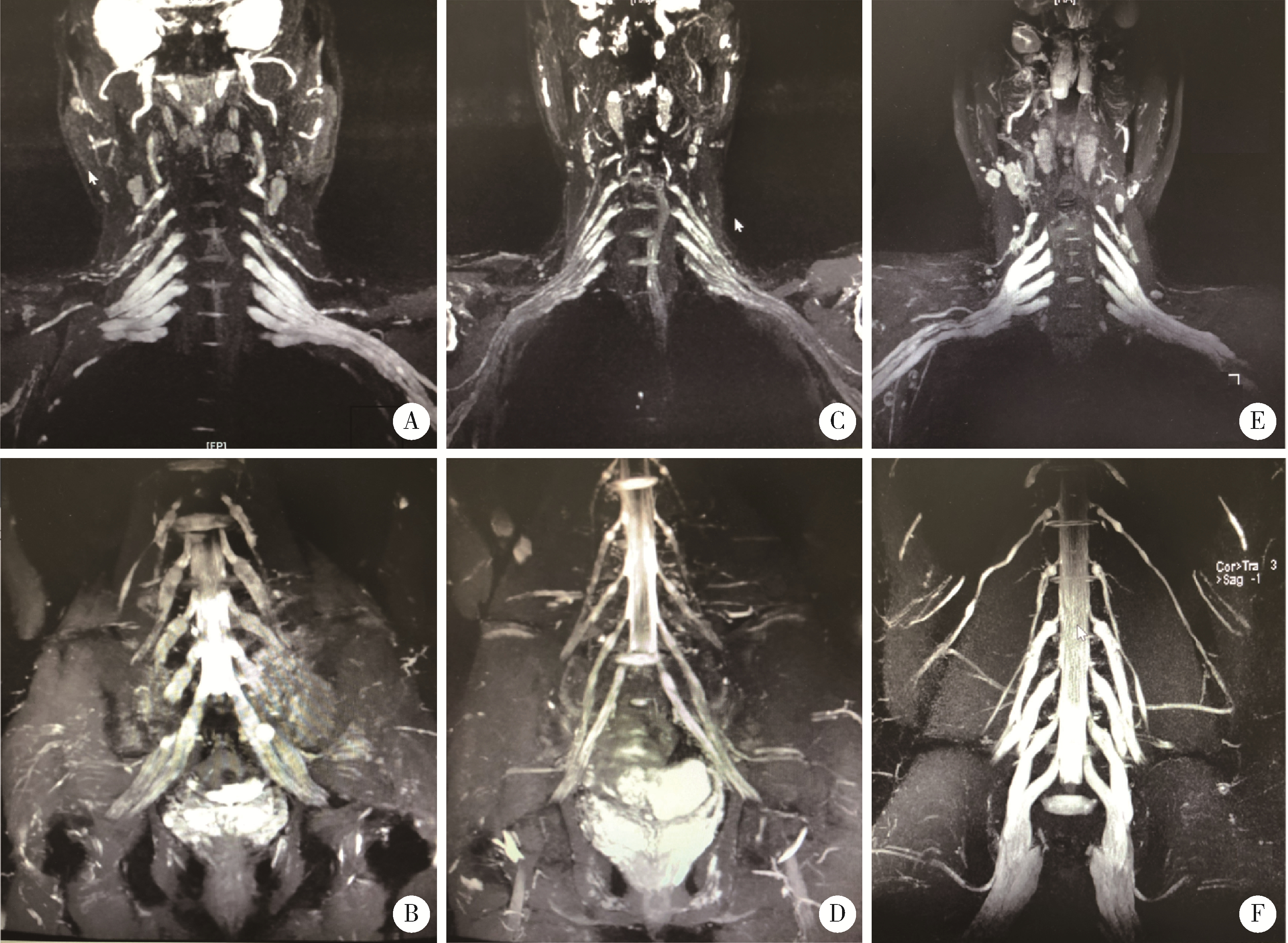
目的: 分析比较腓骨肌萎缩症1A型(Charcot-Marie-Tooth1A,CMT1A)患者和慢性炎性脱髓鞘性多发性神经病(chronic inflammatory demyelinating polyneuropathy, CIDP)患者F波改变的特点和原因。方法: 收集自2012年1月到2018年12月在北京大学第三医院诊治的CMT1A和CIDP患者各30例,记录临床资料、电生理指标(神经传导速度和F波、H反射)、神经功能等级评分等,部分患者行臂丛和腰丛的磁共振影像检查,分析比较结果。结果: CMT1A患者的正中神经平均运动传导速度为(21.10±10.60) m/s, CIDP患者为(31.52±12.46)m/s, 二者差异有统计学意义(t=-6.75, P < 0.001),CMT1A患者中约43.3%(13/30)未引出尺神经F波,明显高于CIDP未引出F波的患者比例(4/30,13.3%),χ2=6.65,P=0.010。在可引出F波的患者中,CMT1A组患者的F波潜伏期为(52.40±17.56) ms,CIDP组为(42.20± 12.73) ms, 二者差异有统计学意义(t=2.96, P=0.006),F波的出现率CMT1A组是34.6%±39%,CIDP组是70.7%±15.2%,二者差异有统计学意义(t=-5.13, P < 0.001)。神经束蛋白155(neurofascin 155, NF155)患者的正中神经传导速度为23.22 m/s, F波潜伏期为62.9~70.7 ms,出现率为85%~95%。CMT1A型臂丛和腰丛神经增粗的比例分别为83.3%(5/6)和85.7%(6/7),CIDP患者臂丛和腰丛神经增粗的比例仅为25.0%(1/4,2/8)。NF155抗体阳性患者可见臂丛和腰丛MRI神经根明显增粗。结论: CMT1A患者F波延长反应了近端和远端周围神经的均一性改变,可以作为与局灶性脱髓鞘受损为主的CIDP患者的鉴别方法,但同时需要注意与神经结蛋白病NF155引起的周围神经损害相鉴别。F波虽然经常作为反应近端神经受累的指标,但是运动神经元兴奋性、前角细胞和运动神经髓鞘病变均可以影响它的潜伏期和出现率,F波异常需要结合患者的病因和其他电生理指标及影像学等检查手段综合分析。
中图分类号:
- R745.4
| 1 |
Rossor AM , Polke JM , Houlden H , et al. Clinical implications of genetic advances in Charcot-Marie-Tooth disease[J]. Nat Rev Neurol, 2013, 9 (10): 562- 571.
doi: 10.1038/nrneurol.2013.179 |
| 2 | Davis CJ , Bradley WG , Madrid R . The peroneal muscular atrophy syndrome: Clinical, genetic, electrophysiological and nerve biopsy studies. Ⅰ. Clinical, genetic and electrophysiological findings and classification[J]. J Genet Hum, 1978, 26 (4): 311- 349. |
| 3 |
刘小璇, 樊东升, 宋淑娟. 中国人群腓骨肌萎缩症的致病基因分布特点及临床表型[J]. 中华内科杂志, 2015, 54 (7): 623- 627.
doi: 10.3760/cma.j.issn.0578-1426.2015.07.011 |
| 4 |
van den Bergh PY , Hadden RD , Bouche P , et al. European Fe-deration of Neurological Societies/Peripheral Nerve Society Guideline on management of chronic inflammatory demyelinating polyradiculoneuropathy: Report of a joint task force of the European Fe-deration of Neurological Societies and the Peripheral Nerve Society: First revision[J]. Eur J Neurol, 2010, 17 (3): 356- 363.
doi: 10.1111/j.1468-1331.2009.02930.x |
| 5 |
马妍, 鲁明, 樊东升, 等. 无力麻木-周围神经损害-抗NF155 IgG4抗体阳性[J]. 中华医学杂志, 2016, 96 (43): 3519- 3543.
doi: 10.3760/cma.j.issn.0376-2491.2016.43.017 |
| 6 |
马妍, 鲁明, 樊东升. 抗NF155 IgG抗体阳性慢性炎性脱髓鞘性多发性神经根一例并文献复习[J]. 中国神经免疫学和神经病学杂志, 2017, 24 (3): 188- 196.
doi: 10.3969/j.issn.1006-2963.2017.03.009 |
| 7 |
马妍, 鲁明, 樊东升. 郎飞结/结旁疾病慢性炎性脱髓鞘性多发性神经根相关抗体的研究进展[J]. 中华神经科杂志, 2017, 50 (10): 778- 780.
doi: 10.3760/cma.j.issn.1006-7876.2017.10.016 |
| 8 |
Ogata H , Yamasaki R , Hiwatashi A , et al. Characterization of IgG4 anti-neurofascin 155 antibody-positive polyneuropathy[J]. Ann Clin Transl Neurol, 2015, 2 (10): 960- 971.
doi: 10.1002/acn3.248 |
| 9 |
Querol L , Nogales-Gadea G , Rojas-Garcia R , et al. Neurofascin IgG4 antibodies in CIDP associate with disabling tremor and poor response to IVIg[J]. Neurology, 2014, 82 (10): 879- 886.
doi: 10.1212/WNL.0000000000000205 |
| 10 |
Devaux JJ , Miura Y , Fukami Y , et al. Neurofascin-155 IgG4 in chronic inflammatory demyelinating polyneuropathy[J]. Neurology, 2016, 86 (9): 800- 807.
doi: 10.1212/WNL.0000000000002418 |
| 11 |
Niu J , Cui L , Liu M , et al. Multiple sites ultrasonography of peripheral nerves in differentiating Charcot-Marie-Tooth Type 1A from chronic inflammatory demyelinating polyradiculoneuropathy[J]. Front Neurol, 2017, 8, 181.
doi: 10.3389/fneur.2017.00181 |
| 12 |
Vaeggemose M , Vaeth S , Pham M , et al. Magnetic resonance reurography and diffusion tensor imaging of the peripheral nerves in patients with CMT Type 1A[J]. Muscle Nerve, 2017, 56 (6): E78- E84.
doi: 10.1002/mus.25691 |
| 13 |
中华医学会神经病学分会, 中华医学会神经病学分会周围神经病协作组, 中华医学会神经病学分会肌电图与临床神经电生理学组, 中华医学会神经病学分会神经肌肉病学组. 中国慢性炎症性脱髓鞘性多发性神经根神经病诊治指南[J]. 中华神经科杂志, 2019, 52 (11): 883- 888.
doi: 10.3760/cma.j.issn.1006-7876.2019.11.003 |
| 14 |
Pefla L , Moreno CB , Gutierrez-Alvarez AM . Pain management in Guillain-Barre syndrome: A systematic review[J]. Neurologia, 2015, 30 (7): 433- 438.
doi: 10.1016/j.nrl.2014.04.009 |
| 15 | 汤晓芙. 临床肌电图学[M]. 北京: 北京医科大学/中国协和医科大学联合出版社, 1995: 51- 59. |
| 16 | 卢祖能. 实用肌电图学[M]. 北京: 人民卫生出版社, 2000: 851- 853. |
| 17 | Wang ZL , Liu M , Ding Q . Split-hand index in amyotrophic lateral sclerosis: An F-wave study[J]. Amyotroph Lateral Scler Frontotemporal Degener, 2019, 20 (7/8): 562- 567. |
| 18 |
Baek SH , Hong YH , Choi SJ , et al. Electrodiagnostic data-driven clustering identifies a prognostically different subgroup of patients with chronic inflammatory demyelinating polyneuropathy[J]. J Neurol Neurosurg Psychiatry, 2019, 90 (6): 674- 680.
doi: 10.1136/jnnp-2018-319758 |
| 19 |
van den Bergh PYK , van Doorn PA , et al. European Academy of Neurology/Peripheral Nerve Society Guideline on diagnosis and treatment of chronic inflammatory demyelinating polyradiculoneuropathy: Report of a joint task force-second revision[J]. Eur J Neurol, 2021, 28 (11): 3556- 3583.
doi: 10.1111/ene.14959 |
| 20 | Martín-Aguilar L , Lleixà C , Pascual-Goñi E , et al. Clinical and laboratory features in anti-NF155 autoimmune nodopathy[J]. Neurol Neuroimmunol Neuroinflamm, 2021, 9 (1): e1098. |
| 21 |
Chhabra A , Madhuranthakam AJ , Andreisek G . Magnetic resonance neurography: Current perspectives and literature review[J]. Eur Radiol, 2018, 28 (2): 698- 707.
doi: 10.1007/s00330-017-4976-8 |
| 22 |
Kronlage M , Pitarokoili K , Schwarz D , et al. Diffusion tensor imaging in chronic inflammatory demyelinating polyneuropathy: Diagnostic accuracy and correlation with electrophysiology[J]. Invest Radiol, 2017, 52 (11): 701- 707.
doi: 10.1097/RLI.0000000000000394 |
| 23 |
Doppler K , Stengel H , Appeltshauser L , et al. Neurofascin-155 IgM autoantibodies in patients with inflammatory neuropathies[J]. J Neurol Neurosurg Psychiatry, 2018, 89 (11): 1145- 1151.
doi: 10.1136/jnnp-2018-318170 |
| 24 | Wu F , Ren Y , Wang WW , et al. Microstructural alteration of lumbosacral nerve roots in chronic inflammatory demyelinating polyradiculoneuropathy: Insights from DTI and correlations with electrophysiological parameters[J]. Acad Radiol, 2022, 29 (Suppl 3): 175- 182. |
| [1] | 林国中,王振宇,谢京城,刘彬,马长城,陈晓东. 内含终丝的骶管囊肿21例临床研究[J]. 北京大学学报(医学版), 2020, 52(3): 582-585. |
| [2] | 樊东升, 张俊, 邓敏, 康德瑄, 郑菊阳, 徐迎胜, 鲁明, 傅瑜, 沈扬, 张英爽, 张华纲. 肌萎缩侧索硬化/运动神经元病的基础与临床研究[J]. 北京大学学报(医学版), 2009, 41(3): 279-281. |
| [3] | 杨朝晖, 彭歆, 谢秋菲. 面神经离断损伤神经电图诊断评价[J]. 北京大学学报(医学版), 2008, 40(6): 639-641. |
| [4] | 周崇阳, 杨朝晖, 冯海兰. 咬合重建对咀嚼肌肌电图协同模式的近、远期影响[J]. 北京大学学报(医学版), 2008, 40(3): 323-326. |
| [5] | 刘小璇, 樊东升, 张俊, 郑菊阳, 马铁民. 比较不同方式移植的人间充质干细胞在大鼠失神经支配的骨骼肌的分布及对坐骨神经损伤的影响[J]. 北京大学学报(医学版), 2008, 40(2): 185-191. |
| [6] | 张如旭, 罗巍, 资晓宏, 夏昆, 蔡芳, 萧剑峰, 赵国华, 张付峰, 沈潞, 江泓, 唐北沙. 中国汉族人群腓骨肌萎缩症Cx32基因突变分析[J]. 北京大学学报(医学版), 2005, 37(1): 68-71. |
| [7] | 章远志, Nanbert Zhong. 腓骨肌萎缩症的分子遗传学研究[J]. 北京大学学报(医学版), 2005, 37(1): 100-105. |
| Viewed | ||||||||||||||||||||||||||||||||||||||||||||||||||
|
Full text 171
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
Abstract 518
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
Cited |
|
|||||||||||||||||||||||||||||||||||||||||||||||||
| Shared | ||||||||||||||||||||||||||||||||||||||||||||||||||
| Discussed | ||||||||||||||||||||||||||||||||||||||||||||||||||
|
||
