北京大学学报(医学版) ›› 2026, Vol. 58 ›› Issue (3): 496-502. doi: 10.19723/j.issn.1671-167X.2026.03.008
2000—2021年全球204个国家直接与间接孕产妇死亡联合轨迹及演变特征
周一, 程钊, 冯星淋*( )
)
- 北京大学公共卫生学院卫生政策与管理学系, 北京 100191
Joint trajectories and evolution patterns of direct and indirect maternal mortality across 204 countries from 2000 to 2021
Yi ZHOU, Zhao CHENG, Xinglin FENG*()
- Department of Health Policy and Management, Peking University School of Public Health, Beijing 100191, China
摘要:
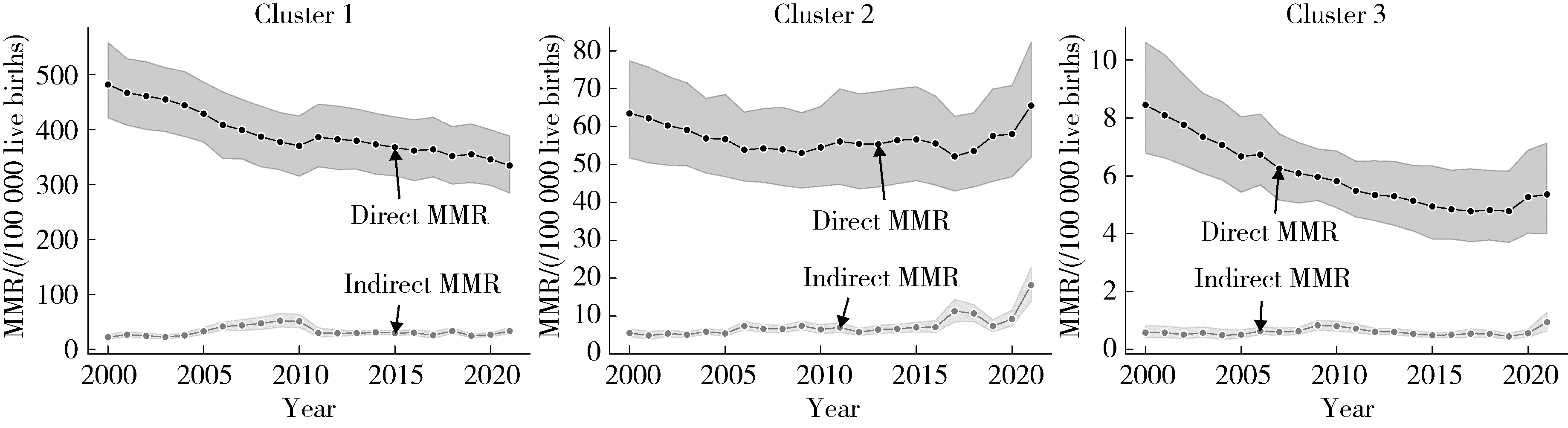
目的: 以直接与间接孕产妇死亡率(maternal mortality ratio,MMR)为联合结局,识别2000—2021年全球国家层面联合轨迹类型,并比较不同轨迹类型在跨千年发展目标期间(millennium development goals,MDG,2000—2015年)与可持续发展目标(sustainable development goals,SDG,2015—2021年)阶段变化特征及其卫生系统与制度环境差异。方法: 基于全球疾病负担(Global Burden Disease, GBD)研究数据库,纳入2000—2021年全球204个国家和地区15~49岁育龄妇女的孕产妇死亡指标。选取2000、2005、2010、2015和2021年国家直接产科死因与间接产科死因死亡率作为联合结局变量,取对数后采用纵向K-means聚类(k =2~6)识别联合轨迹类型,并依据Calinski-Harabasz (CH)指数确定最优类别数。在聚类分型基础上,构建分段线性混合效应模型(随机截距),以2015年为结点分别估计2000年基线截距及MDG、SDG两个阶段的变化斜率。进一步提取2021年至少4次产前检查覆盖率、满足现代化避孕的比例、剖宫产率、女性人类免疫缺陷病毒(human immunodeficiency virus,HIV)流行率、机构分娩率、专业助产人员覆盖率及流产合法性指数等指标,采用Kruskal-Wallis H检验比较不同轨迹类型国家在卫生服务覆盖、健康风险暴露与制度环境方面的差异。结果: 纵向聚类结果显示,当k=3时CH指数达到峰值(CH=342.63),最终将204个国家和地区划分为高负担组(n=66)、中等负担组(n=88)与低负担组(n=50)3类联合轨迹。2021年3组直接孕产妇死亡率分别为334.6/10万活产(95%CI:282.5~386.7)、65.6/10万活产(95%CI:50.4~80.7)和5.4/10万活产(95%CI:3.7~7.0);间接MMR分别为33.6/10万活产(95%CI:27.9~39.2)、18.2/10万活产(95%CI:13.5~22.9)和0.9/10万活产(95%CI:0.6~1.3)。分段混合效应模型显示,在MDG阶段(2000—2015年),3组直接孕产妇死亡率均呈显著下降趋势(斜率分别为-0.020、-0.016、-0.036,P均<0.001);进入SDG阶段(2015—2021年)后,直接孕产妇死亡率下降明显放缓并趋于停滞(斜率分别为-0.011、0.011、-0.006, P>0.05)。间接孕产妇死亡率方面,MDG阶段高负担组与中等负担组呈小幅上升(斜率分别为0.029与0.015,P<0.05),低负担组变化不显著(P>0.05);SDG阶段中等负担组间接孕产妇死亡率出现显著加速上升(斜率为0.121,95%CI:0.092~0.151,P<0.001),而高负担组与低负担组总体平稳(P>0.05)。卫生系统与制度环境指标比较显示,3组差异均具有统计学意义(P<0.001):高负担组至少4次产前检查覆盖率、机构分娩率与专业助产覆盖率相对较低,现代避孕方法需求满足率较低且女性HIV流行率较高;中等负担组机构分娩率与专业助产覆盖率接近全覆盖,但剖宫产率处于较高水平;低负担组多项指标处于较优水平且流产合法性指数更高。结论: 2000—2021年全球国家层面直接与间接孕产妇死亡存在显著分化的联合轨迹。MDG阶段直接死因下降显著,但SDG阶段普遍放缓并出现停滞;与此同时,中等负担国家间接死因在SDG阶段显著上升,提示在总体孕产妇死亡率相对稳定的情况下可能存在结构性风险累积。将直接与间接死因的联合轨迹纳入常规监测框架,有助于分阶段、分类型识别不同国家孕产妇死亡转型特征并确定干预重点。
中图分类号:
- R173
| 1 |
World Health Organization, UNICEF, UNFPA, et al. Trends in maternal mortality 2000 to 2020: Estimates by WHO, UNICEF, UNFPA, World Bank Group and UNDESA/Population Division[M/OL]. Geneva: World Health Organization, 2023[2026-02-01]. https://iris.who.int/server/api/core/bitstreams/c3957b94-cdd5-47d7-85f8-6202be229f8e/content.
|
| 2 |
World Health Organization. SDG target 3.1 maternal mortality[EB/OL]. [2026-02-01]. https://www.who.int/data/gho/data/themes/topics/sdg-target-3-1-maternal-mortality.
|
| 3 |
World Health Organization. Millennium development goals (MDG)[EB/OL]. [2026-02-01]. https://www.who.int/zh/news-room/fact-sheets/detail/millennium-development-goals-%28mdgs%29.
|
| 4 |
|
| 5 |
doi: 10.1016/S2214-109X(23)00468-0 |
| 6 |
doi: 10.1016/S2214-109X(24)00560-6 |
| 7 |
doi: 10.1186/s12884-025-08443-w |
| 8 |
doi: 10.34172/aim.2022.105 |
| 9 |
|
| 10 |
|
| 11 |
Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2023 (GBD 2023) Covariates 1980-2023[EB/OL]. [2026-02-15]. https://doi.org/10.6069/b09t-1r53.
|
| 12 |
doi: 10.1016/S0140-6736(18)31668-4 |
| 13 |
doi: 10.1136/bmjgh-2024-016549 |
| 14 |
doi: 10.1016/S2214-109X(24)00145-1 |
| 15 |
|
| 16 |
|
| 17 |
|
| 18 |
|
| 19 |
|
| 20 |
|
| 21 |
|
| 22 |
|
| 23 |
|
| [1] | 王晓伟,穆英超,郭振宇,周玉博,张勇,李宏田,刘建蒙. 中国山东某县1951年以来出生女性初潮年龄与绝经年龄长期趋势[J]. 北京大学学报(医学版), 2023, 55(3): 502-510. |
| [2] | 何伟,杨思雯,陈娟,朱晓俊,陈志忠,马文军. 275 nm和310 nm紫外线对去卵巢骨质疏松大鼠骨代谢的影响[J]. 北京大学学报(医学版), 2022, 54(2): 236-243. |
| [3] | 宋沁峰,李宏田,杨静,原鹏波,程志浩,刘建蒙,赵扬玉. 双胎妊娠孕早期甲状腺功能及其与早产的关联性[J]. 北京大学学报(医学版), 2021, 53(3): 473-478. |
| [4] | 李雪莹, 毛康娜, 弭小艺, 高玲玲, 杨晓, 陶惠芬, 张迎武, 陈敬, 王行, 沈丽娟, 袁洁铃, 苗淼, 周虹. 育儿胜任感量表在学龄前儿童母亲中应用的信效度评价[J]. 北京大学学报(医学版), 2021, 53(3): 479-484. |
|
||
