北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (6): 1032-1036. doi: 10.19723/j.issn.1671-167X.2021.06.004
类风湿关节炎合并角膜溃疡的临床特点和相关因素分析
罗靓1,2,霍文岗3,张钦4,△( ),李春1,△()
),李春1,△()
- 1.北京大学人民医院风湿免疫科,北京 100044
2.重庆市中西医结合康复医院康复科,重庆 400013
3.河北以岭医院风湿免疫科,石家庄 050091
4.北京大学人民医院眼科,北京 100044
Clinical characteristics and risk factors of rheumatoid arthritis with ulcerative keratitis
LUO Liang1,2,HUO Wen-gang3,ZHANG Qin4,△(),LI Chun1,△()
- 1. Department of Rheumatology and Immunology, Peking University People’s Hospital, Beijing 100044, China
2. Department of Rehabilitation, Chongqing Rehabilitation Hospital of Integrated Traditional and Western, Chongqing 400013, China
3. Department of Rheumatology and Immunology, Hebei Yiling Hospital, Shijiazhuang 050091, China
4. Department of Ophthalmology, Peking University People's Hospital, Beijing 100044, China
摘要:
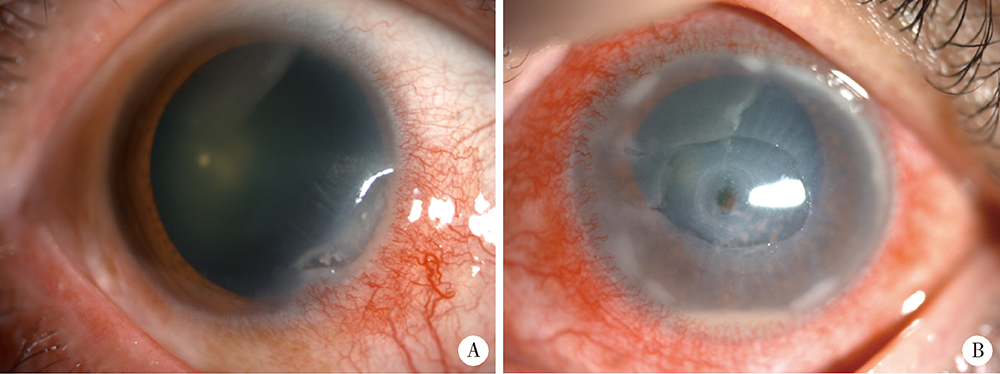
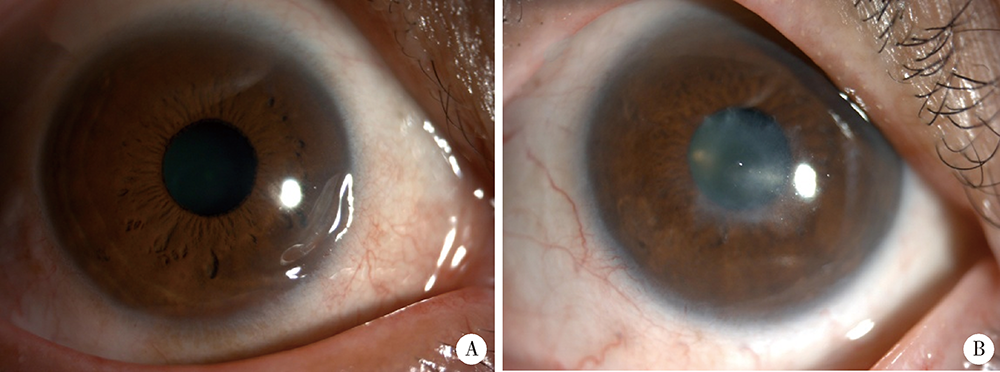
目的:探讨类风湿关节炎(rheumatoid arthritis,RA)合并角膜溃疡(ulcerative keratitis,UK)的临床特点、相关因素及临床转归。方法:选取2003年1月至2021年5月于北京大学人民医院住院的RA患者4 773例,筛选出合并UK的患者16例(UK组),通过倾向性评分匹配(propensity score matching,PSM), 选取无UK的对照组患者72例。对PSM后的两组患者的临床及实验室资料进行统计和分析。结果:RA合并UK表现为单纯边缘性UK 8例、边缘性UK伴穿孔5例、边缘性UK伴葡萄膜炎2例、中央性UK伴穿孔1例。UK组肿胀关节数显著高于对照组[6.0(2.5,23.0) vs. 3.0(1.0, 9.8),Z=-2.047,P=0.041],UK组继发干燥综合征(Sjögren syndrome,SS)的比例(37.5% vs. 6.9%, χ2=11.175,P=0.004)及间质性肺炎(interstitial lung disease,ILD,37.5% vs. 8.3%, χ2=9.456,P=0.008)的比例显著高于对照组,柳氮磺吡啶(12.5% vs. 48.6%, χ2=7.006,P=0.008)、来氟米特(31.3% vs. 63.9%, χ2=5.723,P=0.017)及金制剂(6.3% vs. 33.8%, χ2=4.841,P=0.032)的使用率显著低于对照组。回归分析显示肿胀关节数(OR=1.148)、继发SS(OR=79.118)、合并ILD(OR=6.596)及柳氮磺吡啶的使用(OR=0.037)与RA合并UK的发生存在独立相关性(P<0.05)。结论:UK为RA的少见并发症,多为边缘性UK。肿胀关节数、继发SS、合并ILD及柳氮磺吡啶的使用与RA合并UK发生存在独立相关性。
中图分类号:
- R593.22


| [1] | Jayaraj K, Alvin G, Charles S, et al. Correlation of ocular manifestations with the duration and activity of disease in patients with rheumatoid arthritis[J]. Int J Med Sci, 2017, 6(1):34-37. |
| [2] | Hamideh F, Prete P. Ophthalmologic manifestations of rheumatic diseases[J]. Semin Arthritis Rheum, 2001, 30(4):217-241. |
| [3] |
Foster CS, Forstot SL, Wilson LA. Mortality rate in rheumatoid arthritis patients developing necrotizing scleritis or peripheral ulcerative keratitis: effects of systemic immune suppression[J]. Ophthalmology, 1984, 91(10):1253-1263.
pmid: 6514289 |
| [4] |
Zandavalli F, Castro G, Mazzucco M, et. al. Infliximab is effective in difficult-to-control peripheral ulcerative keratitis. A report of three cases[J]. Rev Bras Reumatol, 2015, 55(3):310-312.
doi: 10.1016/j.rbr.2014.05.006 pmid: 25440698 |
| [5] |
Aletaha D, Neogi T, Silman J, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology / European League Against Rheumatism Collaborative Initiative[J]. Arthritis Rheum, 2010, 62(9):2569-2581.
doi: 10.1002/art.27584 |
| [6] | Yoshida M, Hariya T, Yokokura S, et al. Concomitant herpes simplex keratitis and autoimmune-associated ulcerative keratitis in rheumatoid arthritis patients[J]. Am J Ophthalmol Case Rep, 2020, 18:100648. |
| [7] |
Artifoni M, Rothschild R, Brézin A, et al. Ocular inflammatory diseases associated with rheumatoid arthritis[J]. Nat Rev Rheumatol, 2014, 10(2):108-116.
doi: 10.1038/nrrheum.2013.185 pmid: 24323074 |
| [8] |
Watanabe R, Ishii T, Yoshida M, et al. Ulcerative keratitis in patients with rheumatoid arthritis in the modern biologic era: a series of eight cases and literature review[J]. Int J Rheum Dis, 2017, 20(2):225-230.
doi: 10.1111/1756-185X.12688 pmid: 26179634 |
| [9] |
Harrold R, Shan Y, Rebello S, et al. Prevalence of Sjögren’s syndrome associated with rheumatoid arthritis in the USA: an observational study from the Corrona registry[J]. Clin Rheumatol, 2020, 39(6):1899-1905.
doi: 10.1007/s10067-020-05004-8 pmid: 32130579 |
| [10] |
Singh S, Das V, Basu S. Ocular involvement in Sjögren syndrome: risk factors for severe visual impairment and vision-threatening corneal complications[J]. Am J Ophthalmol, 2021, 225:11-17.
doi: 10.1016/j.ajo.2020.12.019 |
| [11] |
Maseda D, Bonami R, Crofford L. Regulation of B lymphocytes and plasma cells by innate immune mechanisms and stromal cells in rheumatoid arthritis[J]. Expert Rev Clin Immunol, 2014, 10(6):747-762.
doi: 10.1586/1744666X.2014.907744 |
| [12] |
Galor A, Thorne J. Scleritis and peripheral ulcerative keratitis[J]. Rheum Dis Clin North Am, 2007, 33(4):835-854.
doi: 10.1016/j.rdc.2007.08.002 |
| [13] | Wang F, Misra L, Patel V. In vivo confocal microscopy of the human cornea in the assessment of peripheral neuropathy and systemic diseases[J]. Biomed Res Int, 2015, 2015:951081. |
| [14] |
Sainz M, Foster S, Jabbur S, et al. Ocular characteristics and disease associations in scleritis-associated peripheral keratopathy[J]. Arch Ophthalmol, 2002, 120(1):15-19.
doi: 10.1001/archopht.120.1.15 |
| [15] |
Knox NE, Tole DM, Georgoudis P, et al. Peripheral ulcerative keratitis and corneal melt: a 10-year single center review with historical comparison[J]. Cornea, 2014, 33(1):27-31.
doi: 10.1097/ICO.0000000000000008 |
| [16] | 祝磊, 王丽娅, 张俊杰, 等. 0.05%他克莫司滴眼液治疗难治性免疫相关角膜溃疡的疗效及安全性研究[J]. 中华实验眼科杂志, 2015, 33(9):823-827. |
| [17] | 杨纪忠, 李冰. 类风湿关节炎相关性边缘角膜溃疡临床分析[J]. 山西医药杂志, 2009, 38(8):748-749. |
| [18] |
Bonnet I, Rousseau A, Duraffour P, et al. Efficacy and safety of rituximab in peripheral ulcerative keratitis associated with rheumatoid arthritis[J]. RMD Open, 2021, 7(1):e001472.
doi: 10.1136/rmdopen-2020-001472 |
| [19] |
Lucia D, Lara S, Vanesa R, et al. Biologic therapy in severe and refractory peripheral ulcerative keratitis (PUK). Multicenter study of 34 patients[J]. Semin Arthritis Rheum, 2020, 50(4):608-615.
doi: 10.1016/j.semarthrit.2020.03.023 |
| [20] |
Puéchal X, Gottenberg E, Berthelot M, et al. Rituximab therapy for systemic vasculitis associated with rheumatoid arthritis: results from the autoimmunity and rituximab registry[J]. Arthritis Care Res, 2012, 64(3):331-339.
doi: 10.1002/acr.20689 |
| [21] |
Peter K, Dirk B, Susann A, et al. Rapid healing of peripheral ulcerative keratitis in rheumatoid arthritis with prednisone, methotrexate and adalimumab combination therapy[J]. Rheumatology (Oxford), 2017, 56(7):1094.
doi: 10.1093/rheumatology/kex007 |
| [22] |
Messmer M, Foster S. Vasculitic peripheral ulcerative keratitis[J]. Surv Ophthalmol, 1999, 43(5):379-396.
pmid: 10340557 |
| [23] |
Messmer M, Foster S. Destructive corneal and scleral disease associated with rheumatoid arthritis: medical and surgical management[J]. Cornea, 1995, 14(4):408-417.
pmid: 7671613 |
| [1] | 魏慧, 张警丰, 姚中强, 赵金霞. 类风湿关节炎合并慢性病贫血患者的临床特征及相关因素[J]. 北京大学学报(医学版), 2026, 58(2): 307-312. |
| [2] | 吴滔, 林建子, 朱亚锋, 马剑达, 贾霈雯, 杨莉娟, 潘婕, 邹耀威, 杨迎, 卢烨, 戴冽. 血清蛋白质谱筛选及验证类风湿关节炎患者肌肉量减少的生物标志物[J]. 北京大学学报(医学版), 2025, 57(6): 1024-1031. |
| [3] | 丁艳, 王丽芳, 李超然, 卢哲敏, 石连杰. 利妥昔单抗成功治疗类风湿关节炎合并IgG4相关性疾病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1203-1207. |
| [4] | 杨菊, 徐婧, 戴菊华, 石连杰. Lumican蛋白在类风湿关节炎患者血清中的表达及其与疾病和免疫活动的相关性[J]. 北京大学学报(医学版), 2025, 57(5): 911-918. |
| [5] | 冯亮华, 洪丽荣, 陈雨佳, 蔡学明. 泛素特异性蛋白酶35对类风湿关节炎成纤维样滑膜细胞铁死亡的作用及机制[J]. 北京大学学报(医学版), 2025, 57(5): 919-925. |
| [6] | 贾霈雯, 杨迎, 邹耀威, 欧阳志明, 林建子, 马剑达, 杨葵敏, 戴冽. 类风湿关节炎患者低肌肉量综合征的临床特征及其对躯体功能的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1009-1016. |
| [7] | 马豆豆, 卢哲敏, 郭倩, 朱莎, 古今, 丁艳, 石连杰. 小剂量利妥昔单抗成功治疗类风湿关节炎合并重症肌无力1例[J]. 北京大学学报(医学版), 2024, 56(6): 1110-1114. |
| [8] | 闫蕊, 柯丹, 张妍, 李丽, 苏焕然, 陈伟, 孙明霞, 刘晓敏, 罗靓. 血清趋化因子CXCL-10和涎液化糖链抗原6水平在类风湿关节炎合并肺间质病变患者中的诊断和病情评估价值[J]. 北京大学学报(医学版), 2024, 56(6): 956-962. |
| [9] | 赵亮, 史成龙, 马柯, 赵静, 王潇, 邢晓燕, 莫万星, 练益瑞, 高超, 李玉慧. 抗合成酶综合征重叠类风湿关节炎患者的免疫学特征[J]. 北京大学学报(医学版), 2024, 56(6): 972-979. |
| [10] | 翟佳羽, 赵金霞, 安卓, 刘蕊. 低疾病活动度的中轴型脊柱关节炎患者残留症状评估及其相关因素分析[J]. 北京大学学报(医学版), 2024, 56(6): 987-993. |
| [11] | 韩艺钧, 陈小莉, 李常虹, 赵金霞. 甲氨蝶呤在类风湿关节炎患者中的应用现状[J]. 北京大学学报(医学版), 2024, 56(6): 994-1000. |
| [12] | 刘东武, 陈杰, 高明利, 于静. 类风湿关节炎伴发淋巴结Castleman样病理改变1例[J]. 北京大学学报(医学版), 2024, 56(5): 928-931. |
| [13] | 黄会娜,赵静,赵祥格,白自然,李霞,王冠. 乳酸对类风湿关节炎患者外周血CD4+T细胞亚群的调控作用[J]. 北京大学学报(医学版), 2024, 56(3): 519-525. |
| [14] | 汤晓菲,李永红,丁秋玲,孙卓,张阳,王育梅,田美伊,刘坚. 类风湿关节炎患者下肢深静脉血栓发病率及危险因素[J]. 北京大学学报(医学版), 2024, 56(2): 279-283. |
| [15] | 邹雪,白小娟,张丽卿. 艾拉莫德联合托法替布治疗难治性中重度类风湿关节炎的疗效[J]. 北京大学学报(医学版), 2023, 55(6): 1013-1021. |
|
||
