北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (6): 1026-1031. doi: 10.19723/j.issn.1671-167X.2021.06.003
类风湿关节炎患者趋化因子CXCL9和CXCL10在骨侵蚀中的作用
钟华,徐丽玲,白明欣,苏茵( )
)
- 北京大学人民医院风湿免疫科,风湿病机制及免疫诊断北京市重点实验室,北京 100044
Effect of chemokines CXCL9 and CXCL10 on bone erosion in patients with rheumatoid arthritis
ZHONG Hua,XU Li-ling,BAI Ming-xin,SU Yin()
- Beijing Key Laboratory for Rheumatism Mechanism and Immune Diagnosis, Beijing 100044, China
摘要:
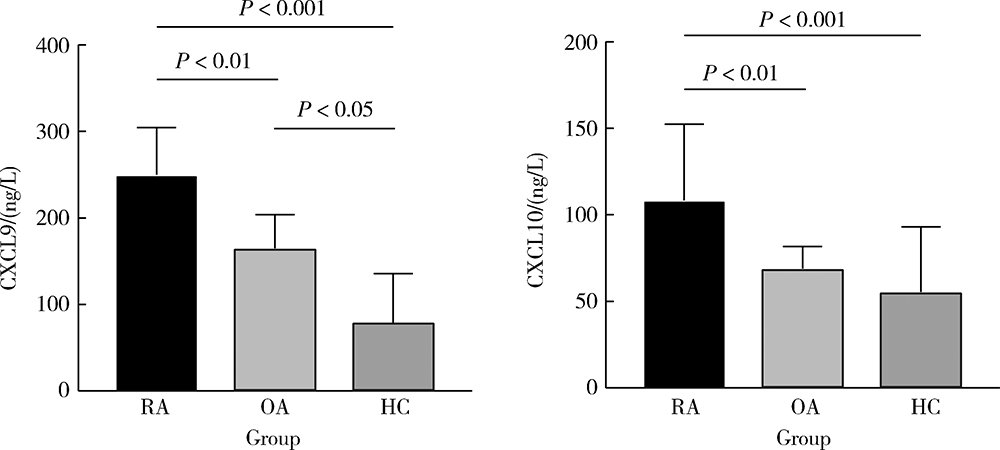
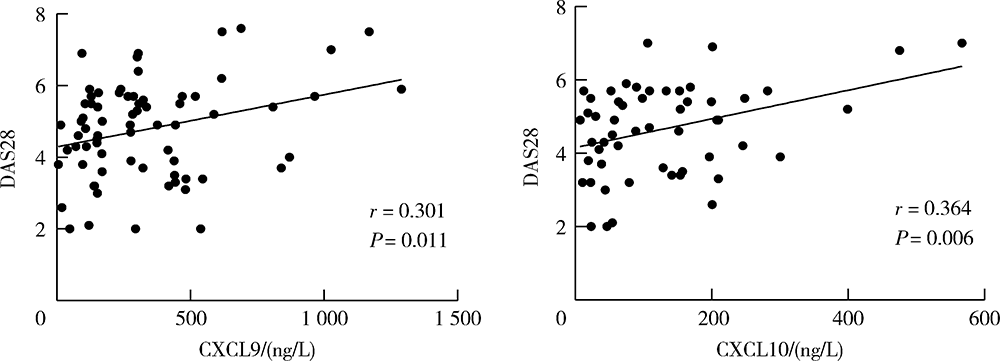
目的:检测趋化因子CXCL9和CXCL10在类风湿关节炎(rheumatoid arthritis, RA)患者外周血中的水平,分析其对RA发生骨侵蚀的作用,探讨CXCL9和CXCL10在RA中的临床意义。方法:采用酶联免疫吸附试验(enzyme linked immunosorbent assay, ELISA)检测105例RA患者、90例骨关节炎(osteoarthritis, OA)患者和25例健康对照者(healthy control, HC)血清CXCL9、CXCL10水平并比较各组间差异,分析其与RA临床特征、实验室指标、疾病活动性及骨侵蚀的相关性,采用Logistic回归分析血清CXCL9和CXCL10水平与RA患者骨侵蚀的相关性。结果:RA组患者血清CXCL9、CXCL10水平显著高于OA组和HC组(P<0.01、P<0.01),RA患者血清CXCL9水平与肿胀关节数(swollen joints, SJC)、类风湿因子(rheumatoid factor, RF)呈正相关(P<0.05),血清CXCL10水平与压痛关节数(tender joints, TJC)、SJC、C反应蛋白(C-reactive protein, CRP)、免疫球蛋白(immunoglobulin, Ig)A、IgM、RF及抗环瓜氨酸多肽抗体(anti-cyclic citrullinated peptide antibody,ACPA)呈正相关(P<0.05)。此外,血清CXCL9、CXCL10水平均与RA疾病活动度评分(disease activity score 28, DAS28)呈正相关(P=0.013、P=0.006),且高疾病活动度组(DAS28≥5.1)的血清CXCL9、CXCL10水平显著高于中低疾病活动度组(DAS28<5.1,P<0.05)。Logistic回归分析提示,病程长、高疾病活动度及血清CXCL9水平升高与RA患者发生骨侵蚀相关(P<0.05)。结论:RA患者血清趋化因子CXCL9和CXCL10的表达水平升高,与RA疾病活动性及骨侵蚀具有相关性,可能参与了RA的发病及骨破坏过程。
中图分类号:
- R593.22

| [1] |
Sparks JA. Rheumatoid arthritis [J]. Ann Intern Med, 2019, 170(1): ITC1-ITC16.
doi: 10.7326/AITC201901010 |
| [2] |
Zhu H, Li R, Da Z, et al. Remission assessment of rheumatoid arthritis in daily practice in China: A cross-sectional observational study[J]. Clin Rheumatol, 2018, 37(3):597-605.
doi: 10.1007/s10067-017-3850-z |
| [3] |
Zhou Y, Wang X, An Y, et al. Disability and health-related quality of life in Chinese patients with rheumatoid arthritis: A cross-sectional study[J]. Int J Rheum Dis, 2018, 21(9):1709-1715.
doi: 10.1111/apl.2018.21.issue-9 |
| [4] |
Poeta VM, Massara M, Capucetti A, et al. Chemokines and chemokine receptors: new targets for cancer immunotherapy[J]. Front Immunol, 2019, 10:379.
doi: 10.3389/fimmu.2019.00379 |
| [5] |
Susek KH, Karvouni M, Alici E, et al. The role of CXC chemokine receptors 1-4 on immune cells in the tumor microenvironment[J]. Front Immunol, 2018, 9:2159.
doi: 10.3389/fimmu.2018.02159 |
| [6] |
Tokunaga R, Zhang W, Naseem M, et al. CXCL9, CXCL10, CXCL11/CXCR3 axis for immune activation: A target for novel cancer therapy[J]. Cancer Treat Rev, 2018, 63:40-47.
doi: S0305-7372(17)30199-8 pmid: 29207310 |
| [7] |
McInnes IB, Schett G. The pathogenesis of rheumatoid arthritis[J]. N Engl J Med, 2011, 365(23):2205-2219.
doi: 10.1056/NEJMra1004965 |
| [8] |
Muntyanu A, Abji F, Liang K, et al. Differential gene and protein expression of chemokines and cytokines in synovial fluid of patients with arthritis[J]. Arthritis Res Ther, 2016, 18(1):296.
doi: 10.1186/s13075-016-1196-6 |
| [9] |
Antonelli A, Ferrari SM, Giuggioli D, et al. Chemokine (C-X-C motif) ligand CXCL10 in autoimmune diseases[J]. Autoimmun Rev, 2014, 13(3):272-280.
doi: 10.1016/j.autrev.2013.10.010 |
| [10] |
Aletaha D, Neogi T, Silman AJ, et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative[J]. Arthritis Rheum, 2010, 62(9):2569-2581.
doi: 10.1002/art.27584 |
| [11] |
Zhang W, Doherty M, Peat G, et al. EULAR evidence-based recommendations for the diagnosis of knee osteoarthritis[J]. Ann Rheum Dis, 2010, 69(3):483-489.
doi: 10.1136/ard.2009.113100 pmid: 19762361 |
| [12] |
Prevoo ML, van’t Hof MA, Kuper HH, et al. Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis[J]. Arthritis Rheum, 1995, 38(1):44-48.
doi: 10.1002/art.v38:1 |
| [13] |
Fransen J, van Riel PL. The disease activity score and the EULAR response criteria [J]. Rheum Dis Clin North Am, 2009, 35(4): 745-757, vii-viii.
doi: 10.1016/j.rdc.2009.10.001 |
| [14] |
Arnett FC, Edworthy SM, Bloch DA, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis[J]. Arthritis Rheum, 1988, 31(3):315-324.
doi: 10.1002/(ISSN)1529-0131 |
| [15] | Ostergaard M, Peterfy C, Conaghan P, et al. OMERACT rheumatoid arthritis magnetic resonance imaging studies. Core set of MRI acquisitions, joint pathology definitions, and the OMERACT RA-MRI scoring system[J]. J Rheumatol, 2003, 30(6):1385-1386. |
| [16] |
Bruyn GA, Hanova P, Iagnocco A, et al. Ultrasound definition of tendon damage in patients with rheumatoid arthritis. Results of a OMERACT consensus-based ultrasound score focusing on the diagnostic reliability[J]. Ann Rheum Dis, 2014, 73(11):1929-1934.
doi: 10.1136/annrheumdis-2013-203596 |
| [17] |
Zeidler H. The need to better classify and diagnose early and very early rheumatoid arthritis[J]. J Rheumatol, 2012, 39(2):212-217.
doi: 10.3899/jrheum.110967 |
| [18] |
Griffith JW, Sokol CL, Luster AD. Chemokines and chemokine receptors: Positioning cells for host defense and immunity[J]. Annu Rev Immunol, 2014, 32:659-702.
doi: 10.1146/annurev-immunol-032713-120145 pmid: 24655300 |
| [19] |
Korniejewska A, McKnight AJ, Johnson Z, et al. Expression and agonist responsiveness of CXCR3 variants in human T lymphocytes[J]. Immunology, 2011, 132(4):503-515.
doi: 10.1111/j.1365-2567.2010.03384.x pmid: 21255008 |
| [20] |
Schoenborn JR, Wilson CB. Regulation of interferon-gamma during innate and adaptive immune responses[J]. Adv Immunol, 2007, 96:41-101.
pmid: 17981204 |
| [21] |
Farber JM. Mig and IP-10: CXC chemokines that target lymphocytes[J]. J Leukoc Biol, 1997, 61(3):246-257.
doi: 10.1002/jlb.1997.61.issue-3 |
| [22] |
Kwak HB, Ha H, Kim HN, et al. Reciprocal cross-talk between RANKL and interferon-gamma-inducible protein 10 is responsible for bone-erosive experimental arthritis[J]. Arthritis Rheum, 2008, 58(5):1332-1342.
doi: 10.1002/(ISSN)1529-0131 |
| [23] |
Kraan MC, Patel DD, Haringman JJ, et al. The development of clinical signs of rheumatoid synovial inflammation is associated with increased synjournal of the chemokine CXCL8 (interleukin-8)[J]. Arthritis Res, 2001, 3(1):65-71.
pmid: 11178128 |
| [1] | 魏慧, 张警丰, 姚中强, 赵金霞. 类风湿关节炎合并慢性病贫血患者的临床特征及相关因素[J]. 北京大学学报(医学版), 2026, 58(2): 307-312. |
| [2] | 吴滔, 林建子, 朱亚锋, 马剑达, 贾霈雯, 杨莉娟, 潘婕, 邹耀威, 杨迎, 卢烨, 戴冽. 血清蛋白质谱筛选及验证类风湿关节炎患者肌肉量减少的生物标志物[J]. 北京大学学报(医学版), 2025, 57(6): 1024-1031. |
| [3] | 丁艳, 王丽芳, 李超然, 卢哲敏, 石连杰. 利妥昔单抗成功治疗类风湿关节炎合并IgG4相关性疾病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1203-1207. |
| [4] | 杨菊, 徐婧, 戴菊华, 石连杰. Lumican蛋白在类风湿关节炎患者血清中的表达及其与疾病和免疫活动的相关性[J]. 北京大学学报(医学版), 2025, 57(5): 911-918. |
| [5] | 冯亮华, 洪丽荣, 陈雨佳, 蔡学明. 泛素特异性蛋白酶35对类风湿关节炎成纤维样滑膜细胞铁死亡的作用及机制[J]. 北京大学学报(医学版), 2025, 57(5): 919-925. |
| [6] | 刘伟, 郭稳, 过哲, 李春艳, 李云龙, 刘思奇, 张亮, 宋慧. 痛风患者放射学阴性骨侵蚀的相关危险因素[J]. 北京大学学报(医学版), 2025, 57(4): 735-739. |
| [7] | 贾霈雯, 杨迎, 邹耀威, 欧阳志明, 林建子, 马剑达, 杨葵敏, 戴冽. 类风湿关节炎患者低肌肉量综合征的临床特征及其对躯体功能的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1009-1016. |
| [8] | 马豆豆, 卢哲敏, 郭倩, 朱莎, 古今, 丁艳, 石连杰. 小剂量利妥昔单抗成功治疗类风湿关节炎合并重症肌无力1例[J]. 北京大学学报(医学版), 2024, 56(6): 1110-1114. |
| [9] | 闫蕊, 柯丹, 张妍, 李丽, 苏焕然, 陈伟, 孙明霞, 刘晓敏, 罗靓. 血清趋化因子CXCL-10和涎液化糖链抗原6水平在类风湿关节炎合并肺间质病变患者中的诊断和病情评估价值[J]. 北京大学学报(医学版), 2024, 56(6): 956-962. |
| [10] | 赵亮, 史成龙, 马柯, 赵静, 王潇, 邢晓燕, 莫万星, 练益瑞, 高超, 李玉慧. 抗合成酶综合征重叠类风湿关节炎患者的免疫学特征[J]. 北京大学学报(医学版), 2024, 56(6): 972-979. |
| [11] | 韩艺钧, 陈小莉, 李常虹, 赵金霞. 甲氨蝶呤在类风湿关节炎患者中的应用现状[J]. 北京大学学报(医学版), 2024, 56(6): 994-1000. |
| [12] | 刘东武, 陈杰, 高明利, 于静. 类风湿关节炎伴发淋巴结Castleman样病理改变1例[J]. 北京大学学报(医学版), 2024, 56(5): 928-931. |
| [13] | 黄会娜,赵静,赵祥格,白自然,李霞,王冠. 乳酸对类风湿关节炎患者外周血CD4+T细胞亚群的调控作用[J]. 北京大学学报(医学版), 2024, 56(3): 519-525. |
| [14] | 汤晓菲,李永红,丁秋玲,孙卓,张阳,王育梅,田美伊,刘坚. 类风湿关节炎患者下肢深静脉血栓发病率及危险因素[J]. 北京大学学报(医学版), 2024, 56(2): 279-283. |
| [15] | 邹雪,白小娟,张丽卿. 艾拉莫德联合托法替布治疗难治性中重度类风湿关节炎的疗效[J]. 北京大学学报(医学版), 2023, 55(6): 1013-1021. |
|
||
