北京大学学报(医学版) ›› 2025, Vol. 57 ›› Issue (6): 1024-1031. doi: 10.19723/j.issn.1671-167X.2025.06.003
血清蛋白质谱筛选及验证类风湿关节炎患者肌肉量减少的生物标志物
吴滔1, 林建子1, 朱亚锋2, 马剑达1, 贾霈雯1, 杨莉娟1, 潘婕1, 邹耀威1, 杨迎1, 卢烨1, 戴冽1,*( )
)
- 1. 中山大学孙逸仙纪念医院风湿免疫科,广州 510120
2. 中山大学孙逸仙纪念医院基础与转化医学研究中心,广州 510120
Serum inter-alpha-trypsin inhibitor heavy chain H3 is identified as a potential biomarker for myopenia in patients with rheumatoid arthritis using proteomic profiling
Tao WU1, Jianzi LIN1, Yafeng ZHU2, Jianda MA1, Peiwen JIA1, Lijuan YANG1, jie PAN1, Yaowei ZOU1, Ying YANG1, Ye LU1, Lie DAI1,*()
- 1. Department of Rheumatology and Immunology, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, 510120, China
2. Basic and Translational Medical Research Center, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, 510120, China
摘要:
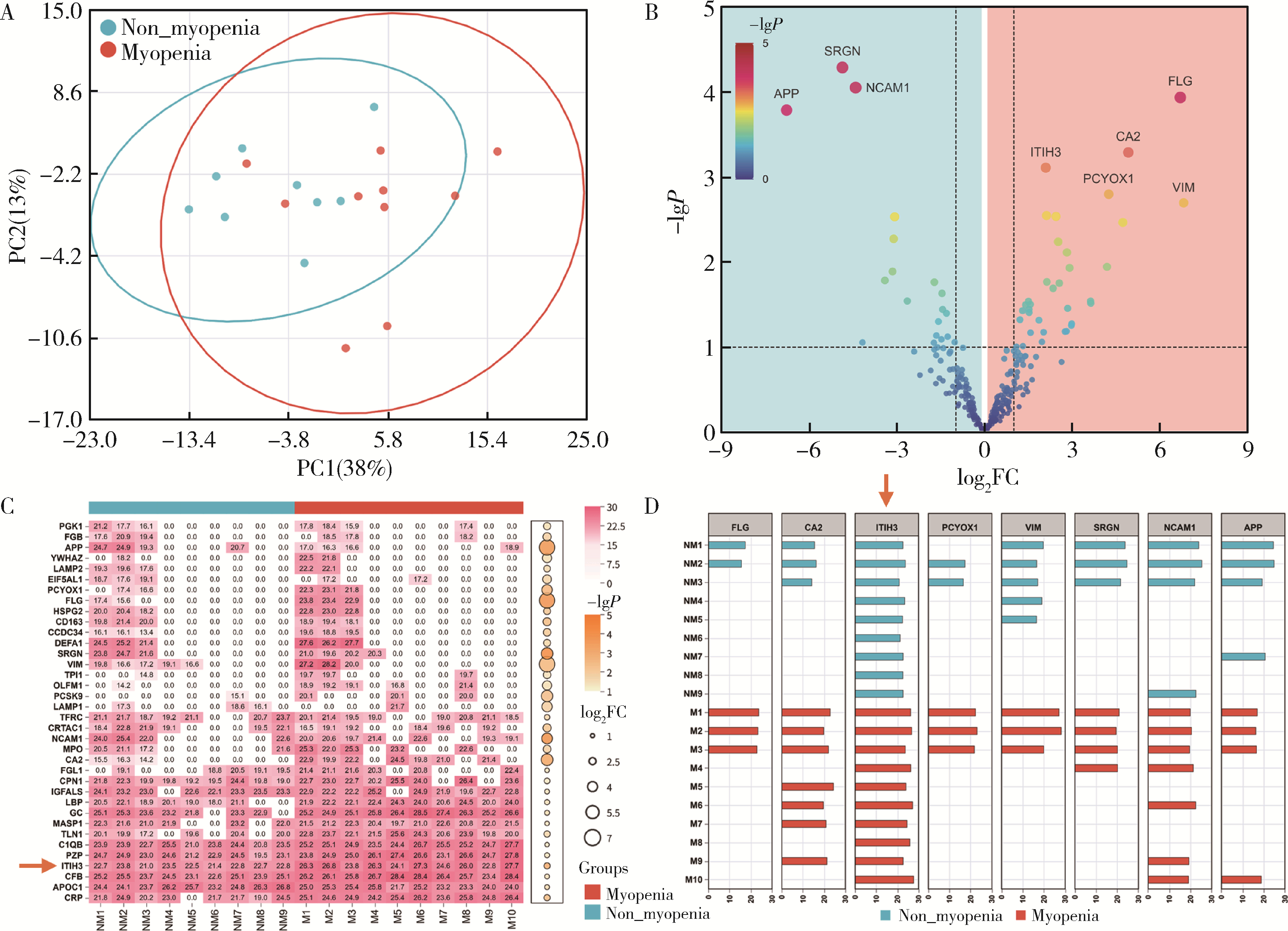
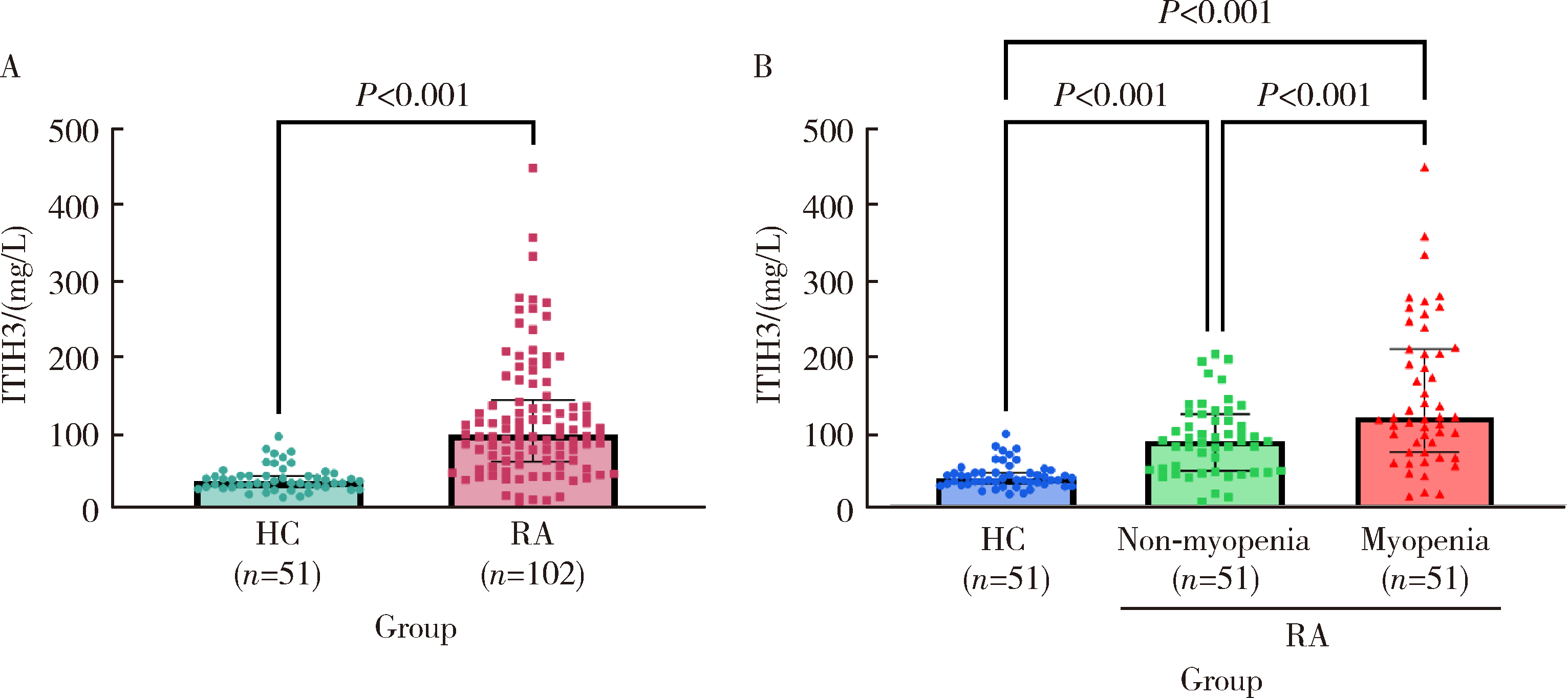
目的: 探索类风湿关节炎(rheumatoid arthritis,RA)患者肌肉量减少的生物标志物。方法: 本研究为横断面研究,采用非标记液相色谱-串联质谱技术检测基线病情活动且2年随访期间保持肌肉量正常或肌肉量减少的RA患者血清蛋白组学特征,并通过生物信息学分析两组患者血清中的差异蛋白;进一步纳入102例RA患者(肌肉量减少组和肌肉量正常组各51例)及招募志愿者51例作为健康对照组(healthy controls,HC)进行差异蛋白的ELISA验证,并采用Logistic回归分析RA患者基线肌肉量减少的相关因素。结果: 10例肌肉量减少组与9例肌肉量正常组RA患者通过基线血清蛋白组学分析筛选出38个差异蛋白,其中间-α-胰蛋白酶抑制蛋白重链3(inter-alpha-trypsin inhibitor heavy chain H3,ITIH3)表达差异显著(log2FC=2.09),并在所有血清样本中稳定表达。ELISA验证结果显示102例RA患者血清ITIH3水平显著高于HC组[(119.4±79.7) mg/L vs. (42.3±16.6) mg/L, P < 0.001],且肌肉量减少组RA患者血清ITIH3显著高于肌肉量正常组[(148.1±94.7) mg/L vs. (90.8±46.6) mg/L, P < 0.001]。多因素Logistic回归分析结果显示,校正混杂因素后,血清ITIH3水平仍是RA患者肌肉量减少的独立危险因素(OR=1.024,95%CI:1.013~1.038,P < 0.001)。结论: 血清ITIH3水平是RA患者肌肉量减少的独立危险因素,提示ITIH3可能是RA肌肉量减少的潜在生物标志物。
中图分类号:
- R593.22


| 1 |
中华医学会老年医学分会, 国家老年疾病临床医学研究中心(湘雅医院). 中国肌肉减少症诊疗指南(2024版)[J]. 中华医学杂志, 2025, 105(3): 181- 203.
|
| 2 |
doi: 10.1038/s41413-025-00438-9 |
| 3 |
doi: 10.1007/s13539-011-0025-7 |
| 4 |
doi: 10.1002/jcsm.12381 |
| 5 |
doi: 10.1080/03009742.2020.1842902 |
| 6 |
doi: 10.1038/s41584-023-00921-9 |
| 7 |
doi: 10.1007/s40520-016-0717-0 |
| 8 |
doi: 10.3390/medicina61040551 |
| 9 |
doi: 10.3389/fnut.2022.1007184 |
| 10 |
doi: 10.1177/1759720X20946220 |
| 11 |
国家皮肤与免疫疾病临床医学研究中心(北京协和医院), 中国医师协会风湿免疫专科医师分会, 中国康复医学会风湿免疫病康复专业委员会, 等. 2024中国类风湿关节炎诊疗指南[J]. 中华内科杂志, 2024, 63(11): 1059- 1077.
|
| 12 |
贾霈雯, 杨迎, 邹耀威, 等. 类风湿关节炎患者低肌肉量综合征的临床特征及其对躯体功能的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1009- 1016.
|
| 13 |
doi: 10.1074/jbc.M808560200 |
| 14 |
doi: 10.1074/jbc.M111.324913 |
| 15 |
doi: 10.1186/s12967-025-06563-7 |
| 16 |
doi: 10.3390/cells11081256 |
| 17 |
doi: 10.1007/s00401-024-02754-6 |
| [1] | 丁艳, 王丽芳, 李超然, 卢哲敏, 石连杰. 利妥昔单抗成功治疗类风湿关节炎合并IgG4相关性疾病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1203-1207. |
| [2] | 杨丛艺, 郑小雯, 陈静宜, 徐俊, 陈峰, 陈扬, 陈宁. 溃疡性结肠炎患者唾液外泌体内蛋白标志物的筛选及功能分析[J]. 北京大学学报(医学版), 2025, 57(5): 895-902. |
| [3] | 杨菊, 徐婧, 戴菊华, 石连杰. Lumican蛋白在类风湿关节炎患者血清中的表达及其与疾病和免疫活动的相关性[J]. 北京大学学报(医学版), 2025, 57(5): 911-918. |
| [4] | 冯亮华, 洪丽荣, 陈雨佳, 蔡学明. 泛素特异性蛋白酶35对类风湿关节炎成纤维样滑膜细胞铁死亡的作用及机制[J]. 北京大学学报(医学版), 2025, 57(5): 919-925. |
| [5] | 贾霈雯, 杨迎, 邹耀威, 欧阳志明, 林建子, 马剑达, 杨葵敏, 戴冽. 类风湿关节炎患者低肌肉量综合征的临床特征及其对躯体功能的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1009-1016. |
| [6] | 马豆豆, 卢哲敏, 郭倩, 朱莎, 古今, 丁艳, 石连杰. 小剂量利妥昔单抗成功治疗类风湿关节炎合并重症肌无力1例[J]. 北京大学学报(医学版), 2024, 56(6): 1110-1114. |
| [7] | 闫蕊, 柯丹, 张妍, 李丽, 苏焕然, 陈伟, 孙明霞, 刘晓敏, 罗靓. 血清趋化因子CXCL-10和涎液化糖链抗原6水平在类风湿关节炎合并肺间质病变患者中的诊断和病情评估价值[J]. 北京大学学报(医学版), 2024, 56(6): 956-962. |
| [8] | 赵亮, 史成龙, 马柯, 赵静, 王潇, 邢晓燕, 莫万星, 练益瑞, 高超, 李玉慧. 抗合成酶综合征重叠类风湿关节炎患者的免疫学特征[J]. 北京大学学报(医学版), 2024, 56(6): 972-979. |
| [9] | 韩艺钧, 陈小莉, 李常虹, 赵金霞. 甲氨蝶呤在类风湿关节炎患者中的应用现状[J]. 北京大学学报(医学版), 2024, 56(6): 994-1000. |
| [10] | 刘东武, 陈杰, 高明利, 于静. 类风湿关节炎伴发淋巴结Castleman样病理改变1例[J]. 北京大学学报(医学版), 2024, 56(5): 928-931. |
| [11] | 黄会娜,赵静,赵祥格,白自然,李霞,王冠. 乳酸对类风湿关节炎患者外周血CD4+T细胞亚群的调控作用[J]. 北京大学学报(医学版), 2024, 56(3): 519-525. |
| [12] | 汤晓菲,李永红,丁秋玲,孙卓,张阳,王育梅,田美伊,刘坚. 类风湿关节炎患者下肢深静脉血栓发病率及危险因素[J]. 北京大学学报(医学版), 2024, 56(2): 279-283. |
| [13] | 邹雪,白小娟,张丽卿. 艾拉莫德联合托法替布治疗难治性中重度类风湿关节炎的疗效[J]. 北京大学学报(医学版), 2023, 55(6): 1013-1021. |
| [14] | 吴琦,蔡月明,何娟,黄文蒂,王庆文. 血脂异常与类风湿关节炎肺间质病变的相关性分析[J]. 北京大学学报(医学版), 2023, 55(6): 982-992. |
| [15] | 张警丰,金银姬,魏慧,姚中强,赵金霞. 体重指数与类风湿关节炎临床特征的相关性分析[J]. 北京大学学报(医学版), 2023, 55(6): 993-999. |
|
||
