北京大学学报(医学版) ›› 2025, Vol. 57 ›› Issue (6): 1203-1207. doi: 10.19723/j.issn.1671-167X.2025.06.029
利妥昔单抗成功治疗类风湿关节炎合并IgG4相关性疾病1例
丁艳, 王丽芳, 李超然, 卢哲敏, 石连杰*( )
)
- 北京大学首钢医院风湿免疫科, 北京 100144
Rheumatoid arthritis combined with IgG4-related disease successfully treated with rituximab: A case report
Yan DING, Lifang WANG, Chaoran LI, Zhemin LU, Lianjie SHI*()
- Department of Rheumatology and Immunology, Peking University Shougang Hospital, Beijing 100144, China
摘要:
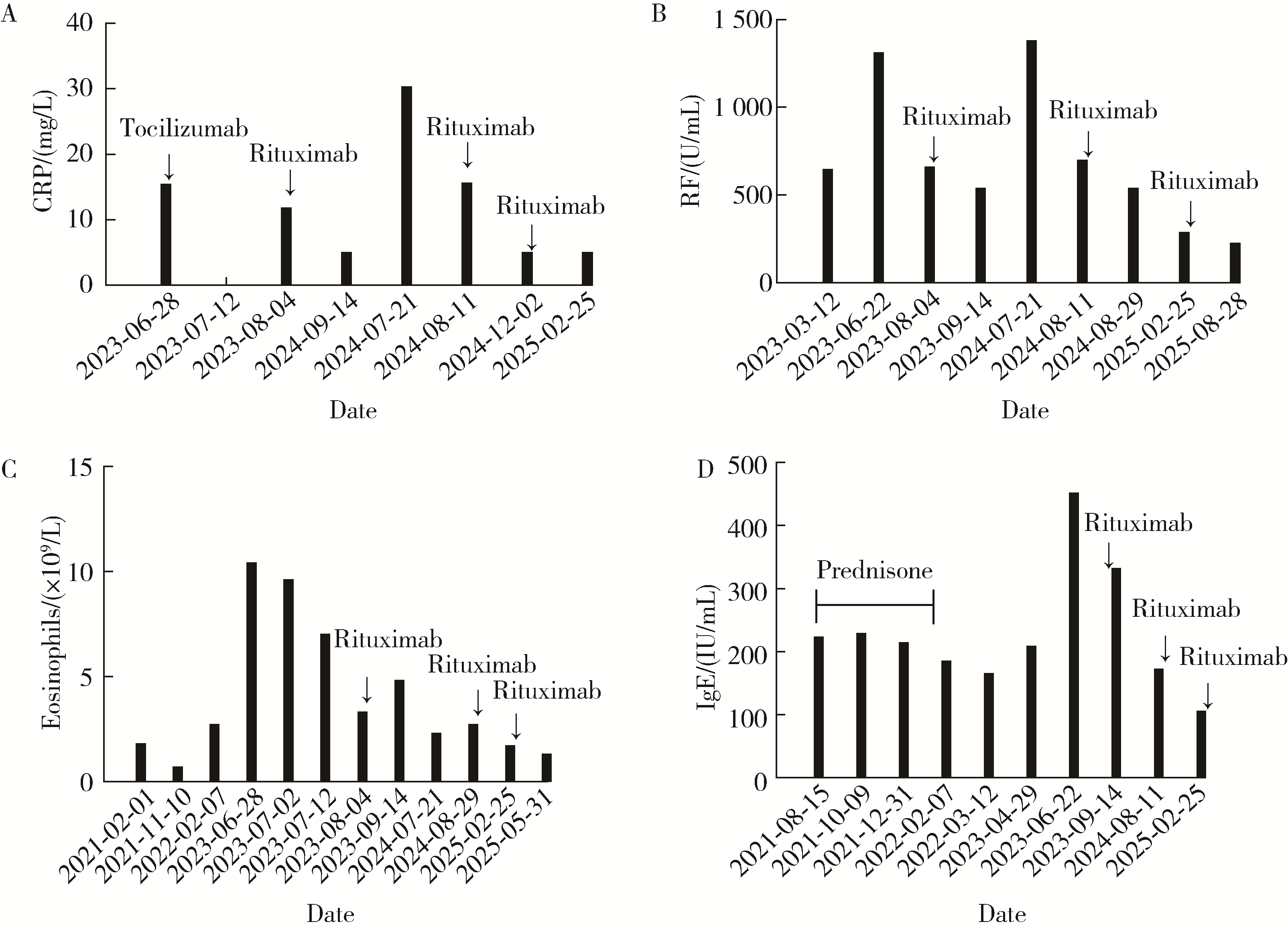
类风湿关节炎是一种以慢性对称性关节炎为主要表现的自身免疫性疾病, 合并嗜酸性粒细胞增高的类风湿关节炎有其自身特征, 但也应警惕合并免疫球蛋白(immunoglobulin, Ig)G4相关性疾病的可能。本文报道1例以多关节肿痛伴晨僵为主要表现的患者, 抗角蛋白抗体、抗环瓜氨酸肽抗体、抗核周因子抗体及类风湿因子阳性, 红细胞沉降率明显升高, 明确诊断类风湿关节炎。该患者病程中逐渐出现外周血嗜酸性粒细胞升高, 使用来氟米特、雷公藤多苷等药物治疗效果欠佳。调整为甲氨蝶呤及托珠单抗治疗后, 患者关节症状明显好转, 但外周血嗜酸性粒细胞升高无明显改善。病程中患者出现淋巴结及腮腺肿大, 淋巴结超声提示左侧锁骨上低回声结节, 双侧腋下、右侧腹股沟区异常淋巴结, 双侧颈部、左侧腹股沟区淋巴结可见。腮腺超声提示双侧腮腺内低回声结节, 腮腺导管增宽, 骨髓穿刺活检未见明显异常, 淋巴结病理活检提示有IgG4+细胞浸润, 进一步完善血清IgG4, 发现血清IgG4升高。最终诊断为类风湿关节炎合并IgG4相关性疾病可能, 调整治疗为甲氨蝶呤联合利妥昔单抗治疗, 患者关节肿痛明显好转, C反应蛋白逐渐恢复正常, 嗜酸性粒细胞明显下降, 病情缓解。因此, 对于合并嗜酸性粒细胞增多的类风湿关节炎应警惕IgG4相关性疾病的可能, 采用利妥昔单抗为临床治疗提供了新思路。
中图分类号:
- R593.2

| 1 |
doi: 10.1002/art.41120 |
| 2 |
doi: 10.1007/s00296-018-4191-1 |
| 3 |
doi: 10.1136/rmdopen-2015-000070 |
| 4 |
doi: 10.1038/s41584-018-0109-2 |
| 5 |
doi: 10.1016/j.berh.2016.07.003 |
| 6 |
doi: 10.1038/s41598-019-52847-6 |
| 7 |
doi: 10.1093/rheumatology/ken336 |
| 8 |
doi: 10.7150/ijbs.5996 |
| 9 |
doi: 10.1016/S0952-7915(96)80058-6 |
| 10 |
doi: 10.1007/s00428-002-0702-1 |
| 11 |
|
| 12 |
|
| 13 |
doi: 10.1136/gutjnl-2015-310336 |
| 14 |
|
| 15 |
|
| 16 |
doi: 10.1007/s10067-019-04699-8 |
| 17 |
doi: 10.1111/1756-185X.14920 |
| 18 |
doi: 10.1055/s-0044-1782218 |
| 19 |
doi: 10.1136/annrheumdis-2014-206605 |
| 20 |
张文, 董凌莉, 朱剑, 等. IgG 4相关性疾病诊治中国专家共识[J]. 中华内科杂志, 2021, 60 (3): 192- 206.
|
| 21 |
doi: 10.1016/j.ejim.2019.12.029 |
| [1] | 吴滔, 林建子, 朱亚锋, 马剑达, 贾霈雯, 杨莉娟, 潘婕, 邹耀威, 杨迎, 卢烨, 戴冽. 血清蛋白质谱筛选及验证类风湿关节炎患者肌肉量减少的生物标志物[J]. 北京大学学报(医学版), 2025, 57(6): 1024-1031. |
| [2] | 赵亚云, 倪梦凡, 李雪, 王蓓, 程功, 何菁, 金月波. 利妥昔单抗治疗原发性干燥综合征肾损害的临床疗效和安全性[J]. 北京大学学报(医学版), 2025, 57(6): 1051-1060. |
| [3] | 杨菊, 徐婧, 戴菊华, 石连杰. Lumican蛋白在类风湿关节炎患者血清中的表达及其与疾病和免疫活动的相关性[J]. 北京大学学报(医学版), 2025, 57(5): 911-918. |
| [4] | 冯亮华, 洪丽荣, 陈雨佳, 蔡学明. 泛素特异性蛋白酶35对类风湿关节炎成纤维样滑膜细胞铁死亡的作用及机制[J]. 北京大学学报(医学版), 2025, 57(5): 919-925. |
| [5] | 贾霈雯, 杨迎, 邹耀威, 欧阳志明, 林建子, 马剑达, 杨葵敏, 戴冽. 类风湿关节炎患者低肌肉量综合征的临床特征及其对躯体功能的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1009-1016. |
| [6] | 马豆豆, 卢哲敏, 郭倩, 朱莎, 古今, 丁艳, 石连杰. 小剂量利妥昔单抗成功治疗类风湿关节炎合并重症肌无力1例[J]. 北京大学学报(医学版), 2024, 56(6): 1110-1114. |
| [7] | 闫蕊, 柯丹, 张妍, 李丽, 苏焕然, 陈伟, 孙明霞, 刘晓敏, 罗靓. 血清趋化因子CXCL-10和涎液化糖链抗原6水平在类风湿关节炎合并肺间质病变患者中的诊断和病情评估价值[J]. 北京大学学报(医学版), 2024, 56(6): 956-962. |
| [8] | 赵亮, 史成龙, 马柯, 赵静, 王潇, 邢晓燕, 莫万星, 练益瑞, 高超, 李玉慧. 抗合成酶综合征重叠类风湿关节炎患者的免疫学特征[J]. 北京大学学报(医学版), 2024, 56(6): 972-979. |
| [9] | 韩艺钧, 陈小莉, 李常虹, 赵金霞. 甲氨蝶呤在类风湿关节炎患者中的应用现状[J]. 北京大学学报(医学版), 2024, 56(6): 994-1000. |
| [10] | 刘东武, 陈杰, 高明利, 于静. 类风湿关节炎伴发淋巴结Castleman样病理改变1例[J]. 北京大学学报(医学版), 2024, 56(5): 928-931. |
| [11] | 黄会娜,赵静,赵祥格,白自然,李霞,王冠. 乳酸对类风湿关节炎患者外周血CD4+T细胞亚群的调控作用[J]. 北京大学学报(医学版), 2024, 56(3): 519-525. |
| [12] | 汤晓菲,李永红,丁秋玲,孙卓,张阳,王育梅,田美伊,刘坚. 类风湿关节炎患者下肢深静脉血栓发病率及危险因素[J]. 北京大学学报(医学版), 2024, 56(2): 279-283. |
| [13] | 邹雪,白小娟,张丽卿. 艾拉莫德联合托法替布治疗难治性中重度类风湿关节炎的疗效[J]. 北京大学学报(医学版), 2023, 55(6): 1013-1021. |
| [14] | 冯璐,翟佳羽,赵金霞. IgG4相关性疾病患者就诊情况及其临床特征[J]. 北京大学学报(医学版), 2023, 55(6): 1028-1032. |
| [15] | 吴洁,张雯,梁舒,秦艺璐,范文强. 妊娠期原发性干燥综合征合并视神经脊髓炎谱系疾病危重症1例[J]. 北京大学学报(医学版), 2023, 55(6): 1118-1124. |
|
||
