北京大学学报(医学版) ›› 2024, Vol. 56 ›› Issue (6): 1036-1040. doi: 10.19723/j.issn.1671-167X.2024.06.014
抗磷脂抗体在白塞病合并血栓中的临床意义
李钰锴1, 王红彦1, 罗靓1,2, 李云1, 李春1,*( )
)
- 1. 北京大学人民医院风湿免疫科,北京 100044
2. 重庆市渝北区人民医院中医科,重庆 401120
Clinical significance of antiphospholipid antibodies in Behcet disease with thrombosis
Yukai LI1, Hongyan WANG1, Liang LUO1,2, Yun LI1, Chun LI1,*()
- 1. Department of Rheumatology and Immunology, Peking University People' s Hospital, Beijing 100044, China
2. Department of Traditional Chinese Medicine, the People' s Hospital of Yubei District of Chongqing, Chongqing 401120, China
摘要:
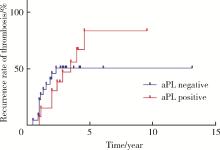
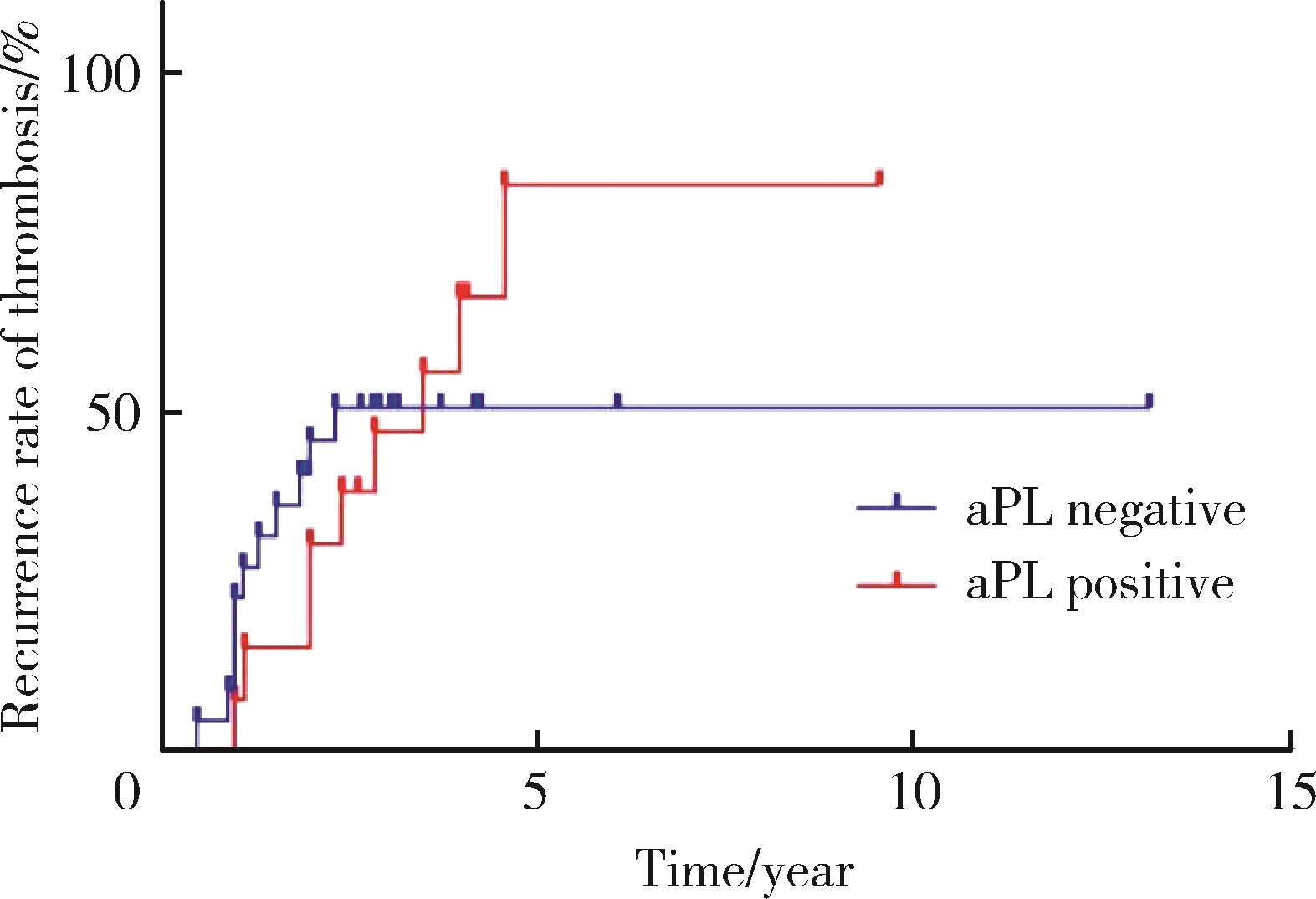
目的: 探讨抗磷脂抗体(antiphospholipid antibody, aPL)在白塞病(Behcet disease, BD)合并血栓中的分布及其临床意义。方法: 回顾性选取2008年2月至2024年7月于北京大学人民医院风湿免疫科住院的222例BD患者作为研究对象,收集患者的一般资料(包括年龄、性别等)、临床表现(包括口腔溃疡、生殖器溃疡和血栓等)、实验室指标[包括aPL、人类白细胞抗原(human leukocyte antigen, HLA)-B51、抗内皮细胞抗体等],随访合并血栓的BD患者血栓复发情况。使用卡方检验比较aPL阳性组和aPL阴性组患者的临床症状及实验室指标上的差异。使用Log-rank检验对aPL阳性组和aPL阴性组的血栓复发率进行比较,并用Two-stage方法进行P矫正,最后使用Graphpad prism进行绘图。结果: BD患者中,aPL单阳性、双阳性及三阳性患者的比例分别为22.1%、0.5% 和1.4%。抗心磷脂抗体、抗β2糖蛋白Ⅰ抗体和狼疮抗凝物(lupus anticoagulant, LAC)的阳性率分别为10.4%、1.8%和13.1%。aPL阳性组血栓的发生率显著高于aPL阴性组(44.9% vs. 16.9%, P < 0.001)。aPL阳性组的血红细胞沉降率[(20.78±4.91) mm/h vs. (15.85±4.29) mm/h, P=0.005]、C反应蛋白[(12.97±5.17) mg/L vs. (7.49±4.22) mg/L, P=0.010]和免疫球蛋白M [(1.55±0.95) g/L vs. (1.12±0.72) g/L, P < 0.001]显著高于aPL阴性组。LAC阳性是BD患者血栓发生的独立危险因素(OR=8.51, 95%CI: 2.71~26.72, P < 0.001)。aPL阳性组的血栓复发率高于aPL阴性组,但两组差异无统计学意义(69.23% vs. 52.17%, P=0.932)。结论: LAC阳性和动脉瘤是BD患者血栓形成的独立危险因素,aPL阳性也会显著增加BD患者血栓发生风险,对指导BD的治疗具有重要意义。
中图分类号:
- R593.2
| 1 |
Bulur I , Onder M . Behçet disease: New aspects[J]. Clin Dermatol, 2017, 35 (5): 421- 434.
doi: 10.1016/j.clindermatol.2017.06.004 |
| 2 |
Saadoun D , Wechsler B . Behçet' s disease[J]. Orphanet J Rare Dis, 2012, 7, 20.
doi: 10.1186/1750-1172-7-20 |
| 3 |
Shapouri-Moghaddam A , Tavakkol Afshari SJ , Rahimi HR , et al. Para-clinical and immunological evaluation in Buerger' s disease as a suspected autoimmune disease: Case series[J]. Rep Biochem Mol Biol, 2021, 9 (4): 379- 384.
doi: 10.52547/rbmb.9.4.379 |
| 4 |
El-Ageb EM , Al-Maini MH , Al-Shukaily AK , et al. Clinical features of Behçet' s disease in patients in the Sultanate of Oman: The significance of antiphospholipid antibodies?[J]. Rheumatol Int, 2002, 21 (5): 176- 181.
doi: 10.1007/s00296-001-0157-8 |
| 5 |
Espinosa G , Font J , Tàssies D , et al. Vascular involvement in Behçet' s disease: Relation with thrombophilic factors, coagulation activation, and thrombomodulin[J]. Am J Med, 2002, 112 (1): 37- 43.
doi: 10.1016/S0002-9343(01)01048-8 |
| 6 |
Calamia KT , Schirmer M , Melikoglu M . Major vessel involvement in Behçet ' s disease: An update[J]. Curr Opin Rheumatol, 2011, 23 (1): 24- 31.
doi: 10.1097/BOR.0b013e3283410088 |
| 7 | Lie JT . Vascular involvement in Behçet' s disease: Arterial and venous and vessels of all sizes[J]. J Rheumatol, 1992, 19 (3): 341- 343. |
| 8 |
Islam MA , Alam SS , Kundu S , et al. Prevalence of antiphospholipid antibodies in Behçet' s disease: A systematic review and meta-analysis[J]. PLoS One, 2020, 15 (1): e0227836.
doi: 10.1371/journal.pone.0227836 |
| 9 |
Le Joncour A , Martos R , Loyau S , et al. Critical role of neutrophil extracellular traps (NETs) in patients with Behcet' s disease[J]. Ann Rheum Dis, 2019, 78 (9): 1274- 1282.
doi: 10.1136/annrheumdis-2018-214335 |
| 10 |
Li C , Zuo Y , Zhang S , et al. Additional risk factors associated with thrombosis and pregnancy morbidity in a unique cohort of antiphospholipid antibody-positive patients[J]. Chin Med J (Engl), 2022, 135 (6): 658- 664.
doi: 10.1097/CM9.0000000000001964 |
| 11 |
Zhang X , Gong Z , Shen Y , et al. Alkaline ceramidase 1-mediated platelet ceramide catabolism mitigates vascular inflammation and abdominal aortic aneurysm formation[J]. Nat Cardiovasc Res, 2023, 2 (12): 1173- 1189.
doi: 10.1038/s44161-023-00364-1 |
| 12 |
Güngörer V , Polat MC , Çelikel E , et al. Factors associated with the development of thrombosis in pediatric Behçet disease[J]. J Clin Rheumatol, 2023, 29 (4): e19- e24.
doi: 10.1097/RHU.0000000000001930 |
| 13 | Hatemi G , Christensen R , Bang D , et al. 2018 update of the EULAR recommendations for the management of Behçet' s syndrome[J]. Ann Rheum Dis, 2018, 77 (6): 808- 818. |
| 14 |
Seyahi E . Phenotypes in Behçet' s syndrome[J]. Intern Emerg Med, 2019, 14 (5): 677- 689.
doi: 10.1007/s11739-019-02046-y |
| 15 | Bettiol A , Prisco D , Emmi G . Behçet: The syndrome[J]. Rheumatology (Oxford), 2020, 59 (Suppl 3): iii101- iii107. |
| [1] | 孟庆伟, 范梦, 郭煌达, 章涵宇, 王梦莹, 王斯悦, 彭和香, 王雪珩, 侯天姣, 秦雪英, 陈大方, 李劲, 武轶群, 吴涛, 陈洪波, 胡永华. 老年人心源性卒中抗凝治疗的预后[J]. 北京大学学报(医学版), 2026, 58(3): 536-542. |
| [2] | 魏慧, 张警丰, 姚中强, 赵金霞. 类风湿关节炎合并慢性病贫血患者的临床特征及相关因素[J]. 北京大学学报(医学版), 2026, 58(2): 307-312. |
| [3] | 赵杰, 付春, 赵秀娟, 薛海岩, 李纾, 王振洲, 朱凤雪. 胸部创伤患者在重症监护病房内发生呼吸机相关性肺炎的危险因素[J]. 北京大学学报(医学版), 2026, 58(2): 351-358. |
| [4] | 郭芷均, 俎明, 马超, 张贺军, 张静, 丁士刚. 同时性多发早期胃癌漏诊病灶的临床病理特征[J]. 北京大学学报(医学版), 2026, 58(2): 410-415. |
| [5] | 高雅静, 李正芳, 马梦思, 武丽君. SII和SIRI对白塞病葡萄膜炎的风险预测及疾病活动度和预后的评估[J]. 北京大学学报(医学版), 2025, 57(6): 1067-1073. |
| [6] | 董琪, 何菁, 贾园, 姚海红, 张霞. 模拟复发性多软骨炎的VEXAS综合征1例[J]. 北京大学学报(医学版), 2025, 57(6): 1180-1183. |
| [7] | 李博闻, 张强, 孙益鑫. 儿童及青年漏斗胸患者Nuss术后发生脊柱侧弯的风险预测模型建立及验证[J]. 北京大学学报(医学版), 2025, 57(5): 941-946. |
| [8] | 胡枫艺, 孟庆阳, 陈拿云, 王佳宁, 刘振龙, 马勇, 杨渝平, 龚熹, 王成, 刘平, 史尉利. 镜下内侧髌股复合体重建治疗伴高级别滑车发育不良复发性髌骨脱位的临床疗效[J]. 北京大学学报(医学版), 2025, 57(5): 947-955. |
| [9] | 杨小勇, 张帆, 马潞林, 刘承. 前列腺导管腺癌临床特征及腺外侵犯的影响因素[J]. 北京大学学报(医学版), 2025, 57(5): 956-960. |
| [10] | 缪祺, 洪保安, 张学舟, 孙志鹏, 王维, 王宇轩, 薄予轩, 赵佳晖, 张宁. 膀胱癌合并冠心病患者行经尿道膀胱肿瘤切除术围手术期抗血小板药物管理[J]. 北京大学学报(医学版), 2025, 57(4): 698-703. |
| [11] | 刘伟, 郭稳, 过哲, 李春艳, 李云龙, 刘思奇, 张亮, 宋慧. 痛风患者放射学阴性骨侵蚀的相关危险因素[J]. 北京大学学报(医学版), 2025, 57(4): 735-739. |
| [12] | 陆梦溪, 刘秋萍, 周恬静, 刘晓非, 孙烨祥, 沈鹏, 林鸿波, 唐迅, 高培. 基于社区人群队列的甘油三酯-葡萄糖指数与心血管病发病和死亡的关联[J]. 北京大学学报(医学版), 2025, 57(3): 430-435. |
| [13] | 杨龙傲, 金旭, 黄文初, 何丽华, 陈娟. 视屏作业人员视疲劳及干眼的流行病学调查[J]. 北京大学学报(医学版), 2025, 57(3): 554-561. |
| [14] | 郭华秋, 王哲, 杨雪, 白洁. 口腔急诊出血患者的临床特征与危险因素[J]. 北京大学学报(医学版), 2025, 57(1): 142-147. |
| [15] | 邓敏婷, 王楠, 夏斌, 赵玉鸣, 朱俊霞. 儿童及青少年挫入恒前牙自行再萌出的相关影响因素[J]. 北京大学学报(医学版), 2025, 57(1): 148-153. |
|
||
