北京大学学报(医学版) ›› 2018, Vol. 50 ›› Issue (6): 1004-1008. doi: 10.19723/j.issn.1671-167X.2018.06.011
我国西藏地区(高原)系统性红斑狼疮患者临床及免疫学特征分析
杨娇1,姚海红2,莫晓冬3,罗增1,白玛央金1,△( )
)
- 1. 西藏自治区人民医院风湿免疫科, 拉萨 850000
2. 北京大学人民医院风湿免疫科, 北京 100044
3. 北京大学人民医院血液科, 北京 100044
Clinical and immunological characteristics of patients with systemic lupus erythematosus in Tibet plateau, China
Jiao YANG1,Hai-hong YAO2,Xiao-dong MO3,Zeng LUO1,yang-jin Bai-ma1,△()
- 1. Department of Rheumatology and Immunology, Tibet Autonomous Region People’s Hospital, Lhasa 850000, China
2. Department of Rheumatology and Immunology, Peking University People’s Hospital, Beijing 100044, China
3. Department of Hemotology, Peking University People’s Hospital, Beijing 100044, China
摘要:
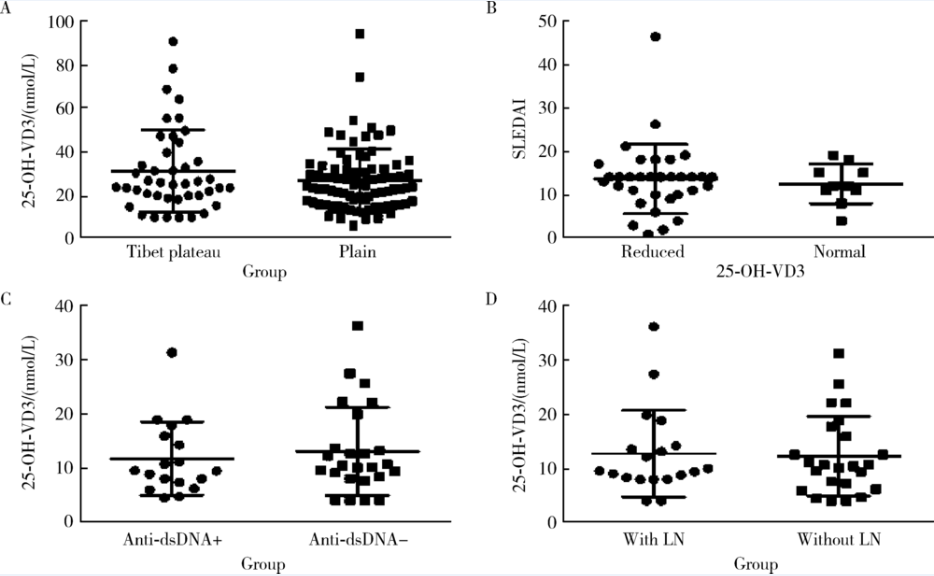
目的: 探讨我国西藏地区系统性红斑狼疮(systemic lupus erythematosus,SLE)患者发病特点、受累器官、免疫学特点。方法: 回顾性研究西藏自治区人民医院风湿免疫科2014年5月至2016年4月住院的SLE患者共70例,随机抽取北京大学人民医院风湿免疫科SLE数据库中120例年龄及性别匹配的住院SLE患者作为对照组,对比高原与平原地区SLE患者临床特点、受累器官、免疫学特点。结果: 西藏地区SLE患者男女比例1 :10.7,平原患者男女比例1 :11.0;高原患者发病年龄(33.2±11.4)岁,平原患者发病年龄(35.3±13.2)岁,两组发病年龄相当。首发临床症状方面,高原地区SLE患者以关节炎(78.6%)、脱发(55.7%)、颧部红斑(48.6%)为常见,其中关节炎、脱发发生率明显高于平原组(P<0.05);高原地区SLE患者70%出现血液系统受累,与平原地区类似;狼疮肾炎及狼疮脑病发生率均明显低于平原组(38.6% vs. 56.7%, 2.9% vs. 17.5%, P<0.05)。血清学方面,高原地区抗双链DNA(double-stranded DNA,dsDNA)抗体阳性率为57.1%,抗Smith(Sm)抗体(55.7%)、抗干燥综合征A(Sj?gren syndrome A, SSA)抗体(74.3%)、抗干燥综合征B(Sj?gren syndrome B, SSB)抗体(41.4%)及抗u1核糖核蛋白(u1-ribosenuclear protein,u1RNP)抗体(45.7%)阳性率均显著高于平原地区患者(P<0.05);分别有61.4%、38.6%的高原SLE患者出现补体C3、C4减低,显著低于平原患者(P<0.05)。SLE疾病活动度指数(SLE disease activity index,SLEDAI)评分在两组间差异无统计学意义(高原组为12.19±5.58,平原组为12.69±7.28)。此外,西藏地区SLE患者合并陈旧结核或者活动结核病13例(18.6%),慢性乙型肝炎或携带者7例(10%)。高原组SLE患者血清25羟维生素D3(25-dihydroxy-vitamin D3, 25-OH-VD3)减低者少于平原组(76.7% vs. 90.0%,P=0.046),血清25-OH-VD3水平高原组为(31.14±18.74) nmol/L,平原组为(26.91±14.27) nmol/L,两组间差异无统计学意义(P=0.16)。结论: 西藏地区SLE患者首发临床症状以关节炎、脱发、颧部红斑最为常见,其中关节炎、脱发发生率显著高于平原地区;狼疮肾炎及狼疮脑病发生率明显低于平原;多种自身抗体的阳性率显著高于平原地区。在年龄、性别构成、SLEDAI评分方面与平原地区类似,血清25-OH-VD3减低者平原组多于高原组,但25-OH-VD3水平在两组间无明显差异。
中图分类号:
- R593.241

| [1] | 中华医学会风湿病学分会. 系统性红斑狼疮诊断及治疗指南[J]. 中华风湿病学杂志, 2010,14(5):342-346. |
| [2] | Hochberg MC . Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus[J]. Arthritis Rheum, 1997,40(9):1725. |
| [3] |
Bombardier C, Gladman DD, Urowitz MB , et al. Derivation of the SLEDAI. A disease activity index for lupus patients. The Committee on Prognosis Studies in SLE[J]. Arthritis Rheum, 1992,35(6):630-640.
doi: 10.1002/(ISSN)1529-0131 |
| [4] | WS288—2008, 中华人民共和国卫生行业标准:肺结核诊断[S]. |
| [5] | WS299—2008, 中华人民共和国卫生行业标准:乙型病毒性肝炎诊断标准[S]. |
| [6] |
Li M, Zhang W, Leng X , et al. Chinese SLE Treatment and Research group (CSTAR) registry: Ⅰ. Major clinical characteristics of Chinese patients with systemic lupus erythematosus[J]. Lupus, 2013,22(11):1192-1199.
doi: 10.1177/0961203313499086 pmid: 23963101 |
| [7] |
Zhang S, Su J, Li X , et al. Chinese SLE Treatment and Research group (CSTAR) registry: Ⅴ. gender impact on Chinese patients with systemic lupus erythematosus[J]. Lupus, 2015,24(12):1267-1275.
doi: 10.1177/0961203315585813 pmid: 25972364 |
| [8] |
胡莉娜, 吴丽娟, 古宇 , 等. 地震伤员藏族人群在急进平原治疗前后红细胞及相关参数的分析[J]. 国际检验医学杂志, 2012,33(2):174-175.
doi: 10.3969/j.issn.1673-4130.2012.02.019 |
| [9] | 胡海燕, 王亚魁, 张志刚 . 中医治疗高原脱发120例疗效观察[J]. 西藏科技, 2002(10):52. |
| [10] | 罗洋, 杜华, 杨桂兰 , 等. 红景天治疗高原性脱发的临床研究[J]. 西北国防医学杂志, 2015,36(12):808-810. |
| [11] |
Kuhn A, Beissert S . Photosensitivity in lupus erythematosus[J]. Autoimmunity, 2005,38(7):519-529.
doi: 10.1080/08916930500285626 |
| [12] |
Foltyn VN, Golan TD . In vitro ultraviolet irradiation induces pro-inflammatory responses in cells from premorbid SLE mice[J]. Lupus, 2001,10(4):272-283.
doi: 10.1191/096120301680416968 pmid: 11341104 |
| [13] |
Ni JD, Yao X, Pan HF , et al. Clinical and serological correlates of anti-Sm autoantibodies in Chinese patients with systemic lupus erythematosus: 1 584 cases[J]. Rheumatol Int, 2009,29(11):1323-1326.
doi: 10.1007/s00296-009-0855-1 pmid: 19194707 |
| [14] |
黄菁梅, 李小冬, 谭焕源 , 等. 系统性红斑狼疮患者抗u1RNP抗体检测的临床意义[J]. 临床肺科杂志, 2010,15(5):734-735.
doi: 10.3969/j.issn.1009-6663.2010.05.078 |
| [15] |
罗靓, 何英 . 狼疮脑病的临床治疗概述[J]. 中国中医急症, 2017,26(1):91-94.
doi: 10.3969/j.issn.1004-745X.2017.01.028 |
| [16] | 平措卓玛. 2010 年西藏自治区结核病监测资料分析[J]. 疾病监测, 2013 ( 4):269-271. |
| [17] | 陈红梅, 国杰, 胡凤梅 . 2011—2013年西藏自治区结核病流行特征分析[J]. 现代预防医学, 2015,42(16):2887-2889. |
| [1] | 马豆豆, 马晓彩, 常天静, 王丽芳, 丁艳, 石连杰. 临床表现似系统性红斑狼疮的大B细胞淋巴瘤骨髓受累1例[J]. 北京大学学报(医学版), 2026, 58(3): 666-669. |
| [2] | 汤晓菲, 丁秋玲, 张阳, 王育梅, 田美伊, 孙卓, 王荣荣, 陈妍, 刘坚. 阿伐曲泊帕治疗难治性系统性红斑狼疮相关血小板减少1例[J]. 北京大学学报(医学版), 2026, 58(2): 405-409. |
| [3] | 李欣艺, 赵金霞, 穆荣. 阿司匹林对系统性红斑狼疮妊娠者结局的影响[J]. 北京大学学报(医学版), 2025, 57(6): 1074-1080. |
| [4] | 王晓林, 郭邵逸, 陈大召, 温锡杰, 华勇, 张亮, 张秦. 全髋关节置换术治疗系统性红斑狼疮继发股骨头缺血性坏死的随访研究[J]. 北京大学学报(医学版), 2025, 57(6): 1081-1088. |
| [5] | 卫春, 杨月, 赵新菊, 刘栩, 贾园. 系统性红斑狼疮合并自身免疫性郎飞结病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1174-1179. |
| [6] | 梁景原, 张霞, 姚海红. 误诊为系统性硬化症的POEMS综合征1例[J]. 北京大学学报(医学版), 2025, 57(6): 1184-1187. |
| [7] | 赵凯, 鲁芙爱, 王永福. 中枢神经系统感染模拟神经精神狼疮1例[J]. 北京大学学报(医学版), 2025, 57(6): 1188-1192. |
| [8] | 王小梦, 曾晓君, 李娟. 黎族与汉族系统性红斑狼疮患者的主要临床特征[J]. 北京大学学报(医学版), 2025, 57(6): 1213-1218. |
| [9] | 曹沛, 栾庆先. 牙周炎与全身系统性疾病的思考与探索[J]. 北京大学学报(医学版), 2025, 57(5): 852-858. |
| [10] | 袁显墩, 李照华, 徐丹, 李婷, 方丹, 穆荣. 丝氨酸蛋白酶23在系统性硬化病皮肤纤维化中的作用和机制[J]. 北京大学学报(医学版), 2025, 57(5): 903-910. |
| [11] | 王文琼, 侯玉珂, 李春, 张学武. 系统性红斑狼疮患者不良妊娠结局的预测因素[J]. 北京大学学报(医学版), 2025, 57(3): 599-603. |
| [12] | 王红彦, 李鑫铭, 房柯池, 朱华群, 贾汝琳, 王晶. 系统性红斑狼疮疾病活动度相关特征分析及评估模型的构建[J]. 北京大学学报(医学版), 2024, 56(6): 1017-1022. |
| [13] | 陈丹丹, 李云, 卢情怡, 相晓红, 孙峰, 李英妮, 赵静, 王红彦, 李春. 育龄期系统性红斑狼疮患者卵巢功能的评价及其影响因素[J]. 北京大学学报(医学版), 2024, 56(6): 1023-1028. |
| [14] | 王莉, 高超, 任欢欢, 沈艳平, 黄晓玮, 姚鸿, 韩丹丹. 系统性红斑狼疮患者自我管理能力现状及相关因素分析[J]. 北京大学学报(医学版), 2024, 56(6): 1029-1035. |
| [15] | 潘苇, 李云, 罗俊佳, 李春, 叶华, 李雪, 贾园. 系统性硬化症患者新型冠状病毒感染特点及疫苗接种效果:一项单中心队列研究[J]. 北京大学学报(医学版), 2024, 56(6): 1041-1046. |
|
||
