北京大学学报(医学版) ›› 2018, Vol. 50 ›› Issue (6): 1078-1082. doi: 10.19723/j.issn.1671-167X.2018.06.024
鼻喷右美托咪定在儿童口腔门诊全身麻醉前的镇静效果
高玲( ),刘云,杨旭东
),刘云,杨旭东
- 北京大学口腔医学院·口腔医院,麻醉科 国家口腔疾病临床医学研究中心 口腔数字化医疗技术和材料国家工程实验室 口腔数字医学北京市重点实验室, 北京 100081
Effects of intranasal dexmedetomidine for children undergoing dental rehabilitation under general anesthesia: a double-blinded randomized controlled trial
Ling GAO(),Yun LIU,Xu-dong YANG
- Department of Anesthesiology, Peking University School and Hospital of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
摘要:
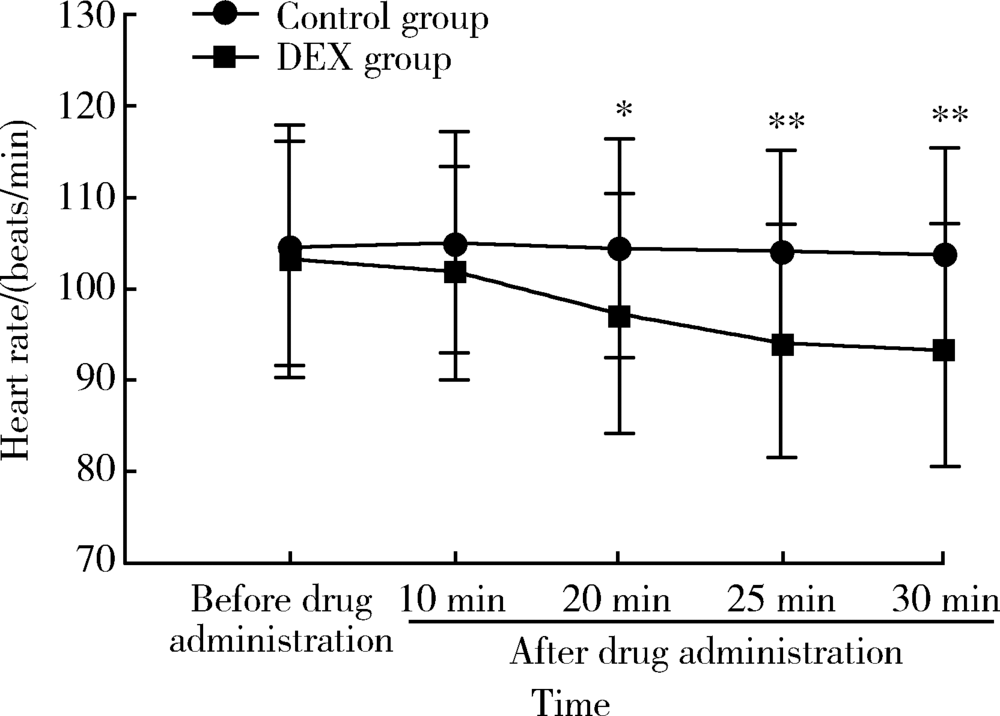
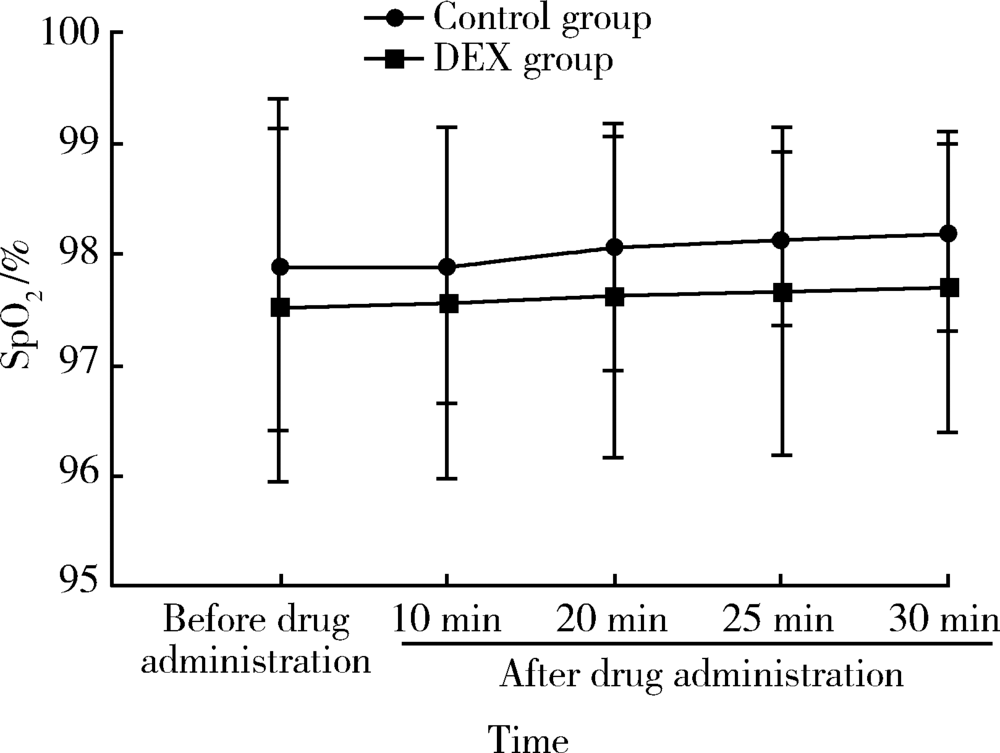
目的: 观察全身麻醉下牙病治疗患儿鼻喷右美托咪定(dexmedetomidine,DEX)对术前紧张情绪、父母分离焦虑、面罩接受程度和术后躁动的影响。方法: 选择北京大学口腔医院儿童口腔门诊全身麻醉下牙病治疗的患儿60例,年龄2~9岁,随机分为2组:对照组术前30 min经鼻喷入生理盐水0.02 mL/kg,DEX组喷入DEX 2 μg/kg(药物使用原液)。观察和记录患儿给药前及给药后10、20、25、30 min的心率(heart rate,HR)、脉搏血氧饱和度(oxygen saturation,SpO2)以及给药30 min后的Ramsay镇静评分、分离焦虑评分、面罩吸入诱导接受度评分和术后躁动评分及并发症的情况。结果: 两组患儿的年龄、体重、性别构成、手术时间、拔管时间和苏醒时间相似,差异无统计学意义。DEX组患儿与父母的分离焦虑、面罩接受程度明显优于对照组(56.7% vs. 26.7%,73.3% vs. 40%,P均<0.05),术后躁动评分在两组间差异无统计学意义(P>0.05)。与对照组相比,DEX组患儿给药20 min后HR有所下降,差异有统计学意义[(97.13±12.93)次/min vs. (104.53±11.97)次/min, P<0.05]。两组患儿的SpO2未见明显差异,且均未见心动过缓、低氧血症的发生。结论: 全身麻醉前经鼻喷入DEX可以产生良好的术前镇静作用,改善与父母的分离焦虑,提高面罩接受度。两组患儿苏醒质量高,无明显的苏醒期躁动、呼吸抑制等并发症。鼻喷DEX 2 μg/kg是一种安全有效的儿童术前给药方式。
中图分类号:
- R782.05



| [1] |
夏斌, 秦满, 马文利 , 等. 693例儿童全身麻醉下牙齿治疗的特征分析[J]. 北京大学学报(医学版), 2013,45(6):984-988.
doi: 10.3969/j.issn.1671-167X.2013.06.032 |
| [2] |
Kain ZN, Mayes LC , O’Connor TZ, et al. Preoperative anxiety in children. Predictors and outcomes[J]. Arch Pediatr Adolesc Med, 1996,150(12):1238-1245.
doi: 10.1001/archpedi.1996.02170370016002 |
| [3] |
Wstson AT, Visram A . Children’s preoperative anxiety and postoperative behavior[J]. Paediatr Anaesth, 2003,13(3):188-204.
doi: 10.1046/j.1460-9592.2003.00848.x pmid: 12641680 |
| [4] |
Wolfe TR, Braude DA . Intranasl medication delivery for children: A brief review and update[J]. Pediatrics, 2010,126(3):532-537.
doi: 10.1542/peds.2010-0616 pmid: 20696726 |
| [5] |
Peng K, Wu SR, Ji FH , et al. Premedication with dexmedetomidine in pediatric patients: a systematic review and meta-analysis[J]. Clinics, 2014,69(11):777-786.
doi: 10.6061/clinics/2014(11)12 pmid: 4255070 |
| [6] |
Piao G, Wu J . Systematic assessment of dexmedetomidine as an anesthetic agent: a meta-analysis of randomized controlled trials[J]. Arch Med Sci, 2014,10(1):19-24.
doi: 10.5114/aoms.2014.40730 pmid: 3953974 |
| [7] |
Kuang H, Johnson JA, Mulqueen JM , et al. The efficacy of benzodiazepines as acute anxiolytics in children: A meta-analysis[J]. Depress Anxiety, 2017,34(10):888-896.
doi: 10.1002/da.22643 pmid: 28504861 |
| [8] |
Deshmukh PV, Kulkami SS, Parchandekar MK , et al. Comparison of preanesthetic sedation in pediatric patients with oral and intranasal midazolam[J]. J Anaesthesiol Clin Pharmacol, 2016,32(3):353-358.
doi: 10.4103/0970-9185.168205 pmid: 5009843 |
| [9] |
Iirola T, Vilo S, Manner T , et al. Bioavailability of dexmedetomidine after intranasal administration[J]. Eur J Clin Pharmacol, 2011,67(8):825-831.
doi: 10.1007/s00228-011-1002-y |
| [10] |
Lee Y, Kim J, Kim S , et al. Intranasal administration of dexmedetomidine (DEX) as a premedication for pediatric patients undergoing general anesthesia for dental treatment[J]. J Dent Anesth Pain Med, 2016,16(1):25-29.
doi: 10.17245/jdapm.2016.16.1.25 pmid: 5564115 |
| [11] |
Sheta SA, Al-Sarheed MA, Abdelhalim AA . Intranasal dexmedetomidine vs. midazolam for premedication in children undergoing complete dental rehabilitation: a double-blinded randomized controlled trial[J]. Pediatric Anesth, 2014,24(2):181-189.
doi: 10.1111/pan.12287 pmid: 24237879 |
| [12] |
Yuen VM, Irwin MG, Hui TW , et al. A double-blind, crossover assessment of the sedative and analgesic effects of intranasal dexmedetomidine[J]. Anesth Analg, 2007,105(2):374-380.
doi: 10.1213/01.ane.0000269488.06546.7c pmid: 17646493 |
| [13] |
Yuen VM, Hui TW, Irwin MG , et al. Optimal timing for the administration of intranasal dexmedetomidine for premedication in children[J]. Anaesthesia, 2010,65(9):922-929.
doi: 10.1111/j.1365-2044.2010.06453.x |
| [14] |
Yuen VM, Hui TW, Irwin MG , et al. A randomised comparison of two intranasal dexmedetomidine doses for premedication in children[J]. Anaesthesia, 2012,67(11):1210-1216.
doi: 10.1111/j.1365-2044.2012.07309.x pmid: 22950484 |
| [15] |
Yuen VM, Hui TW, Irwin MG , et al. A comparison of intranasal dexmedetomidine and oral midazolam for premedication in pediatric anesthesia: a double-blinded randomized controlled trial[J]. Anesth Analg, 2008,106(6):1715-1721.
doi: 10.1213/ane.0b013e31816c8929 pmid: 18499600 |
| [16] |
Wolfe TR, Bemstone T . Intranasal drug delivery: An alternative to intravenous administration in selected emergency cases[J]. J Emerg Nurs, 2004,30(2):141-147.
doi: 10.1016/j.jen.2004.01.006 |
| [17] |
Talon MD, Woodson LC, Sherwood ER , et al. Intranasal dexmedetomidine premedication is comparable with midazolam in burn children undergoing reconstructive surgery[J]. J Burn Care Res, 2009,30(4):599-605.
doi: 10.1097/BCR.0b013e3181abff90 pmid: 19506498 |
| [18] |
Jun JH, Kim KN, Kim JY , et al. The effects of intranasal dexmedetomidine premedication in children: a systematic review and meta-analysis[J]. Can J Anaesth, 2017,64(9):947-961.
doi: 10.1007/s12630-017-0917-x pmid: 28639236 |
| [19] |
Kain ZN, Caldwell-Andrews AA, Maranets I , et al. Predicting which child-parent pair will benefit from parental presence during induction of anesthesia: A decision-making approach[J]. Anesth Analg, 2006,102(1):81-84.
doi: 10.1213/01.ANE.0000181100.27931.A1 pmid: 16368808 |
| [1] | 李宗瀚, 黄洋阅, 李宁, 李明磊, 宋宏程, 张潍平, 刘超. 国产单孔蛇形臂机器人手术系统在儿童肾盂成形术中的应用[J]. 北京大学学报(医学版), 2025, 57(4): 662-665. |
| [2] | 赵兆, 张维宇, 杨文博, 张勇杰, 张晓鹏, 赵慧颖, 周刚, 王强. 低龄、低体重儿童肾移植2例[J]. 北京大学学报(医学版), 2025, 57(4): 803-807. |
| [3] | 张依航, 蔡珊, 陈子玥, 刘云飞, 党佳佳, 师嫡, 李佳欣, 黄天彧, 宋逸. 基于RE-AIM框架儿童青少年近视与肥胖共病综合干预实施性研究结局指标的构建[J]. 北京大学学报(医学版), 2025, 57(3): 436-441. |
| [4] | 唐孟利, 刘扬, 秦冉, 郭欣, 李宏田. 我国10省幼儿园5~6岁儿童近视和近视前期流行特征[J]. 北京大学学报(医学版), 2025, 57(3): 442-447. |
| [5] | 刘光旭, 张良, 赵厚宇, 邓思危, 杨君婷, 李宁, 马瑞, 何艳, 许国章, 刘志科, 詹思延. 2015—2021年宁波市6岁以下儿童热性惊厥的流行病学特征[J]. 北京大学学报(医学版), 2025, 57(3): 584-591. |
| [6] | 李琳, 廖津津. 应用ROC曲线评估久坐行为对儿童青少年视力不良的预测价值[J]. 北京大学学报(医学版), 2025, 57(3): 614-619. |
| [7] | 王紫薇, 李闵, 高慧, 邓芳. 链球菌感染与过敏性紫癜肾炎患儿肾损害的相关性[J]. 北京大学学报(医学版), 2025, 57(2): 284-290. |
| [8] | 邓敏婷, 王楠, 夏斌, 赵玉鸣, 朱俊霞. 儿童及青少年挫入恒前牙自行再萌出的相关影响因素[J]. 北京大学学报(医学版), 2025, 57(1): 148-153. |
| [9] | 孙宁, 王学文, 武勇, 任爽, 李恒, 杜辉, 龚晓峰. 拇外翻术中局部应用氨甲环酸缓解术后肿胀的早期疗效[J]. 北京大学学报(医学版), 2025, 57(1): 172-177. |
| [10] | 杨颖婷, 李若竹, 窦桂丽, 雷玥, 夏斌. iRoot BP Plus用于年轻恒牙外伤部分牙髓切断治疗的临床随机对照研究[J]. 北京大学学报(医学版), 2024, 56(6): 1083-1088. |
| [11] | 赵双云, 邹思雨, 李雪莹, 沈丽娟, 周虹. 中文版口腔健康素养量表简版(HeLD-14)在学龄前儿童家长中应用的信度和效度评价[J]. 北京大学学报(医学版), 2024, 56(5): 828-832. |
| [12] | 陈心心, 唐哲, 乔艳春, 荣文笙. 北京市密云区4岁儿童患龋状况及其与龋活跃性检测的相关性[J]. 北京大学学报(医学版), 2024, 56(5): 833-838. |
| [13] | 岳芷涵,韩娜,鲍筝,吕瑾莨,周天一,计岳龙,王辉,刘珏,王海俊. 儿童早期体重指数轨迹与超重风险关联的前瞻性队列研究[J]. 北京大学学报(医学版), 2024, 56(3): 390-396. |
| [14] | 费秀文,刘斯,汪波,董爱梅. 成人及儿童组织坏死性淋巴结炎临床特征及治疗[J]. 北京大学学报(医学版), 2024, 56(3): 533-540. |
| [15] | 俞光岩. 儿童唾液腺疾病[J]. 北京大学学报(医学版), 2024, 56(1): 1-3. |
|
||
