北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (5): 931-936. doi: 10.19723/j.issn.1671-167X.2019.05.023
正畸牙齿位置的移动对角化龈宽度的影响
王高南1,焦剑2,周彦恒1,施捷1,△( )
)
- 1. 北京大学口腔医学院·口腔医院,正畸科 国家口腔疾病临床医学研究中心 口腔数字化医疗技术和材料国家工程实验室 口腔数字医学北京市重点实验室,北京 100081
2. 北京大学口腔医学院·口腔医院,牙周科 国家口腔疾病临床医学研究中心 口腔数字化医疗技术和材料国家工程实验室 口腔数字医学北京市重点实验室,北京 100081
Effect of orthodontic tooth movement on keratinized gingival width
Gao-nan WANG1,Jian JIAO2,Yan-heng ZHOU1,Jie SHI1,△()
- 1. Department of Orthodontics, Peking University School and Hospital of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
2. Department of Periodontology, Peking University School and Hospital of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
摘要:
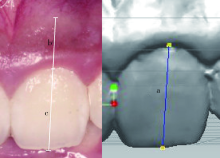
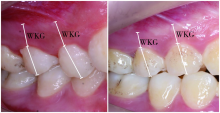
目的:通过测量28例患者正畸治疗前后角化龈宽度的变化以及牙齿位置的变化,分析正畸牙齿移动与角化龈宽度变化的关系。方法:对患者照片与模型进行匹配,通过测量牙冠长度而获得角化龈的宽度。在rapidform 2006上将治疗前后的上颌模型重叠,准确测量正畸移动前后牙齿(包括切牙、尖牙、前磨牙)的位置变化。统计牙齿压低伸长、内收与唇向移动、转矩变化与角化龈宽度的计量数据,分析其变化的关系。结果:对28例患者共213颗牙齿治疗前后数据的相关性进行分析发现,牙齿转矩角度的变化与角化龈宽度的变化有较强相关性(r=-0.47,P<0.001),并在多水平线性回归分析中验证了它们之间的相关性(回归系数<0,P<0.001),同时,牙齿内收和压低与角化龈宽度的变化没有显著相关性(P>0.05),尖牙和前磨牙回归系数为负(尖牙回归系数=-0.35,前磨牙回归系数=-0.38,P<0.05)。结论:正畸过程中的牙齿移动对角化龈的宽度会造成影响,唇向正转矩的增加更有可能引起角化龈宽度的减小;牙齿内收和压低与角化龈宽度的变化没有显著相关性;切牙相对于尖牙和前磨牙,在牙齿移动过程中更容易发生角化龈宽度的变化。正畸过程中,应该对牙齿位置变化可能对角化龈宽度造成的影响进行预判,关注角化龈宽度的变化。
中图分类号:
- R783.5




| [1] | Closs LQ, Branco P, Rizzatto SD , et al. Gingival margin alterations and the pre-orthodontic treatment amount of keratinized gingiva[J]. Braz Oral Res, 2007,21(1):58-63. |
| [2] | Coatoam GW, Behrents RG, Bissada NF . The width of keratinized gingiva during orthodontic treatment: its significance and impact on periodontal status[J]. J Periodontol, 1981,52(6):307-313. |
| [3] | Trentini CM, Moriarty JD, Phillips C , et al. Evaluation of the use of orthodontic records to measure the width of keratinized tissue[J]. J Periodontol, 1995,66(6):438-442. |
| [4] | Melsen B, Allais D . Factors of importance for the development of dehiscences during labial movement of mandibular incisors: a retrospective study of adult orthodontic patients [J]. Am J Orthod Dentofacial Orthop, 2005, 127(5): 552-561; quiz 625. |
| [5] | Wyrębek B, Orzechowska A, Cudziło D , et al. Evaluation of changes in the width of gingival in children and youth[J]. Dev Period Med, 2015,19(2):212-216. |
| [6] | Cho MY, Choi JH, Lee SP , et al. Three-dimensional analysis of the tooth movement and arch dimension changes in Class I malocclusions treated with first premolar extractions: A guideline for virtual treatment planning[J]. Am J Orthod Dentofacial Orthop, 2010,138(6):747-757. |
| [7] | Artun J, Krogstad O . Periodontal status of mandibular incisors following excessive proclination. A study in adults with surgically treated mandibular prognathism[J]. Am J Orthod Dentofacial Orthop, 1987,91(3):225-232. |
| [8] | Dorfman HS . Mucogingival changes resulting from mandibular incisor tooth movement[J]. Am J Orthod, 1978,74(3):286-297. |
| [9] | Djeu G, Hayes C, Zawaideh S . Correlation between mandibular central incisor proclination and gingival recession during fixed appliance therapy[J]. Angle Orthod, 2002,72(3):238-245. |
| [10] | Dannan A, Darwish MA, Sawan MN . Keratinized gingiva width alteration during orthodontic alignment and leveling phase; a preliminary investigation [J/OL]. Int J Dent Sci, 1995, 7(2): 1-6[2018-01-31]. |
| [11] | King KO, Sadler JF, Higgason JD , et al. The effects of angulation upon pre- and postoperative photographs[J]. J Periodontol, 1963,34(2):139-141. |
| [12] | Erkan M, Pikdoken L, Usumez S . Gingival response to mandibular incisor intrusion[J]. Am J Orthod Dentofacial Orthop, 2007, 132(2): 143. e9-13. |
| [13] | Pikdoken L, Erkan M, Usumez S . Gingival response to mandibular incisor extrusion[J]. Am J Orthod Dentofacial Orthop, 2009, 135(4): 432. e1-6. |
| [14] | Zawawi KH, Al-Harthi SM, Al-Zahrani MS . Prevalence of gingival biotype and its relationship to dental malocclusion[J]. Saudi Med J, 2012,33(6):671-675. |
| [15] | Zawawi KH, Al-Zahrani MS . Gingival biotype in relation to incisors’ inclination and position[J]. Saudi Med J, 2014,35(11):1378-1383. |
| [1] | 戴帆帆,刘怡,许天民,陈贵. 探索成人正畸前后下颌三维数字化模型的重叠方法[J]. 北京大学学报(医学版), 2018, 50(2): 271-278. |
| [2] | 沈潇,施捷,徐莉,焦剑,路瑞芳,孟焕新. 伴错牙合畸形的侵袭性牙周炎患者牙周-正畸联合治疗的临床评价[J]. 北京大学学报(医学版), 2017, 49(1): 60-066. |
| [3] | 温馥嘉,陈贵,刘怡. 基于锥形束CT的强支抗内收上前牙病例牙根及牙槽骨的形态学分析[J]. 北京大学学报(医学版), 2016, 48(4): 702-708. |
| [4] | 黄俊强, 刘施瑶, 江久汇. Tweed-Merrifield技术矫治成人严重双颌前突的疗效评价[J]. 北京大学学报(医学版), 2016, 48(3): 555-561. |
| [5] | 孙翔宇, 袁超, 丁鹏, 刘磊, 荣文笙, 郑树国, 徐韬, 司燕. 不同氟制剂预防正畸治疗中釉质脱矿的临床评价[J]. 北京大学学报(医学版), 2015, 47(4): 724-727. |
| [6] | 宋广瀛, 姜若萍, 张晓芸, 刘思琦, 于潇楠, 陈青, 翁萱蓉, 五味子, 苏红, 任翀, 单儒楷, 耿直, 许天民, 建立中国正畸疗效评价标准课题组. 正畸疗效主、客观评价方法的有效性[J]. 北京大学学报(医学版), 2015, 47(1): 90-97. |
| [7] | 潘一春, 赵健慧. 腭中部微种植钉支抗系统的临床效果评价[J]. 北京大学学报(医学版), 2014, 46(6): 969-974. |
| [8] | 李巍然. 唇腭裂正畸治疗研究的新进展[J]. 北京大学学报(医学版), 2014, 46(1): 1-4. |
| [9] | 冯光耀, 邹冰爽, 高雪梅, 曾祥龙, 王秀婧, 阎燕. 正畸拔除下颌第二双尖牙对下颌第三磨牙角度的影响[J]. 北京大学学报(医学版), 2013, 45(1): 77-80. |
| [10] | 魏松, 李晶, 周彦恒. 安氏Ⅱ类病例下颌第二前磨牙拔除后下牙列生理性漂移的三维模型分析[J]. 北京大学学报(医学版), 2013, 45(1): 81-86. |
| [11] | 刘思琦, 沈刚, 白丁, 周洪, 厉松, 陈文静, 王大为7, 李巍然, 耿直8, 许天民. 中国正畸专家对错牙合畸形严重程度的主观判断一致性研究[J]. 北京大学学报(医学版), 2012, 44(1): 98-102. |
| [12] | 宋广瀛, 李巍然, 耿直, 许天民. 正畸疗效满意度主观评价一致性的探讨[J]. 北京大学学报(医学版), 2012, 44(1): 103-107. |
| [13] | 赵宁宁, 林久祥, 陈智滨, 刘妍. 正畸保持期龈沟液骨保护素/核因子kappa B受体活化因子配体水平对牙槽骨改建状态的意义[J]. 北京大学学报(医学版), 2012, 44(1): 108-112. |
| [14] | 李小彤, 张东妹, 杨雁琪. 影响口腔正畸治疗患者下颌第三磨牙状态改变的因素分析[J]. 北京大学学报(医学版), 2011, 43(2): 267-271. |
| [15] | 赵健慧, 丁云. 骨性Ⅱ类错成人与少年治疗前后骨骼变化的对比[J]. 北京大学学报(医学版), 2010, 42(5): 578-581. |
|
||
