北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (4): 704-709. doi: 10.19723/j.issn.1671-167X.2021.04.014
经皮肾镜术中不同憩室颈部处理方式治疗肾盏憩室结石的长期预后
戴翔,左美妮,张晓鹏,胡浩( ),徐涛
),徐涛
- 北京大学人民医院泌尿外科,北京 10044
Comparison of long-term outcomes in different managements of diverticular neck in percutaneous nephrolithotomy for diverticular calculi
DAI Xiang,ZUO Mei-ni,ZHANG Xiao-peng,HU Hao(),XU Tao
- Department of Urology, Peking University People’s Hospital, Beijing 100044, China
摘要:
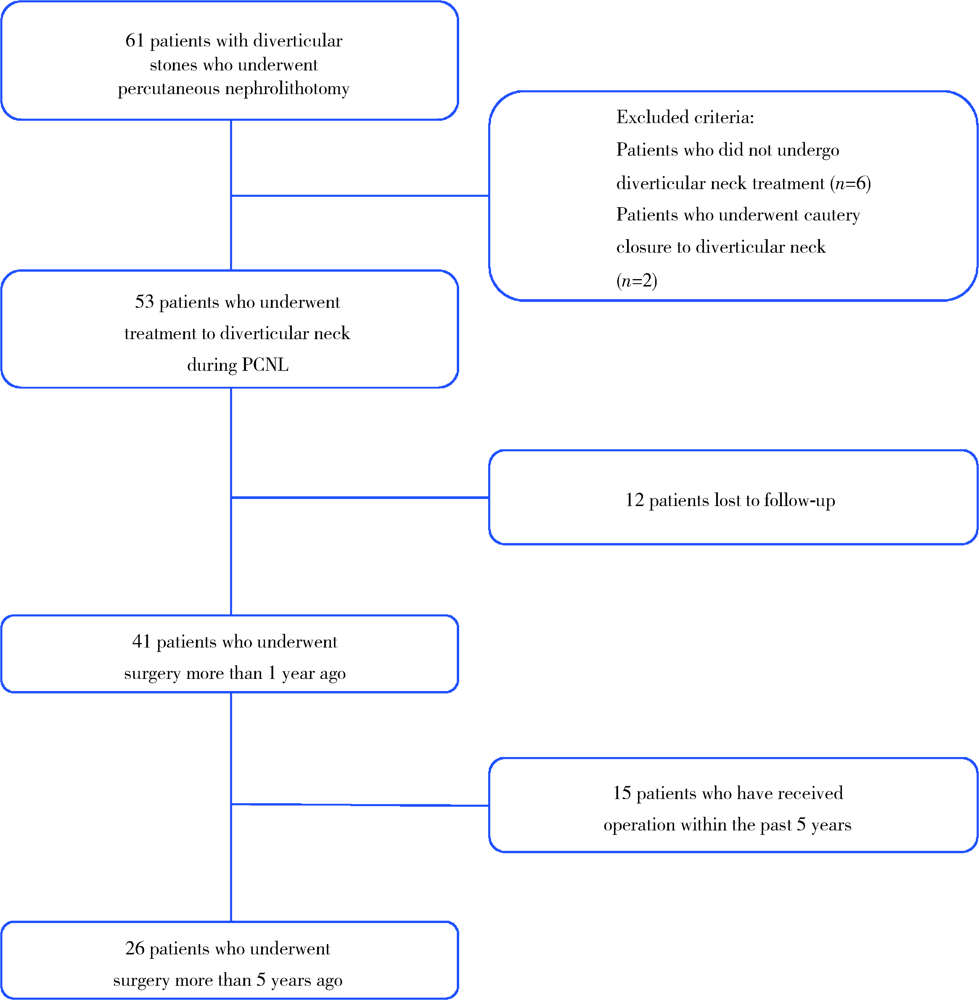
目的: 比较经皮肾镜术中切开法与扩张法两种不同处理憩室颈部的方式治疗肾盏憩室结石的长期预后。方法: 选择2009年6月至2019年1月在北京大学人民医院经皮肾镜取石术治疗肾盏憩室结石患者的临床资料进行回顾性分析,记录年龄、性别、体重指数(body mass index,BMI)、美国麻醉师协会(American Society of Anesthesiology, ASA)分级和术前症状等患者基本情况,结石位置、大小等结石特征数据,皮肾通道长度、手术时长等手术相关数据,以及术后血红蛋白下降幅度、Clavien并发症分级、无石率等围手术期临床资料,并进行了5年以上的长期随访。结果: 53例患者纳入本研究,根据术中处理憩室颈部方式的不同分为扩张组(n=37)和切开组(n=16), 其中男性患者24例(45.3%), 女性29例(54.7%),平均年龄为(39.96±12.88)岁,大多数憩室结石位于肾上极(n=32,60.38%)和背侧(n=41,77.4%),以单发结石为主(n=36,67.9%),两组间人口学数据及结石特征数据除年龄及结石负荷外差异无统计学意义。45例(84.9%)患者术后达到无石状态,44例(83.0%)患者术后症状得到改善。术后12例患者失访,41例患者的平均随访时间为77个月。在术后1年时有1例出现复发。截止2021年3月,15例患者术后随访未满5年,剩余26例术后5年复发率为34.6%。两组患者围手术期并发症发生率、术后无石率及复发率差异均无统计学意义,术后5年复发率均较术后1年时明显升高,保持无石状态和残石状态患者所占比例明显下降。结论: 经皮肾镜处理憩室结石术中切开法和扩张法处理憩室颈部均可达到令人满意的术后无石率,术后5年时憩室结石复发率为30%~40%。
中图分类号:
- R692.4

| [1] |
Waingankar N, Hayek S, Smith AD, et al. Calyceal diverticula: a comprehensive review [J]. Rev Urol, 2014, 16(1):29-43.
pmid: 24791153 |
| [2] |
Parkhomenko E, Tran T, Thai J, et al. Percutaneous management of stone containing calyceal diverticula: associated factors and outcomes [J]. J Urol, 2017, 198(4):864-868.
doi: S0022-5347(17)60624-4 pmid: 28483573 |
| [3] | Dretler S. A new useful endourologic classification of calyceal diverticula [J]. J Endourol, 1992, 6:6. |
| [4] |
McGarry L, Sahadev R, Hogan G, et al. Calyceal diverticula in children: laparoscopic marsupialization is the optimal intervention [J]. J Pediatr Urol, 2020, 16(2): 221.e1-221.e6.
doi: 10.1016/j.jpurol.2020.01.014 |
| [5] |
Bas O, Ozyuvali E, Aydogmus Y, et al. Management of calyceal diverticular calculi: a comparison of percutaneous nephrolithotomy and flexible ureterorenoscopy [J]. Urolithiasis, 2015, 43(2):155-161.
doi: 10.1007/s00240-014-0725-5 |
| [6] |
Turna B, Raza A, Moussa S, et al. Management of calyceal diverticular stones with extracorporeal shock wave lithotripsy and percutaneous nephrolithotomy: long-term outcome [J]. BJU Int, 2007, 100(1):151-156.
doi: 10.1111/bju.2007.100.issue-1 |
| [7] | Yang H, Yao X, Tang C, et al. Flexible Ureterorenoscopy management of calyceal diverticular calculi [J]. Urol J, 2019, 16(1):12-15. |
| [8] | Zhang JQ, Wang Y, Zhang JH, et al. Retrospective analysis of ultrasound-guided flexible ureteroscopy in the management of calyceal diverticular calculi [J]. Chin Med J (Engl), 2016, 129(17):2067-2073. |
| [9] | Elsamra S, Motato H, Friedlander J, et al. 1 675 percutaneous treatment of calyceal diverticulum: access, stone extraction, and fulguration [J]. J Urol, 2013, 189(4):e689. |
| [10] |
Boonyapalanant C, Saksirisampant P, Taweemonkongsap T, et al. Factors impacting stone-free rate after retrograde intrarenal surgery for calyceal diverticular calculi [J]. Res Rep Urol, 2020, 12:345-350.
doi: 10.2147/RRU.S265959 pmid: 32903933 |
| [11] | 王强, 孙家庆, 晁亮, 等. 经皮肾镜超声碎石清石联合自制钩状电极一期治疗肾盏憩室结石 [J]. 中华腔镜泌尿外科杂志:电子版, 2013, 7(1):33-36. |
| [12] |
Donnellan SM, Harewood LM, Webb DR. Percutaneous management of caliceal diverticular calculi: technique and outcome [J]. J Endourol, 1999, 13(2):83-88.
pmid: 10213100 |
| [1] | 田聪,刘军,杨波,乔佳佳,黄晓波,许清泉. 经皮肾镜取石术中异常肾盂黏膜活检结果分析[J]. 北京大学学报(医学版), 2023, 55(5): 948-952. |
| [2] | 高健,胡立宝,陈尘,郅新,徐涛. 经皮肾镜去石术后出血的介入治疗[J]. 北京大学学报(医学版), 2020, 52(4): 667-671. |
| [3] | 王明瑞,王起,胡浩,赖金惠,贺永新,熊杰,刘献辉,刘士军,许克新,徐涛. 标准通道经皮肾镜取石术治疗孤立肾肾结石的长期安全性和有效性[J]. 北京大学学报(医学版), 2020, 52(4): 663-666. |
| [4] | 谌诚,张博,韩文科,林健,王刚,张晓春,宋毅,赵峥,张中元,金杰,虞巍. 超声造影技术引导下经皮肾穿刺应用于经皮肾镜取石术的单中心初步经验[J]. 北京大学学报(医学版), 2017, 49(6): 1071-1075. |
| [5] | 陈亮, 李建兴, 黄晓波, 杨波, 王佳, 王晓峰. 肾结石合并肾功能不全患者围手术期尿微量白蛋白与尿肌酐比值检测及意义[J]. 北京大学学报(医学版), 2011, 43(5): 757-760. |
|
||
