北京大学学报(医学版) ›› 2022, Vol. 54 ›› Issue (1): 113-118. doi: 10.19723/j.issn.1671-167X.2022.01.018
两种硅酸钙类材料用于成熟恒牙牙髓切断术的临床效果
钱锟,潘洁,朱文昊,赵晓一,刘畅,雍颹( )
)
- 北京大学口腔医学院·口腔医院综合科,国家口腔医学中心,国家口腔疾病临床医学研究中心,口腔数字化医疗技术和材料国家工程实验室,口腔数字医学北京市重点实验室,国家卫生健康委员会口腔医学计算机应用工程技术研究中心,国家药品监督管理局口腔生物材料重点实验室,北京 100081
Evaluation of bioceramic putty repairmen iRoot and mineral trioxide aggregate in mature permanent teeth pulpotomy
QIAN Kun,PAN Jie,ZHU Wen-hao,ZHAO Xiao-yi,LIU Chang,YONG Wei()
- Department of General Dentistry, Peking University School and Hospital of Stomatology & National Center of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology & NHC Research Center of Engineering and Technology for Computerized Dentistry & NMPA Key Laboratory for Dental Materials, Beijing 100081, China
摘要:
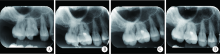
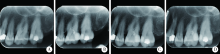
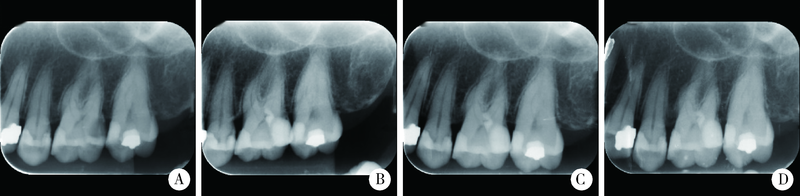
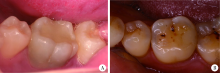
目的: 评价两种硅酸钙类材料——生物陶瓷材料iRoot和三氧化矿物凝聚体(mineral trioxide aggregate, MTA)在成熟恒牙牙髓切断治疗中的应用效果。方法: 选择2017 年 11月至2019 年9 月在北京大学口腔医院综合科就诊患者,对龋源性露髓的成熟恒前磨牙、磨牙行牙髓切断术,随机分组,使用iRoot(iRoot组,n=22)和MTA(MTA组,n=21)作为盖髓剂,并分别于术后3、6、12个月通过临床检查(温度测试和电活力测试)及影像学检查评价临床疗效。对患者、评价者采用盲法,但由于两种盖髓剂性状有明显差异,因此对实施治疗者(接诊医师)未能采用盲法。结果: 两组患者的性别、平均年龄、牙列及牙位分布差异均无统计学意义(P>0.05)。术后12个月随访时失访7例(iRoot组4例,MTA组3例)。两组各有1例在3个月复查时出现一过性敏感,而在6个月复查时牙髓活力正常。iRoot组有1例在12个月复查时出现一过性敏感。两组12个月随访时的成功率均为100%,治愈率分别为94.4%(iRoot组)及100%(MTA组), 差异无统计学意义(P>0.05)。iRoot组无病例发生明显的牙冠变色,而MTA组有3例患牙出现明显牙冠变色。结论: 12个月观察期内, iRoot用于成熟恒牙活髓保存治疗取得与MTA相似的令人满意的临床效果;iRoot不易造成治疗后牙齿变色且操作便利,因此拥有更好的临床应用前景。
中图分类号:
- R781.3

| [1] |
Duncan HF, Galler KM, Tomson PL, et al. European society of endodontology position statement: management of deep caries and the exposed pulp[J]. Int Endod J, 2019: 52(7):923-934.
doi: 10.1111/iej.13080 pmid: 30664240 |
| [2] | 董艳梅. 活髓保存治疗与生物活性盖髓剂的临床现状与研究[J]. 中华口腔医学杂志, 2014, 49(5):268-271. |
| [3] | 高学军, 岳林. 牙体牙髓病学[M]. 北京: 北京大学医学出版社, 2013: 367-368. |
| [4] |
Linsuwanont P, Wimonsutthikul K, Pothimoke U, et al. Treatment outcomes of mineral trioxide aggregate pulpotomy in vital permanent teeth with carious pulp exposure: the retrospective study[J]. J Endod, 2017, 43(2):225-230.
doi: S0099-2399(16)30754-3 pmid: 28041685 |
| [5] |
Taha NA, Khazali MA. Partial pulpotomy in mature permanent teeth with clinical signs indicative of irreversible pulpitis: a randomized clinical trial[J]. J Endod, 2017, 43(9):1417-1421.
doi: 10.1016/j.joen.2017.03.033 |
| [6] | 韦曦, 凌均棨. 直接盖髓术的现代理念与临床进展[J]. 中华口腔医学杂志, 2019, 54(9):577-583. |
| [7] |
Kulan P, Karabiyik O, Kose GT, et al. The effect of accelerated mineral trioxide aggregate on odontoblastic differentiation in dental pulp stem cell niches[J]. Int Endod J, 2018, 51(7):758-766.
doi: 10.1111/iej.12747 pmid: 28117904 |
| [8] |
Yoon JH, Choi SH, Koh JT, et al. Hard tissue formation after direct pulp capping with osteostatin and MTA in vivo[J]. Restor Dent Endod, 2021, 46(2):e17.
doi: 10.5395/rde.2021.46.e17 |
| [9] |
Liu S, Wang S, Dong Y. Evaluation of a bioceramic as a pulp capping agent in vitro and in vivo[J]. J Endod, 2015, 41(5):652-657.
doi: 10.1016/j.joen.2014.12.009 |
| [10] |
Komabayashi T, Zhu Q, Eberhart R, et al. Current status of direct pulp-capping materials for permanent teeth[J]. Dent Mater J, 2016, 35(1):1-12.
doi: 10.4012/dmj.2015-013 pmid: 26830819 |
| [11] |
Mahgoub N, Alqadasi B, Aldhorae K, et al. Comparison between iRoot BP Plus (EndoSequence root repair material) and mineral trioxide aggregate as pulp-capping agents: a systematic review[J]. J Int Soc Prev Community Dent, 2019, 9(6):542-552.
doi: 10.4103/jispcd.JISPCD_249_19 pmid: 32039073 |
| [12] |
Asgary S, Hassanizadeh R, Torabzadeh H, et al. Treatment outcomes of 4 vital pulp therapies in mature molars[J]. J Endod, 2018, 44(4):529-535.
doi: S0099-2399(17)31301-8 pmid: 29397215 |
| [13] |
Taha NA, Ahmad MB, Ghanim A. Assessment of mineral trioxide aggregate pulpotomy in mature permanent teeth with carious exposures[J]. Int Endod J, 2017, 50(2):117-125.
doi: 10.1111/iej.12605 pmid: 26715408 |
| [14] |
Shi S, Bao ZF, Liu Y, et al. Comparison of in vivo dental pulp responses to capping with iRoot BP Plus and mineral trioxide aggregate[J]. Int Endod J, 2016, 49(2):154-160.
doi: 10.1111/iej.12439 pmid: 25661049 |
| [15] |
Parirokh M, Torabinejad M, Dummer PMH. Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview-part Ⅰ: vital pulp therapy[J]. Int Endod J, 2018, 51(2):177-205.
doi: 10.1111/iej.12841 pmid: 28836288 |
| [16] |
Javid B, Panahandeh N, Torabzadeh H, et al. Bioactivity of endodontic biomaterials on dental pulp stem cells through dentin[J]. Restor Dent Endod, 2019, 45(1):e3.
doi: 10.5395/rde.2020.45.e3 |
| [17] |
Liu Y, Liu XM, Bi J, et al. Cell migration and osteo/odontogenesis stimulation of iRoot FS as a potential apical barrier material in apexification[J]. Int Endod J, 2020, 53(4):467-477.
doi: 10.1111/iej.13237 pmid: 31622505 |
| [18] |
Lu J, Li Z, Wu X, et al. iRoot BP Plus promotes osteo/odontogenic differentiation of bone marrow mesenchymal stem cells via MAPK pathways and autophagy[J]. Stem Cell Res Ther, 2019, 10(1):222.
doi: 10.1186/s13287-019-1345-3 |
| [19] |
ElReash AA, Hamama H, Eldars W, et al. Antimicrobial activity and pH measurement of calcium silicate cements versus new bioactive resin composite restorative material[J]. BMC Oral Health, 2019, 19(1):235.
doi: 10.1186/s12903-019-0933-z pmid: 31684929 |
| [20] |
Öncel Torun Z, Torun D, Demirkaya K, et al. Effects of iRoot BP and white mineral trioxide aggregate on cell viability and the expression of genes associated with mineralization[J]. Int Endodontic J, 2015, 48(10):986-993.
doi: 10.1111/iej.2015.48.issue-10 |
| [21] |
Zhang J, Zhu LX, Cheng X, et al. Promotion of dental pulp cell migration and pulp repair by a bioceramic putty involving FGFR-mediated signaling pathways[J]. J Dent Res, 2015, 94(6):853-862.
doi: 10.1177/0022034515572020 pmid: 25724555 |
| [22] |
Peskersoy C, Lukarcanin J, Turkun M. Efficacy of different cal-cium silicate materials as pulp-capping agents: randomized clinical trial[J]. J Dent Sci, 2021, 16(2):723-731.
doi: 10.1016/j.jds.2020.08.016 pmid: 33854725 |
| [23] |
Qudeimat MA, Barrieshi-Nusair KM, Owais AI. Calcium hydro-xide vs. mineral trioxide aggregates for partial pulpotomy of permanent molars with deep caries[J]. Eur Arch Paediatr Dent, 2007, 8(2):99-104.
doi: 10.1007/BF03262577 |
| [24] |
Kang C, Kim S, Shin Y, et al. A randomized controlled trial of ProRoot MTA, OrthoMTA and RetroMTA for pulpotomy in primary molars[J]. Oral Dis, 2015, 21(6):785-791.
doi: 10.1111/odi.12348 pmid: 25970794 |
| [25] | 丁美丽, 秦满, 郑佳佳, 等. 新型生物陶瓷材料用于年轻恒牙牙髓切断术的效果评价[J]. 口腔医学研究, 2018, 34(7):766-770. |
| [26] | Yang Y, Xia B, Xu Z, et al. The effect of partial pulpotomy with iRoot BP Plus in traumatized immature permanent teeth: a rando-mized prospective controlled trial[J]. Dent Traumatol, 2020, 36(5):518-525. |
| [27] | 雷玥, 杨颖婷, 战园. 生物陶瓷材料在乳牙牙髓切断术中的应用[J]. 北京大学学报(医学版), 2019, 51(1):70-74. |
| [28] |
Azimi S, Fazlyab M, Sadri D, et al. Comparison of pulp response to mineral trioxide aggregate and a bioceramic paste in partial pulpotomy of sound human premolars: a randomized controlled trial[J]. Int Endod J, 2014, 47(9):873-881.
doi: 10.1111/iej.12231 pmid: 24330490 |
| [29] |
Zanini M, Hennequin M, Cousson PY. A review of criteria for the evaluation of pulpotomy outcomes in mature permanent teeth[J]. J Endod, 2016, 42(8):1167-1174.
doi: 10.1016/j.joen.2016.05.008 |
| [30] |
Simon S, Perard M, Zanini M, et al. Should pulp chamber pulpotomy be seen as a permanent treatment? Some preliminary thoughts[J]. Int Endod J, 2013, 46(1):79-87.
doi: 10.1111/j.1365-2591.2012.02113.x pmid: 22900881 |
| [31] |
Kunert GG, Kunert IR, da Costa Filho LC, et al. Permanent teeth pulpotomy survival analysis: retrospective follow-up[J]. J Dent, 2015, 43(9):1125-1131.
doi: 10.1016/j.jdent.2015.06.010 |
| [32] | Mass E, Zilberman U. Long-term radiologic pulp evaluation after partial pulpotomy in young permanent morlars[J]. Quintessence Int, 2011, 42(7):547-554. |
| [1] | 杨颖婷, 李若竹, 窦桂丽, 雷玥, 夏斌. iRoot BP Plus用于年轻恒牙外伤部分牙髓切断治疗的临床随机对照研究[J]. 北京大学学报(医学版), 2024, 56(6): 1083-1088. |
| [2] | 郑佳佳,杨雪,温泉,付元,邵校,丁美丽. 生物活性陶瓷iRoot BP Plus®在儿童年轻恒前牙复杂冠折牙髓切断术中的应用[J]. 北京大学学报(医学版), 2024, 56(1): 179-184. |
| [3] | 赵晓一,刘畅,钱锟,潘洁. 成熟恒牙牙髓切断术的疗效及影像学评价[J]. 北京大学学报(医学版), 2024, 56(1): 138-143. |
| [4] | 雍颹,钱锟,朱文昊,赵晓一,刘畅,潘洁. 成年恒牙牙髓切断后牙髓钙化的X线片评价[J]. 北京大学学报(医学版), 2023, 55(1): 88-93. |
| [5] | 王爽,彭楚芳,刘鹤. 新型生物陶瓷材料用于乳磨牙牙髓切断术的临床疗效[J]. 北京大学学报(医学版), 2022, 54(6): 1196-1201. |
| [6] | 雷玥,杨颖婷,战园. 生物陶瓷材料在乳牙牙髓切断术中的应用[J]. 北京大学学报(医学版), 2019, 51(1): 70-74. |
| [7] | 李爽,张清. 玷污层对新型三氧化矿物凝聚体根尖封闭性的影响[J]. 北京大学学报(医学版), 2018, 50(3): 560-563. |
| [8] | 窦桂丽,吴南,赵双云,夏斌. 乳磨牙牙髓切断术两年疗效观察及其影响因素回顾性分析[J]. 北京大学学报(医学版), 2018, 50(1): 170-175. |
| [9] | 郭怡丹,张笋. Er:YAG激光用于比格犬牙髓切断术[J]. 北京大学学报(医学版), 2016, 48(4): 714-719. |
| [10] | 郑佳佳,陈小贤,张笋,葛立宏. 中日两国部分口腔医师乳牙活髓保存诊疗操作现况调查[J]. 北京大学学报(医学版), 2015, 47(6): 1050-1052. |
| [11] | 白洁, 秦满, 姬爱平. Pulpdent Multi-Cal用于年轻恒前牙活髓切断术的临床研究[J]. 北京大学学报(医学版), 2011, 43(6): 882-885. |
|
||
