北京大学学报(医学版) ›› 2022, Vol. 54 ›› Issue (6): 1123-1127. doi: 10.19723/j.issn.1671-167X.2022.06.011
唾液腺超声对干燥综合征的诊断价值
刘杨,程昉,王艳玲,艾香艳,朱振航,赵福涛*( )
)
- 上海交通大学医学院附属第九人民医院风湿免疫科, 上海 201999
Diagnostic performances of salivary gland ultrasonography for Sjögren's syndrome
Yang LIU,Fang CHENG,Yan-ling WANG,Xiang-yan AI,Zhen-hang ZHU,Fu-tao ZHAO*()
- Department of Rheumatology and Immunology, the Ninth People's Hospital, Shanghai Jiaotong University School of Medicine, Shanghai 201999, China
摘要:
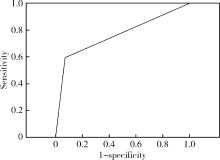
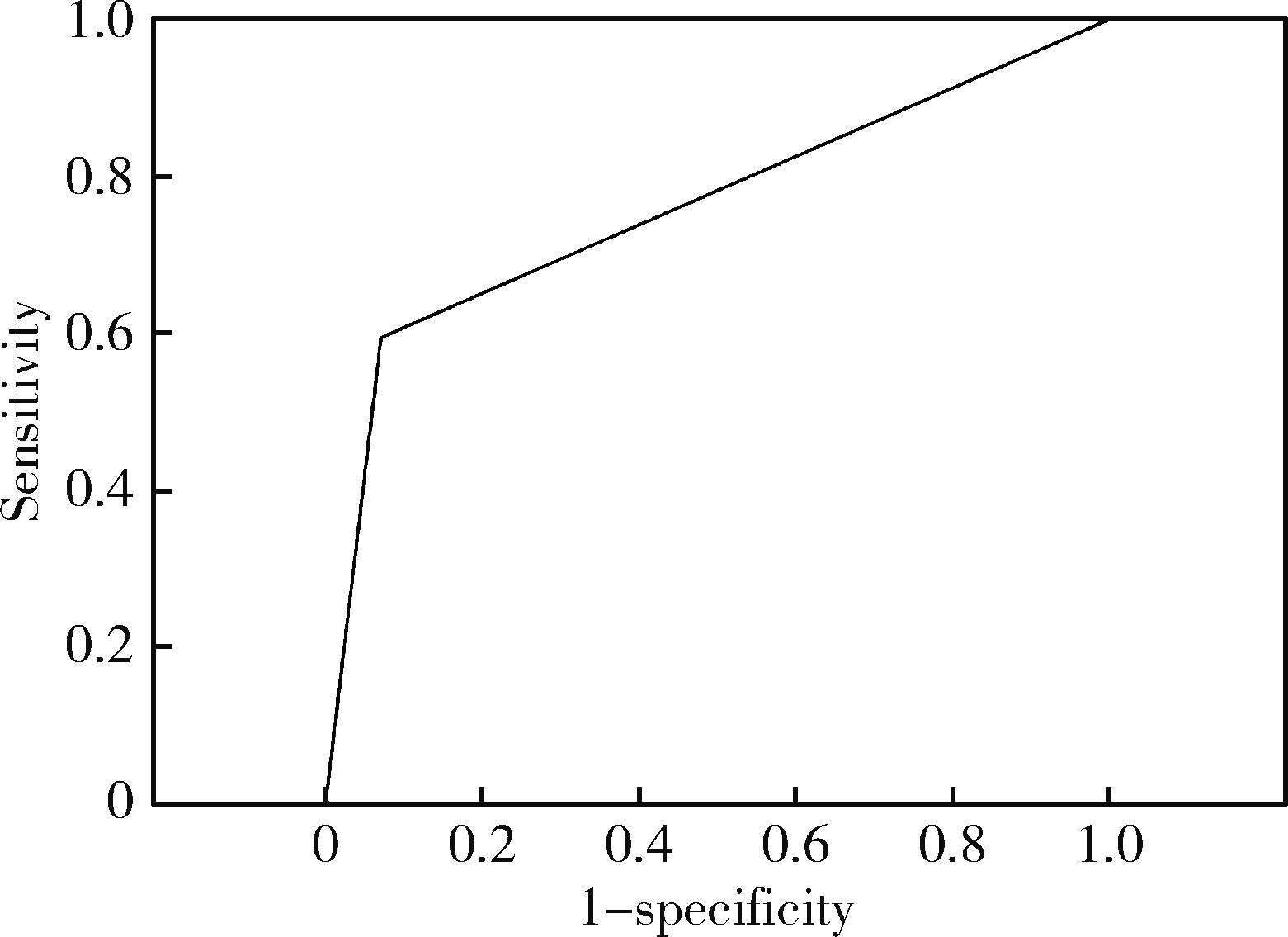
目的: 评估唾液腺超声(salivary gland uhrasonography,SGUS)对干燥综合征(Sj?gren’s syndrome,SS)的诊断价值。方法: 收集2019年12月至2022年1月就诊于上海交通大学医学院附属第九人民医院风湿免疫科门诊及住院部的246例表现为口干和/或眼干燥的患者,均完善SGUS,并采用2019年风湿病临床试验结果指标(outcome measures in rheumatology clinical trial,OMERACT)工作组超声评分系统对患者唾液腺进行评分,记录患者一般资料、未刺激唾液流率(unstimulated saliva flow rate, USFR)、Schirmer试验及血清学检查结果,193例完善唇腺活检检查。采用2016年美国风湿病学会(American College of Rheumatology,ACR)/欧洲抗风湿病联盟(European League Against Rheumatism,EULAR)共识作为SS诊断金标准。采用χ2检验比较两组唾液腺超声评分的差异,用受试者工作特征(receiver operating characteristic,ROC)曲线评估SGUS诊断SS的准确性,并比较SS患者中SGUS阳性组与阴性组的临床特征。结果: 共175例患者符合2016年ACR/EULAR共识为SS组,余71例不符合ACR/EULAR共识为非SS患者,两组患者年龄[(54.2±11.8)岁 vs.(53.4±14.9)岁,P=0.705]、女性(94.4% vs.93.1%,P=1.000)比较差异均无统计学意义。共109例患者SGUS阳性(≥2分),其中104例符合SS诊断,5例不符合SS诊断,SS组SGUS阳性率明显高于非SS组(59.4% vs.7.0%,P < 0.001)。2019年OMERACT超声评分系统诊断SS的曲线下面积为0.762(95%CI 0.701~0.823),SGUS评分与ACR/EULAR共识的绝对一致性为69.1%(170/246),敏感性为59.4%(104/175),特异性为93.0%(66/71),阳性预测值为95.4%(104/109),阴性预测值为48.2% (66/137)。共81例患者SGUS、抗干燥综合征A (Sj?gren’s syndrome A, SSA)抗体双阳性,均符合ACR/EULAR共识,阳性符合率为100%(81/81);85例患者SGUS阴性且无抗SSA抗体,60例未达到ACR/EULAR共识,阴性符合率为70.6% (60/85)。在SS患者中,SGUS阳性组有更高的抗核抗体(antinuclear antibody, ANA)阳性率(83.1%对98.1%,P < 0.001)。结论: 2019年OMERACT超声评分系统在诊断SS中有重要价值,与抗SSA抗体联合可进一步提高诊断性能。
中图分类号:
- R593.2
| 1 |
Shiboski CH , Shiboski SC , Seror R , et al. 2016 American College of Rheumatology/European League Against Rheumatism classification criteria for primary Sjögren's syndrome: A consensus and data-driven methodology involving three international patient cohorts[J]. Arthritis Rheumatol, 2017, 69 (1): 35- 45.
doi: 10.1002/art.39859 |
| 2 |
Theander E , Mandl T . Primary Sjögren's syndrome: Diagnostic and prognostic value of salivary gland ultrasonography using a simplified scoring system[J]. Arthritis Care Res (Hoboken), 2014, 66 (7): 1102- 1107.
doi: 10.1002/acr.22264 |
| 3 |
Salaffi F , Carotti M , Iagnocco A , et al. Ultrasonography of salivary glands in primary Sjögren's syndrome: A comparison with contrast sialography and scintigraphy[J]. Rheumatology (Oxford), 2008, 47 (8): 1244- 1249.
doi: 10.1093/rheumatology/ken222 |
| 4 | Lee KA , Lee SH , Kim HR , et al. Diagnostic and predictive eva-luation using salivary glandultrasonography in primary Sjögren's syndrome[J]. Clin Exp Rheumatol, 2018, 112 (3): 165- 172. |
| 5 |
Jousse-Joulin S , Gatineau F , Baldini C , et al. Weight of salivary gland ultrasonography compared toother items of the 2016 ACR/EULAR classification criteria for Primary Sjögren's syndrome[J]. J Intern Med, 2020, 287 (2): 180- 188.
doi: 10.1111/joim.12992 |
| 6 |
van Nimwegen JF , Mossel E , Delli K , et al. Incorporation of salivary gland ultrasonography into the ACR EULAR criteria for primary Sjögren's syndrome[J]. Arthritis Care Res (Hoboken), 2020, 72 (4): 583- 590.
doi: 10.1002/acr.24017 |
| 7 |
Takagi Y , Nakamura H , Sumi M , et al. Combined classification system based on ACR/EULAR and ultrasonographic scores for improving the diagnosis of Sjögren's syndrome[J]. PLoS One, 2018, 13 (4): e0195113.
doi: 10.1371/journal.pone.0195113 |
| 8 |
Jousse-Joulin S , D'Agostino MA , Nicolas C , et al. Video clip assessment of a salivary gland ultrasound scoring system in Sjögren's syndrome using consensual definitions: An OMERACT uhrasound working group reliability exercise[J]. Ann Rheum Dis, 2019, 78 (7): 967- 973.
doi: 10.1136/annrheumdis-2019-215024 |
| 9 |
Zhou M , Song S , Wu S , et al. Diagnostic accuracy of salivary gland ultrasonography with different scoring systems in Sjögren's syndrome: A systematic review and meta-analysis[J]. Sci Rep, 2018, 8 (1): 17128.
doi: 10.1038/s41598-018-35288-5 |
| 10 | Ramsubeik K , Motilal S , Sanchez-Ramos L , et al. Diagnostic accuracy of salivary gland ultrasound in Sjögren's syndrome: A systematic review and meta-analysis[J]. Ther Adv Musculoskelet Dis, 2020, 12, 1- 21. |
| 11 |
Jousse-Joulin S , Milic V , Jonsson MV , et al. Is salivary gland ultrasonography a useful tool in Sjögren's syndrome? A systematic review[J]. Rheumatology (Oxford), 2016, 55 (5): 789- 800.
doi: 10.1093/rheumatology/kev385 |
| 12 | Carotti M , Sala F , Di Carlo M , et al. Diagnostic value of major salivary gland ultrasonography in primary Sjögren's syndrome: The role of grey-scale and colour/power Doppler sonography[J]. Gland Surg, 2019, 8 (Suppl 3): S159- S167. |
| 13 |
Mossel E , Arends S , van Nimwegen JF , et al. Scoring hypoechogenic areas in one parotid and one submandibular gland increases feasibility of ultrasound in primary Sjögren's syndrome[J]. Ann Rheum Dis, 2018, 77 (4): 556- 562.
doi: 10.1136/annrheumdis-2017-211992 |
| 14 |
Izzetti R , Fulvio G , Nisi M , et al. Reliability of OMERACT scoring system in ultra-high frequency ultrasonography of minor salivary glands: Inter-rater agreement study[J]. J Imaging, 2022, 8 (4): 111.
doi: 10.3390/jimaging8040111 |
| 15 |
Al Tabaa O , Gouze H , Hamroun S , et al. Normal salivary gland ultrasonography could rule out the diagnosis of Sjögren's syndrome in anti-SSA-negative patients with sicca syndrome[J]. RMD Open, 2021, 7 (1): e001503.
doi: 10.1136/rmdopen-2020-001503 |
| 16 |
Fana V , Dohn UM , Krabbe S , et al. Application of the OMERACT grey-scale ultrasound scoring system for salivary glands in a single-centre cohort of patients with suspected Sjögren's syndrome[J]. RMD Open, 2021, 7 (2): e001516.
doi: 10.1136/rmdopen-2020-001516 |
| 17 | Robin F, Albert JD, Lescoat A, et al. Diagnostic performances of ultrasound evaluation of major salivary glands according to the 2019 OMERACT US scoring system[J/OL]. Arthritis Care Res (Hoboken), 2021, 5 (2021-05-10)[2022-04-15]. https://onlinelibrary.wiley.com/doi/10.1002/acr.24631. |
| 18 |
Gazeau P , Cornec D , Jousse-Joulin S , et al. Time-course of ultrasound abnormalities of major salivary glands in suspected Sjögren's syndrome[J]. Joint Bone Spine, 2018, 85 (2): 227- 232.
doi: 10.1016/j.jbspin.2017.02.007 |
| 19 | Zandonella-Callegher S , Zabotti A , Giovannini I , et al. Normal-appearing salivary gland ultrasonography identifies a milder phenotype of primary Sjögren's syndrome[J]. Front Med (Lausanne), 2020, 7, 602354. |
| 20 |
Mossel E , Delli K , Nimwegen GF , et al. Ultrasonography of major salivary glands compared with parotid and labial gland biopsy and classification criteria in patients with clinically suspected primary Sjögren's syndrome[J]. Ann Rheum Dis, 2017, 76 (11): 1883- 1889.
doi: 10.1136/annrheumdis-2017-211250 |
| 21 |
Kim JW , Lee H , Park SH , et al. Salivary gland ultrasonography findings are associated with clinical, histological, and serologic features of Sjögren's syndrome[J]. Scand J Rheumatol, 2018, 47 (4): 303- 310.
doi: 10.1080/03009742.2017.1374451 |
| 22 |
Jousse-Joulin S , Devauchelle-Pensec V , Cornec D , et al. Brief report: Ultrasonographic assessment of salivary gland response to rituximab in primary Sjögren's syndrome[J]. Arthritis Rheumatol, 2015, 67 (6): 1623- 1628.
doi: 10.1002/art.39088 |
| 23 |
Lorenzon M , Spina E , Di Franco FT , et al. Salivary gland ultrasound in primary Sjögren's syndrome: Current and future perspectives[J]. Open Access Rheumatol, 2022, 14, 147- 160.
doi: 10.2147/OARRR.S284763 |
| [1] | 杨静, 许晓韵, 郑丹妮, 凌晓彤, 屈留洋, 柳登高. 544例慢性唾液腺炎的临床与影像学特点及病因分析[J]. 北京大学学报(医学版), 2026, 58(3): 650-657. |
| [2] | 丛馨, 苏家增, 吴立玲, 丁冲, 李巍, 俞光岩. 唾液腺非肿瘤性疾病诊治研究进展[J]. 北京大学学报(医学版), 2026, 58(1): 1-9. |
| [3] | 杨雨婷, 屈留洋, 郑丹妮, 凌晓彤, 许晓韵, 柳登高. 1 812例唾液腺结石患者的人口学特征和临床特点[J]. 北京大学学报(医学版), 2026, 58(1): 153-159. |
| [4] | 汤易, 赵雪竹, 杨旭, 贾惠梅, 刘云松. 超声洁治对种植修复基台螺丝扭矩的影响[J]. 北京大学学报(医学版), 2026, 58(1): 84-88. |
| [5] | 刘源, 石桂秀. 干燥综合征到干燥病的命名变迁[J]. 北京大学学报(医学版), 2025, 57(6): 1015-1017. |
| [6] | 林文灏, 谢阳, 王芳晴, 王淑盈, 刘香君, 胡凡磊, 贾园. 基于B细胞单细胞转录组测序的干燥综合征分子分型[J]. 北京大学学报(医学版), 2025, 57(6): 1032-1041. |
| [7] | 向钊, 杨莉, 杨静. 非靶向代谢组学揭示原发性干燥综合征血小板减少患者血清差异代谢物及代谢通路[J]. 北京大学学报(医学版), 2025, 57(6): 1042-1050. |
| [8] | 赵亚云, 倪梦凡, 李雪, 王蓓, 程功, 何菁, 金月波. 利妥昔单抗治疗原发性干燥综合征肾损害的临床疗效和安全性[J]. 北京大学学报(医学版), 2025, 57(6): 1051-1060. |
| [9] | 王翠萍, 陈哲, 程永静. 超微血流成像评估与膝骨关节炎临床症状的关联研究[J]. 北京大学学报(医学版), 2025, 57(6): 1096-1100. |
| [10] | 朱丽秀, 陈仁利, 周素娟, 林烨, 汤一榕, 叶桢. 水通道蛋白5对干燥综合征大鼠TLR4/MyD88/NF-κB信号的影响[J]. 北京大学学报(医学版), 2025, 57(5): 875-883. |
| [11] | 刘伟, 郭稳, 过哲, 李春艳, 李云龙, 刘思奇, 张亮, 宋慧. 痛风患者放射学阴性骨侵蚀的相关危险因素[J]. 北京大学学报(医学版), 2025, 57(4): 735-739. |
| [12] | 宁圆, 张晓盈, 李雪, 李原, 何菁, 金月波. 干燥综合征并发乳腺淋巴瘤1例[J]. 北京大学学报(医学版), 2025, 57(4): 808-811. |
| [13] | 杨源源, 张珊珊, 俞光岩, 杨辉俊, 杨宏宇. 部分下颌下腺切除术治疗下颌下腺良性肿瘤的临床效果[J]. 北京大学学报(医学版), 2025, 57(2): 334-339. |
| [14] | 朱灵丽, 唐琳, 李博文, 王梅, 刘玉华. 两种玷污层去除方法对牙本质表面性能的影响[J]. 北京大学学报(医学版), 2025, 57(2): 340-346. |
| [15] | 原晋芳, 王新利, 崔蕴璞, 王雪梅. 尿促黄体生成素在女童中枢性性早熟预测中的应用[J]. 北京大学学报(医学版), 2024, 56(5): 788-793. |
|
||
