北京大学学报(医学版) ›› 2023, Vol. 55 ›› Issue (5): 812-817. doi: 10.19723/j.issn.1671-167X.2023.05.006
靶向穿刺+6针系统穿刺对PI-RADS 5分患者的前列腺癌诊断效能
刘毅1,袁昌巍1,吴静云2,沈棋1,肖江喜2,*( ),赵峥1,*(),王霄英2,李学松1,何志嵩1,周利群1
),赵峥1,*(),王霄英2,李学松1,何志嵩1,周利群1
- 1. 北京大学第一医院泌尿外科, 北京大学泌尿外科研究所, 国家泌尿男生殖系肿瘤中心, 北京 100034
2. 北京大学第一医院医学影像科, 北京 100034
Diagnostic efficacy of prostate cancer using targeted biopsy with 6-core systematic biopsy for patients with PI-RADS 5
Yi LIU1,Chang-wei YUAN1,Jing-yun WU2,Qi SHEN1,Jiang-xi XIAO2,*(),Zheng ZHAO1,*(),Xiao-ying WANG2,Xue-song LI1,Zhi-song HE1,Li-qun ZHOU1
- 1. Department of Urology, Peking University First Hospital; Institute of Urology, Peking University; National Urological Cancer Center, Beijing 100034, China
2. Department of Radiology, Peking University First Hospital, Beijing 100034, China
摘要:
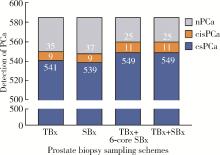
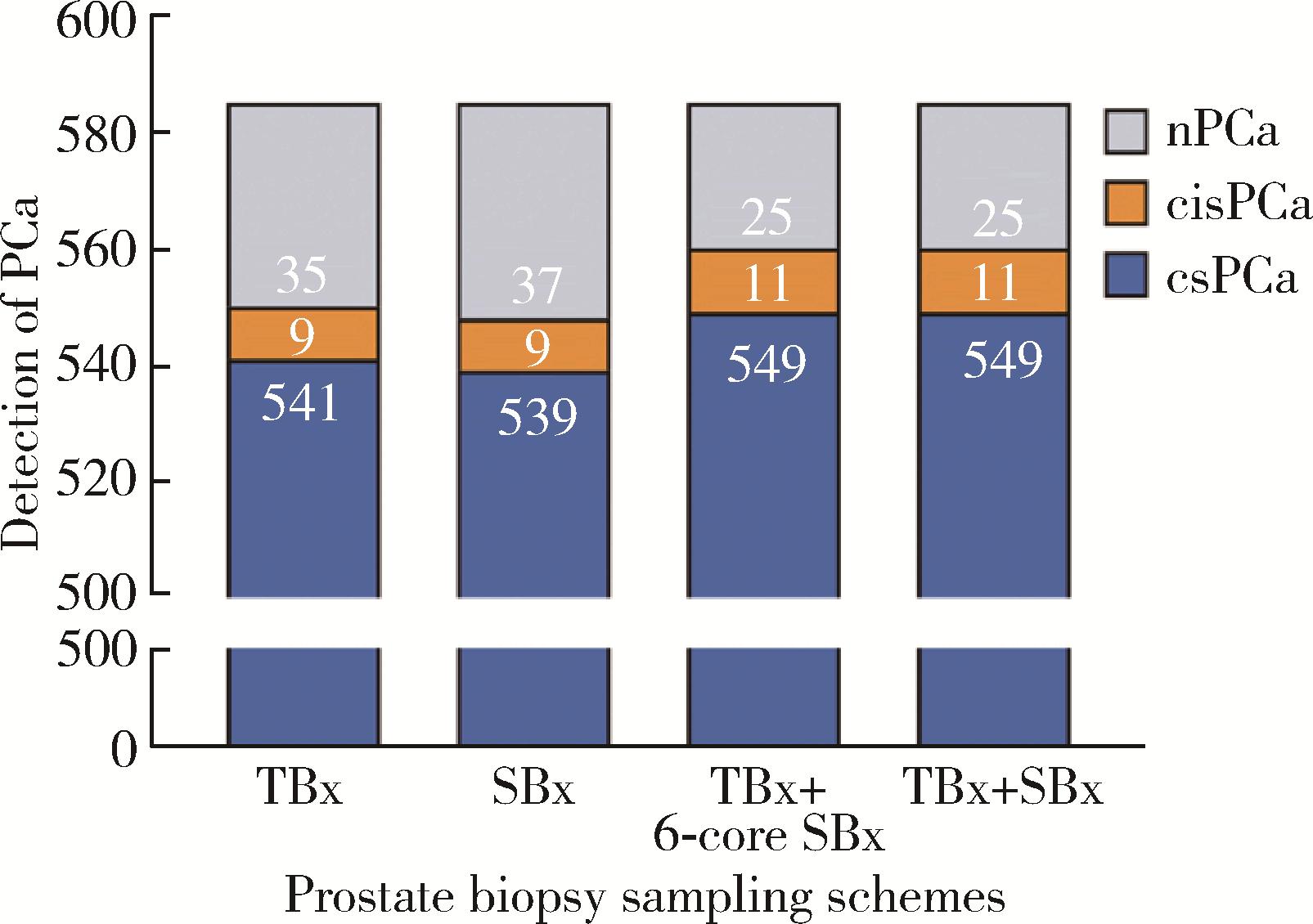
目的: 比较前列腺靶向穿刺、系统穿刺、靶向穿刺+6针系统穿刺活检对前列腺影像报告和数据系统(prostate imaging reporting and data system,PI-RADS)5分患者的前列腺癌(prostate cancer,PCa)及临床有意义前列腺癌(clinically significant prostate cancer,csPCa)的诊断效能,以优化前列腺穿刺方案。方法: 回顾性分析2019年1月至2022年6月北京大学第一医院多参数磁共振(multiparametric magnetic resonance imaging,mpMRI)检查PI-RADS评分5分且行前列腺穿刺活检的患者资料。所有患者在mpMRI/经直肠超声(transrectal ultrasound,TRUS)认知融合引导下,行联合穿刺活检(靶向穿刺联合系统穿刺)。以联合穿刺活检病理结果作为金标准,对比靶向穿刺、系统穿刺及靶向穿刺+6针系统穿刺对PCa和csPCa的诊断效能。按mpMRI T分期(cT2,cT3,cT4)进行分组,通过McNemar及Cochran’s Q检验比较不同穿刺方案对PCa和csPCa的检出情况。结果: 入组585例患者,联合穿刺阳性560例(95.7%),阴性25例(4.3%)。mpMRI T分期cT2期233例(39.8%),cT3期214例(36.6%),cT4期138例(23.6%)。按临床T分期分层后发现,cT2、cT3、cT4亚组中靶向穿刺与联合穿刺对PCa、csPCa检出率差异无统计学意义(PCa:P=0.203、P=0.250、P>0.999;csPCa:P=0.700、P=0.250、P>0.999),靶向穿刺+6针系统穿刺与联合穿刺对PCa、csPCa检出率差异亦无统计学意义(P均>0.999)。系统穿刺PCa和csPCa漏诊率分别为2.1%(12/560)和1.8%(10/549),靶向穿刺分别为1.8%(10/560)和1.4%(8/549),而靶向穿刺+6针系统穿刺检出了所有的PCa和csPCa。但与联合穿刺相比,靶向穿刺和靶向穿刺+6针系统穿刺的平均穿刺针数更少(P<0.001),单针阳性率更高(P<0.001)。结论: 对于PI-RADS 5分患者,靶向穿刺及靶向穿刺+6针系统穿刺有较高的单针阳性率及PCa、csPCa检出率,可作为前列腺穿刺方案的选择之一。
中图分类号:
- R737.25


| 1 |
Culp MB , Soerjomataram I , Efstathiou JA , et al. Recent global patterns in prostate cancer incidence and mortality rates[J]. Eur Urol, 2020, 77 (1): 38- 52.
doi: 10.1016/j.eururo.2019.08.005 |
| 2 |
Shen WW , Cui LG , Ran WQ , et al. Targeted biopsy with reduced number of cores: Optimal sampling scheme in patients undergoing magnetic resonance imaging/transrectal ultrasound fusion prostate biopsy[J]. Ultrasound Med Biol, 2020, 46 (5): 1197- 1207.
doi: 10.1016/j.ultrasmedbio.2020.01.017 |
| 3 |
Raman AG , Sarma KV , Raman SS , et al. Optimizing spatial biopsy sampling for the detection of prostate cancer[J]. J Urol, 2021, 206 (3): 595- 603.
doi: 10.1097/JU.0000000000001832 |
| 4 |
Barkovich EJ , Shankar PR , Westphalen AC . A systematic review of the existing prostate imaging reporting and data system version 2 (PI-RADS v2) literature and subset meta-analysis of PI-RADSv2 categories stratified by Gleason scores[J]. AJR Am J Roentge-nol, 2019, 212 (4): 847- 854.
doi: 10.2214/AJR.18.20571 |
| 5 |
Stabile A , Giganti F , Kasivisvanathan V , et al. Factors influencing variability in the performance of multiparametric magnetic resonance imaging in detecting clinically significant prostate can-cer: A systematic literature review[J]. Eur Urol Oncol, 2020, 3 (2): 145- 167.
doi: 10.1016/j.euo.2020.02.005 |
| 6 |
Hansen NL , Barrett T , Lloyd T , et al. Optimising the number of cores for magnetic resonance imaging-guided targeted and systema-tic transperineal prostate biopsy[J]. BJU Int, 2020, 125 (2): 260- 269.
doi: 10.1111/bju.14865 |
| 7 | 涂祥, 熊性宇, 张驰宸, 等. 6针系统穿刺联合3针磁共振引导靶向穿刺对前列腺癌的检出效果[J]. 中华泌尿外科杂志, 2022, 43 (12): 914- 919. |
| 8 |
Aminsharifi A , Gupta RT , Tsivian E , et al. Reduced core targeted (RCT) biopsy: Combining multiparametric magnetic resonance imaging-transrectal ultrasound fusion targeted biopsy with laterally-directed sextant biopsies: An alternative template for prostate fusion biopsy[J]. Eur J Radiol, 2019, 110, 7- 13.
doi: 10.1016/j.ejrad.2018.11.006 |
| 9 |
Teraoka S , Honda M , Shimizu R , et al. Optimal number of systematic biopsy cores used in magnetic resonance imaging/transrectal ultrasound fusion targeted prostate biopsy[J]. Yonago Acta Med, 2021, 64 (3): 260- 268.
doi: 10.33160/yam.2021.08.004 |
| 10 |
Sigle A , Suarez-Ibarrola R , Benndorf M , et al. Individualized decision making in transperineal prostate biopsy: Should all men undergo an additional systematic biopsy?[J]. Cancers (Basel), 2022, 14 (21): 5230.
doi: 10.3390/cancers14215230 |
| [1] | 刘艳华, 陆敏, 赵旭阳, 张宽根, 武睿, 梅放, 戴志豪, 由江峰, 裴斐. 肿瘤转移抑制基因LASS2去磷酸化对液泡型ATP酶活性及前列腺癌侵袭性的影响[J]. 北京大学学报(医学版), 2025, 57(6): 1113-1123. |
| [2] | 杨小勇, 张帆, 马潞林, 刘承. 前列腺导管腺癌临床特征及腺外侵犯的影响因素[J]. 北京大学学报(医学版), 2025, 57(5): 956-960. |
| [3] | 宁家昕, 王浩然, 罗书航, 敬吉波, 王建业, 侯惠民, 刘明. 氧化应激相关基因与前列腺癌关系的多组学分析[J]. 北京大学学报(医学版), 2025, 57(4): 633-643. |
| [4] | 王泽远, 于栓宝, 郑浩轲, 陶金, 范雅峰, 张雪培. 基于临床特征和多参数MRI的前列腺癌盆腔淋巴结转移的术前预测模型[J]. 北京大学学报(医学版), 2025, 57(4): 684-691. |
| [5] | 孙建军, 马千权, 尹晓亮, 杨辰龙, 张嘉, 陈素华, 吴超, 谢京城, 韩芸峰, 林国中, 司雨, 杨军, 邬海博, 赵强. 任意维度重建磁共振对骶管囊肿进行精准分型对于指导微创手术和康复的意义[J]. 北京大学学报(医学版), 2025, 57(2): 303-308. |
| [6] | 李志存, 吴天俣, 梁磊, 范宇, 孟一森, 张骞. 穿刺活检单针阳性前列腺癌术后病理升级的危险因素分析及列线图模型构建[J]. 北京大学学报(医学版), 2024, 56(5): 896-901. |
| [7] | 邢念增,王明帅,杨飞亚,尹路,韩苏军. 前列腺免活检创新理念的临床实践及其应用前景[J]. 北京大学学报(医学版), 2024, 56(4): 565-566. |
| [8] | 田宇轩,阮明健,刘毅,李德润,吴静云,沈棋,范宇,金杰. 双参数MRI改良PI-RADS评分4分和5分病灶的最大径对临床有意义前列腺癌的预测效果[J]. 北京大学学报(医学版), 2024, 56(4): 567-574. |
| [9] | 姚凯烽,阮明健,李德润,田宇轩,陈宇珂,范宇,刘毅. 靶向穿刺联合区域系统穿刺对PI-RADS 4~5分患者的前列腺癌诊断效能[J]. 北京大学学报(医学版), 2024, 56(4): 575-581. |
| [10] | 欧俊永,倪坤明,马潞林,王国良,颜野,杨斌,李庚午,宋昊东,陆敏,叶剑飞,张树栋. 肌层浸润性膀胱癌合并中高危前列腺癌患者的预后因素[J]. 北京大学学报(医学版), 2024, 56(4): 582-588. |
| [11] | 薛蔚,董樑,钱宏阳,费笑晨. 前列腺癌新辅助治疗与辅助治疗的现状及进展[J]. 北京大学学报(医学版), 2023, 55(5): 775-780. |
| [12] | 毛海,张帆,张展奕,颜野,郝一昌,黄毅,马潞林,褚红玲,张树栋. 基于MRI前列腺腺体相关参数构建腹腔镜前列腺癌术后尿失禁的预测模型[J]. 北京大学学报(医学版), 2023, 55(5): 818-824. |
| [13] | 袁昌巍,李德润,李志华,刘毅,山刚志,李学松,周利群. 多参数磁共振成像中动态对比增强状态在诊断PI-RADS 4分前列腺癌中的应用[J]. 北京大学学报(医学版), 2023, 55(5): 838-842. |
| [14] | 田聪,刘军,杨波,乔佳佳,黄晓波,许清泉. 经皮肾镜取石术中异常肾盂黏膜活检结果分析[J]. 北京大学学报(医学版), 2023, 55(5): 948-952. |
| [15] | 刘颖,霍然,徐慧敏,王筝,王涛,袁慧书. 磁共振血管壁成像评估颈动脉中重度狭窄患者斑块特征与脑血流灌注的相关性[J]. 北京大学学报(医学版), 2023, 55(4): 646-651. |
|
||
