北京大学学报(医学版) ›› 2024, Vol. 56 ›› Issue (3): 441-447. doi: 10.19723/j.issn.1671-167X.2024.03.010
基于马尔科夫模型的社区人群启动降压药物治疗预防心血管病的策略比较
周恬静1,刘秋萍1,张明露1,刘晓非1,康佳丽1,沈鹏2,林鸿波2,唐迅1,3,*( ),高培1,3,4,*()
),高培1,3,4,*()
- 1. 北京大学公共卫生学院流行病与卫生统计学系,北京 100191
2. 宁波市鄞州区疾病预防控制中心,浙江宁波 315101
3. 重大疾病流行病学教育部重点实验室(北京大学),北京 100191
4. 北京大学临床研究所真实世界证据评价中心,北京 100191
Comparison of initiation of antihypertensive therapy strategies for primary prevention of cardiovascular diseases in Chinese population: A decision-analytic Markov modelling study
Tianjing ZHOU1,Qiuping LIU1,Minglu ZHANG1,Xiaofei LIU1,Jiali KANG1,Peng SHEN2,Hongbo LIN2,Xun TANG1,3,*(),Pei GAO1,3,4,*()
- 1. Department of Epidemiology and Biostatistics, Peking University School of Public Health, Beijing 100191, China
2. Yinzhou District Center for Disease Control and Prevention, Ningbo 315101, Zhejiang, China
3. Key Laboratory of Epidemiology of Major Diseases (Peking University), Ministry of Education, Beijing 100191, China
4. Center for Real-world Evidence Evaluation, Peking University Clinical Research Institute, Beijing 100191, China
摘要:
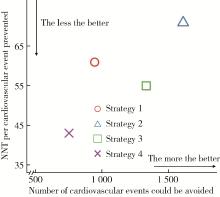
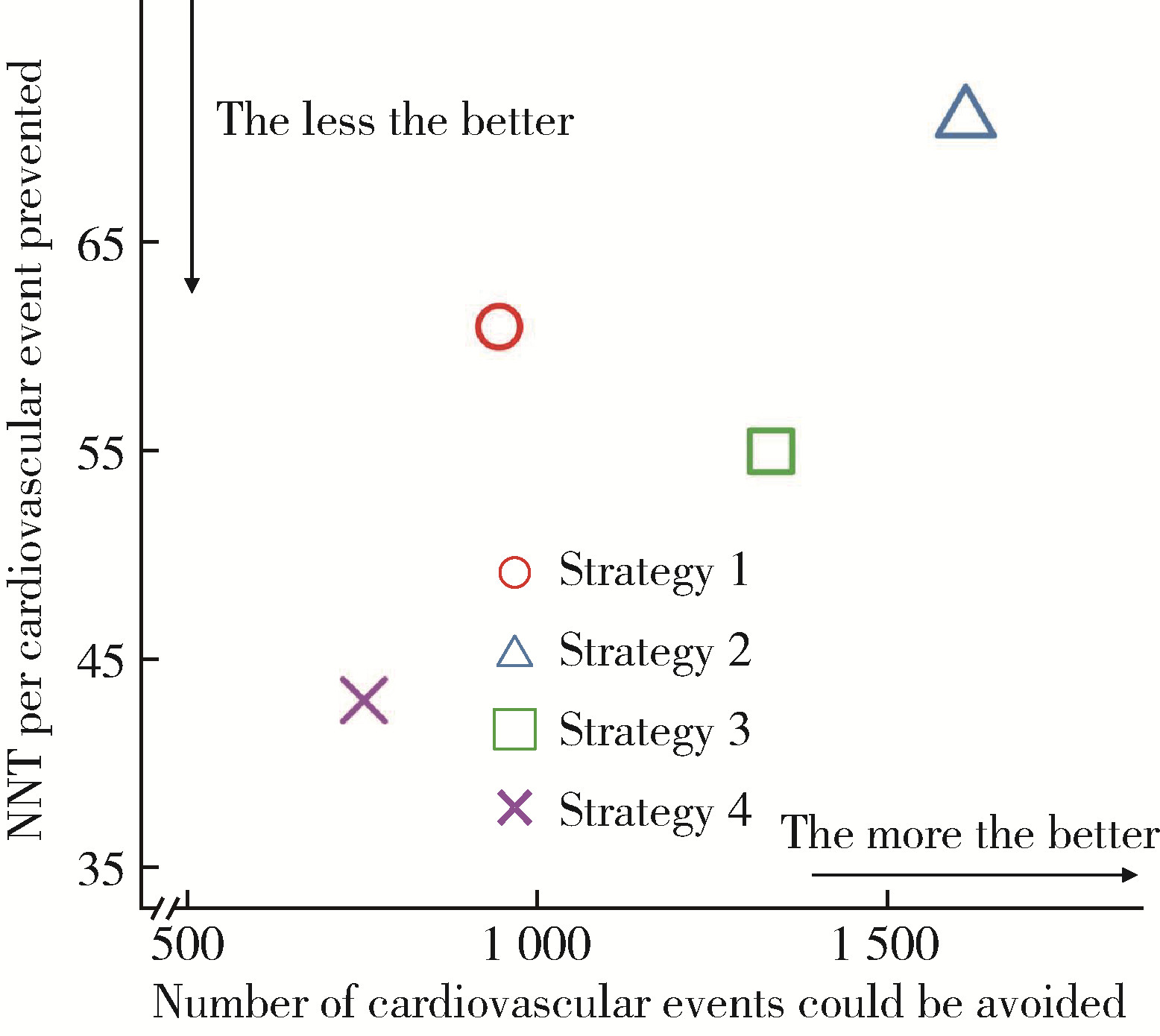
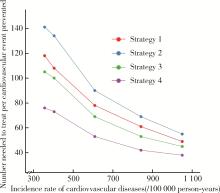
目的: 在中国鄞州电子健康档案研究(Chinese electronic health records research in Yinzhou, CHERRY)的队列人群中,评价启动降压药物治疗的不同策略预防心血管病的健康收益与干预效率。方法: 采用马尔科夫模型模拟评价的不同策略包括:策略1,对收缩压≥140 mmHg的人群启动降压药物治疗(根据2020年《中国心血管病一级预防指南》);策略2,对收缩压≥130 mmHg的人群启动降压药物治疗;策略3,对收缩压≥140 mmHg以及130~140 mmHg且心血管病高风险人群启动降压药物治疗(根据2017年美国心脏病学会/美国心脏协会《成年人高血压预防、检测、评估和管理指南》);策略4,对收缩压≥160 mmHg以及140~160 mmHg且心血管病高风险人群启动降压药物治疗(根据2019年英国国家卫生与临床优化研究所《成年人高血压诊断与管理指南》)。采用2019年世界卫生组织心血管病风险评估模型进行风险分层。马尔科夫模型的循环周期设为1年,模拟10个周期后计算质量调整生命年(quality-adjusted life year, QALY)、心血管病发病数、全因死亡数等结局事件数以评价策略的健康收益,并计算每预防一例心血管病事件或全因死亡的需治疗人数(number needed to treat, NNT)以评价策略的干预效率。马尔科夫模型的参数主要来源于CHERRY队列与公开发表的文献。采用单因素敏感性分析探讨心血管病发病率对结果的影响,采用概率敏感性分析探讨干预措施效应参数的不确定性对结果的影响。结果: 共纳入213 987名35~79岁基线无心血管病史的人群。相比于策略1,单纯下调降压起始值的策略2可预防的心血管病发病数增加666(95% UI: 334~975)例,但每预防一例心血管病发病的NNT增加10(95% UI: 7~20)人;而考虑定量风险评估的策略3可预防的心血管病发病数增加388(95% UI: 194~569)例,且每预防一例心血管病发病的NNT减少6(95% UI: 4~12)人,提示策略3可增加健康收益并具有更高的干预效率。策略4相比于策略1,可预防的心血管病发病数虽然减少193(95% UI: 98~281)例,但每预防一例心血管病事件的NNT减少18(95% UI: 13~37)人,效率更高。单因素敏感性分析及概率敏感性分析结果与主分析结果一致。结论: 在中国发达地区的社区人群中选择降压药物治疗目标人群时,结合心血管病定量风险评估的策略优于单纯将起始值从140 mmHg降至130 mmHg的策略,前者可提升健康收益且兼顾干预效率;不同地区需因地制宜选择降压起始值并结合定量风险评估的策略,以权衡健康收益与干预效率。
中图分类号:
- R54


| 1 |
Mensah GA , Fuster V , Murray CJL , et al. Global burden of cardiovascular diseases and risks, 1990—2022[J]. J Am Coll Cardiol, 2023, 82 (25): 2350- 2473.
doi: 10.1016/j.jacc.2023.11.007 |
| 2 |
胡大一, 韩雅玲, 宁光, 等. 中国心血管病一级预防指南[J]. 中华心血管病杂志, 2020, 48 (12): 1000- 1038.
doi: 10.3760/cma.j.cn112148-20201009-00796 |
| 3 |
Whelton PK , Carey RM , Aronow WS , et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: Executive summary: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines[J]. Hypertension, 2018, 71 (6): 1269- 1324.
doi: 10.1161/HYP.0000000000000066 |
| 4 | Boffa RJ , Constanti M , Floyd CN , et al. Hypertension in adults: Summary of updated NICE guidance[J]. BMJ, 2019, 367, l5310. |
| 5 |
Lu Y , Wang P , Zhou T , et al. Comparison of prevalence, awareness, treatment, and control of cardiovascular risk factors in China and the United States[J]. J Am Heart Assoc, 2018, 7 (3): e007462.
doi: 10.1161/JAHA.117.007462 |
| 6 |
Lin H , Tang X , Shen P , et al. Using big data to improve cardiovascular care and outcomes in China: A protocol for the Chinese electronic health records research in Yinzhou (CHERRY) study[J]. BMJ Open, 2018, 8 (2): e019698.
doi: 10.1136/bmjopen-2017-019698 |
| 7 |
WHO CVD Risk Chart Working Group . World Health Organization cardiovascular disease risk charts: Revised models to estimate risk in 21 global regions[J]. Lancet Glob Health, 2019, 7 (10): e1332- e1345.
doi: 10.1016/S2214-109X(19)30318-3 |
| 8 |
Wang JG , Staessen JA , Franklin SS , et al. Systolic and diastolic blood pressure lowering as determinants of cardiovascular outcome[J]. Hypertension, 2005, 45 (5): 907- 913.
doi: 10.1161/01.HYP.0000165020.14745.79 |
| 9 |
Herrett E , Gadd S , Jackson R , et al. Eligibility and subsequent burden of cardiovascular disease of four strategies for blood pressure-lowering treatment: A retrospective cohort study[J]. Lancet, 2019, 394 (10199): 663- 671.
doi: 10.1016/S0140-6736(19)31359-5 |
| 10 | 巩超, 刘秋萍, 王佳敏, 等. 社区人群他汀干预策略预防心血管病效果的马尔可夫模型评价[J]. 北京大学学报(医学版), 2022, 54 (3): 443- 449. |
| 11 |
Blood Pressure Lowering Treatment Trialists' Collaboration . Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: An individual participant-level data meta-analysis[J]. Lancet, 2021, 397 (10285): 1625- 1636.
doi: 10.1016/S0140-6736(21)00590-0 |
| 12 |
Wang M , Moran AE , Liu J , et al. Cost-effectiveness of optimal use of acute myocardial infarction treatments and impact on coronary heart disease mortality in China[J]. Circ Cardiovasc Qual Outcomes, 2014, 7 (1): 78- 85.
doi: 10.1161/CIRCOUTCOMES.113.000674 |
| 13 |
The China PEACE Collaborative Group . Association of age and blood pressure among 3.3 million adults: Insights from China PEACE million persons project[J]. J Hypertens, 2021, 39 (6): 1143- 1154.
doi: 10.1097/HJH.0000000000002793 |
| 14 |
Kim S , Chang Y , Kang J , et al. Relationship of the blood pressure categories, as defined by the ACC/AHA 2017 blood pressure guidelines, and the risk of development of cardiovascular disease in low-risk young adults: Insights from a retrospective cohort of young adults[J]. J Am Heart Assoc, 2019, 8 (11): e011946.
doi: 10.1161/JAHA.119.011946 |
| 15 |
Qi Y , Han X , Zhao D , et al. Long-term cardiovascular risk associated with stage 1 hypertension defined by the 2017 ACC/AHA hypertension guideline[J]. J Am Coll Cardiol, 2018, 72 (11): 1201- 1210.
doi: 10.1016/j.jacc.2018.06.056 |
| 16 |
Wang Z , Hao G , Wang X , et al. Clinical outcomes and economic impact of the 2017 ACC/AHA guidelines on hypertension in China[J]. J Clin Hypertens, 2019, 21 (8): 1212- 1220.
doi: 10.1111/jch.13609 |
| 17 |
Chen T , Yu D , Cornelius V , et al. Potential health impact and cost-effectiveness of drug therapy for prehypertension[J]. Int J Cardiol, 2017, 240, 403- 408.
doi: 10.1016/j.ijcard.2017.05.003 |
| 18 | Zhang M , Shi Y , Zhou B , et al. Prevalence, awareness, treatment, and control of hypertension in China, 2004-18: Findings from six rounds of a national survey[J]. BMJ, 2023, 380, e071952. |
| 19 | Li J , Zhao D , Cai J , et al. Cost-effectiveness of treatment in adults with blood pressure of 130-139/80-89 mmHg and high cardiovascular risk in China: A modelling study[J]. Lancet Reg Health West Pac, 2024, 42, 100962. |
| 20 |
Karmali KN , Lloyd-Jones DM , van der Leeuw J , et al. Blood pressure-lowering treatment strategies based on cardiovascular risk versus blood pressure: A meta-analysis of individual participant data[J]. PLoS Med, 2018, 15 (3): e1002538.
doi: 10.1371/journal.pmed.1002538 |
| 21 |
Zhou M , Wang H , Zeng X , et al. Mortality, morbidity, and risk factors in China and its provinces, 1990—2017: A systematic analysis for the global burden of disease study 2017[J]. Lancet, 2019, 394 (10204): 1145- 1158.
doi: 10.1016/S0140-6736(19)30427-1 |
| [1] | 陆梦溪, 王炳翰, 康佳丽, 刘秋萍, 周逸帆, 孙烨祥, 沈鹏, 林鸿波, 唐迅, 高培. 生物学年龄在社区人群队列中预测心血管病风险的应用[J]. 北京大学学报(医学版), 2026, 58(3): 543-550. |
| [2] | 陆梦溪, 刘秋萍, 周恬静, 刘晓非, 孙烨祥, 沈鹏, 林鸿波, 唐迅, 高培. 基于社区人群队列的甘油三酯-葡萄糖指数与心血管病发病和死亡的关联[J]. 北京大学学报(医学版), 2025, 57(3): 430-435. |
| [3] | 张明露,刘秋萍,巩超,王佳敏,周恬静,刘晓非,沈鹏,林鸿波,唐迅,高培. 阿司匹林用于心血管病一级预防的不同策略比较:一项马尔可夫模型研究[J]. 北京大学学报(医学版), 2023, 55(3): 480-487. |
| [4] | 张紫薇,花语蒙,刘爱萍. 中国中老年人群抑郁症状、缺血性心血管疾病10年风险对心血管疾病的联合影响[J]. 北京大学学报(医学版), 2023, 55(3): 465-470. |
| [5] | 王佳敏,刘秋萍,张明露,巩超,刘舒丹,陈暐烨,沈鹏,林鸿波,高培,唐迅. 基于马尔可夫模型的社区人群糖尿病筛查预防心血管病的效果评价[J]. 北京大学学报(医学版), 2022, 54(3): 450-457. |
| [6] | 巩超, 刘秋萍, 王佳敏, 刘晓非, 张明露, 杨瀚, 沈鹏, 林鸿波, 唐迅, 高培. 社区人群他汀干预策略预防心血管病效果的马尔可夫模型评价[J]. 北京大学学报(医学版), 2022, 54(3): 443-449. |
| [7] | 司亚琴,唐迅,张杜丹,何柳,曹洋,王晋伟,李娜,刘建江,高培,胡永华. 北方农村人群心血管病一级预防筛查策略的评价[J]. 北京大学学报(医学版), 2018, 50(3): 443-449. |
|
||
