北京大学学报(医学版) ›› 2024, Vol. 56 ›› Issue (5): 788-793. doi: 10.19723/j.issn.1671-167X.2024.05.006
尿促黄体生成素在女童中枢性性早熟预测中的应用
原晋芳, 王新利*( ), 崔蕴璞, 王雪梅
), 崔蕴璞, 王雪梅
- 北京大学第三医院儿科, 北京 100191
Application of urinary luteinizing hormone in the prediction of central precocious puberty in girls
Jinfang YUAN, Xinli WANG*(), Yunpu CUI, Xuemei WANG
- Department of Pediatrics, Peking University Third Hospital, Beijing 100191, China
摘要:
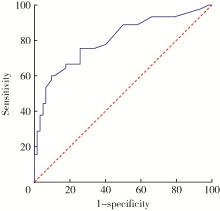
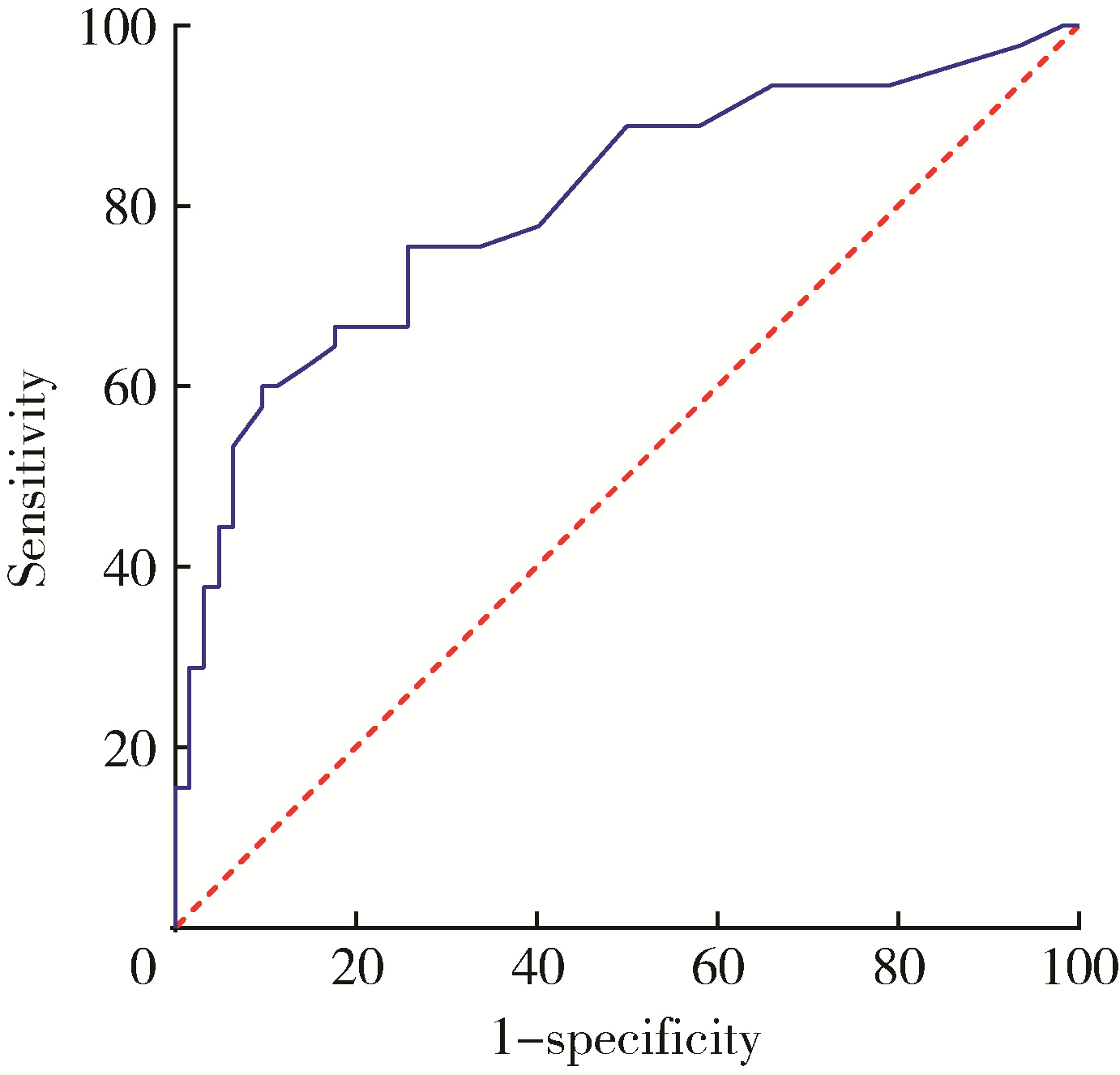
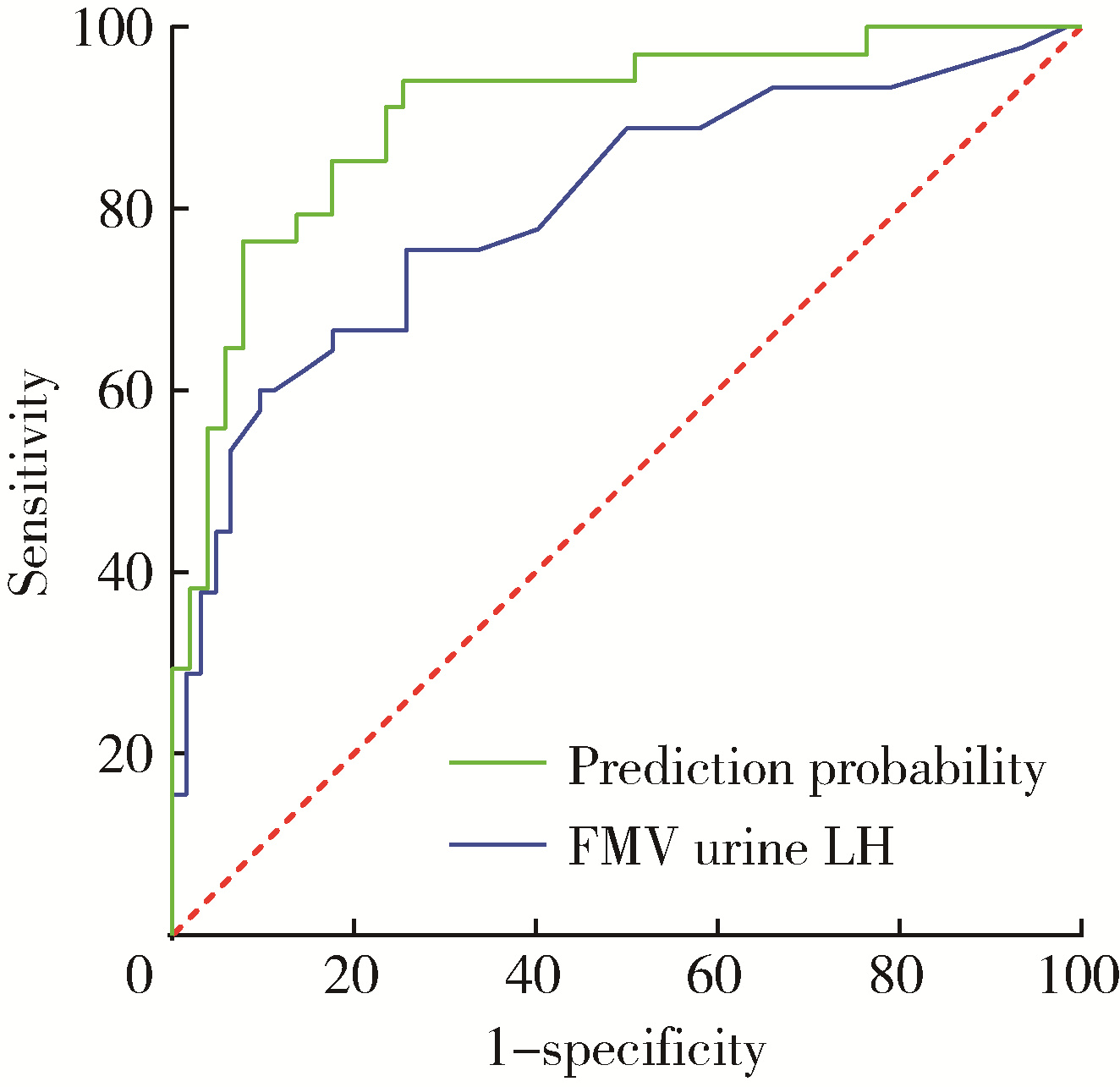
目的: 评估乳房发育女童晨尿促黄体生成素(luteinizing hormone,LH)水平,以确定晨尿LH对于评价中枢性性早熟(central precocious puberty,CPP)的价值。方法: 收集2018年9月至2021年4月期间因性早熟就诊于北京大学第三医院儿科门诊并住院行促性腺激素释放激素(gonadotropin-releasing hormone,GnRH)激发试验的女童共108例,根据CPP诊断标准分为CPP组(n=45)和非CPP组(n=63),比较两组的临床特征及激素水平,采用受试者工作特征(receiver operating characteristic,ROC)曲线分析得出尿LH的临床参考切割值。对尿LH水平与临床常用指标进行相关性分析,进一步评估尿LH在CPP诊断中的价值。结果: ROC曲线分析显示,晨尿LH水平对CPP诊断有意义,切割值为0.69 IU/L时,其敏感度为85%,特异度56.9%,曲线下面积为0.804(P < 0.001)。对GnRH激发试验前的基本临床特征进行二元Logistic回归分析,提示晨尿LH水平、子宫体积、卵巢体积、T骨龄提前程度对于诊断女童CPP均有预测意义(OR值分别为2.125、1.961、1.564、2.672),建立预测模型,ROC曲线下面积为0.904(P<0.001)。进一步行相关性分析,晨尿LH水平与GnRH激发试验前血激素水平(LH、FSH、雌激素)、GnRH激发试验后血LH峰值、T骨龄、子宫体积均呈正相关,r值分别为0.462、0.373、0.242、0.360、0.373和0.263,P值分别为 < 0.001、 < 0.001、0.013、 < 0.001、 < 0.001和0.007。结论: 晨尿LH水平对CPP的诊断有较好的提示意义,同时结合T骨龄提前程度及盆腔超声测量可进一步提高其对女童CPP诊断的预测价值。
中图分类号:
- R725.85


| 1 | 中华医学会儿科学分会内分泌遗传代谢学组, 中华儿科杂志编辑委员会. 中枢性性早熟诊断与治疗专家共识(2022)[J]. 中华儿科杂志, 2023, 61 (1): 16- 22. |
| 2 | Bradley SH , Lawrence N , Steele C , et al. Precocious puberty[J]. BMJ, 2020, 368, l6597. |
| 3 |
Latronico AC , Brito VN , Carel JC . Causes, diagnosis, and treatment of central precocious puberty[J]. Lancet Diabetes Endocrinol, 2016, 4 (3): 265- 274.
doi: 10.1016/S2213-8587(15)00380-0 |
| 4 |
Teilmann G , Pedersen CB , Jensen TK , et al. Prevalence and incidence of precocious pubertal development in Denmark: An epidemiologic study based on national registries[J]. Pediatrics, 2005, 116 (6): 1323- 1328.
doi: 10.1542/peds.2005-0012 |
| 5 | Demir A , Voutilainen R , Juul A , et al. Increase in first morning voided urinary luteinizing hormone levels precedes the physical onset of puberty[J]. J Clin Endocrinol Metab, 1996, 81 (8): 2963- 2967. |
| 6 |
中华医学会儿科学分会内分泌遗传代谢学组, 《中华儿科杂志》编辑委员会. 中枢性性早熟诊断与治疗共识(2015)[J]. 中华儿科杂志, 2015, 53 (6): 412- 418.
doi: 10.3760/cma.j.issn.0578-1310.2015.06.004 |
| 7 | Girard J , Hadziselimovic F . Relevance of urinary gonadotrophins[J]. Eur J Pediatr, 1987, 146 (Suppl 2)): S18- S20. |
| 8 |
Kulin HE , Santner SJ . Timed urinary gonadotropin measurements in normal infants, children, and adults, and in patients with disorders of sexual maturation[J]. J Pediatr, 1977, 90 (5): 760- 765.
doi: 10.1016/S0022-3476(77)81243-2 |
| 9 |
Wood CL , Lane LC , Cheetham T . Puberty: Normal physiology (brief overview)[J]. Best Pract Res Clin Endocrinol Metab, 2019, 33 (3): 101265.
doi: 10.1016/j.beem.2019.03.001 |
| 10 |
Abreu AP , Kaiser UB . Pubertal development and regulation[J]. Lancet Diabetes Endocrinol, 2016, 4 (3): 254- 264.
doi: 10.1016/S2213-8587(15)00418-0 |
| 11 |
Cantas-Orsdemir S , Eugster EA . Update on central precocious puberty: From etiologies to outcomes[J]. Expert Rev Endocrinol Metab, 2019, 14 (2): 123- 130.
doi: 10.1080/17446651.2019.1575726 |
| 12 |
Swerdloff RS , Odell WD . Hormonal mechanisms in the onset of puberty[J]. Postgrad Med J, 1975, 51 (594): 200- 208.
doi: 10.1136/pgmj.51.594.200 |
| 13 |
Apter D , Cacciatore B , Alfthan H , et al. Serum luteinizing hormone concentrations increase 100-fold in females from 7 years to adulthood, as measured by time-resolved immunofluorometric assay[J]. J Clin Endocrinol Metab, 1989, 68 (1): 53- 57.
doi: 10.1210/jcem-68-1-53 |
| 14 |
Rosenfield RL , Bordini B , Yu C . Comparison of detection of normal puberty in girls by a hormonal sleep test and a gonadotropin-releasing hormone agonist test[J]. J Clin Endocrinol Metab, 2013, 98 (4): 1591- 1601.
doi: 10.1210/jc.2012-4136 |
| 15 |
McNeilly JD , Mason A , Khanna S , et al. Urinary gonadotrophins: A useful non-invasive marker of activation of the hypothalamic pituitary-gonadal axis[J]. Int J Pediatr Endocrinol, 2012, 2012 (1): 10.
doi: 10.1186/1687-9856-2012-10 |
| 16 |
Kolby N , Busch AS , Aksglaede L , et al. Nocturnal urinary excretion of FSH and LH in children and adolescents with normal and early puberty[J]. J Clin Endocrinol Metab, 2017, 102 (10): 3830- 3838.
doi: 10.1210/jc.2017-01192 |
| 17 |
Demir A , Voutilainen R , Stenman UH , et al. First morning voided urinary gonadotropin measurements as an alternative to the GnRH test[J]. Horm Res Paediatr, 2016, 85 (5): 301- 308.
doi: 10.1159/000440955 |
| 18 |
Shim YS , An SH , Lee HJ , et al. Random urinary gonadotropins as a useful initial test for girls with central precocious puberty[J]. Endocr J, 2019, 66 (10): 891- 903.
doi: 10.1507/endocrj.EJ19-0071 |
| 19 |
Lee SY , Kim JM , Kim YM , et al. Single random measurement of urinary gonadotropin concentration for screening and monitoring of girls with central precocious puberty[J]. Ann Pediatr Endocrinol Metab, 2021, 26 (3): 178- 184.
doi: 10.6065/apem.2040208.104 |
| 20 |
Zung A , Burundukov E , Ulman M , et al. The diagnostic value of first-voided urinary LH compared with GnRH-stimulated gonadotropins in differentiating slowly progressive from rapidly progressive precocious puberty in girls[J]. Eur J Endocrinol, 2014, 170 (5): 749- 758.
doi: 10.1530/EJE-14-0010 |
| 21 |
Soriano-Guillen L , Argente J . Central precocious puberty, functional and tumor-related[J]. Best Pract Res Clin Endocrinol Metab, 2019, 33 (3): 101262.
doi: 10.1016/j.beem.2019.01.003 |
| 22 |
Xu YQ , Li GM , Li Y . Advanced bone age as an indicator facilitates the diagnosis of precocious puberty[J]. J Pediatr (Rio J), 2018, 94 (1): 69- 75.
doi: 10.1016/j.jped.2017.03.010 |
| 23 |
de Vries L , Horev G , Schwartz M , et al. Ultrasonographic and clinical parameters for early differentiation between precocious puberty and premature thelarche[J]. Eur J Endocrinol, 2006, 154 (6): 891- 898.
doi: 10.1530/eje.1.02151 |
| 24 |
Eksioglu AS , Yilmaz S , Cetinkaya S , et al. Value of pelvic sono-graphy in the diagnosis of various forms of precocious puberty in girls[J]. J Clin Ultrasound, 2013, 41 (2): 84- 93.
doi: 10.1002/jcu.22004 |
| 25 |
Lee SH , Joo EY , Lee JE , et al. The diagnostic value of pelvic ultrasound in girls with central precocious puberty[J]. Chonnam Med J, 2016, 52 (1): 70- 74.
doi: 10.4068/cmj.2016.52.1.70 |
| 26 |
Yuan B , Pi YL , Zhang YN , et al. A diagnostic model of idiopa-thic central precocious puberty based on transrectal pelvic ultrasound and basal gonadotropin levels[J]. J Int Med Res, 2020, 48 (8): 300060520935278.
doi: 10.1177/0300060520935278 |
| 27 |
Yu HK , Liu X , Chen JK , et al. Pelvic ultrasound in diagnosing and evaluating the efficacy of gonadotropin-releasing hormone agonist therapy in girls with idiopathic central precocious puberty[J]. Front Pharmacol, 2019, 10, 104.
doi: 10.3389/fphar.2019.00104 |
| [1] | 彭博, 刘芳芳, 杨伟, 徐瑞平, 陈蕾, 李保中, 王新家, 柯骥, 杨文蕾, 何煜, 刘震, 侯波林, 张利群, 林妙萍, 张立新, 张凡, 蔡奋, 许铧文, 刘萌飞, 刘英, 潘雅琪, 何忠虎, 柯杨. 围术期高血糖与食管切除术后食管鳞癌不良预后相关性[J]. 北京大学学报(医学版), 2026, 58(3): 567-574. |
| [2] | 袁思妍, 闵鹤葳, 陈平, 吴一波, 崔红霞, 张旭熙, 孙昕霙. 基于大五人格特质的2型糖尿病患者健康教育偏好[J]. 北京大学学报(医学版), 2026, 58(3): 600-605. |
| [3] | 温倩颖, 张丽卿, 秦安霖, 李小峰. 无症状高尿酸血症患者小肠细菌过度生长及炎症细胞因子表达水平[J]. 北京大学学报(医学版), 2026, 58(2): 313-318. |
| [4] | 郭睿霖, 张蕾, 王宇, 王晓庆, 王潇潇, 年凇汶, 张丽慧, 肖冰冰, 陆叶. 经闭孔尿道中段无张力悬吊改良术治疗女性压力性尿失禁的疗效[J]. 北京大学学报(医学版), 2026, 58(2): 337-341. |
| [5] | 闵鹤葳, 吴一波, 史宇晖, 李明子, 孙昕霙. 基于健康行动过程取向模型分析2型糖尿病患者膳食模式及血糖控制的影响因素[J]. 北京大学学报(医学版), 2025, 57(6): 1145-1152. |
| [6] | 顾静妍, 李欣艺, 赵金霞, 穆荣. 误诊为类风湿关节炎、痛风的糖尿病致Charcot关节病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1193-1197. |
| [7] | 曹沛, 栾庆先. 牙周炎与全身系统性疾病的思考与探索[J]. 北京大学学报(医学版), 2025, 57(5): 852-858. |
| [8] | 李慎谟, 苏丹丹, 林己煜, 宋昊东, 马潞林, 侯小飞, 王国良, 张洪宪, 叶剑飞, 张树栋. 腹腔镜下膀胱癌根治术同期行肾输尿管全长切除术的预后分析[J]. 北京大学学报(医学版), 2025, 57(5): 961-966. |
| [9] | 冷汶远, 高端, 李晓宇, 左炜, 胡伟民, 朱振鹏, 徐纯如, 林健, 李学松. 口腔黏膜补片与脱细胞真皮基质补片治疗长段尿道狭窄的疗效和安全性对比[J]. 北京大学学报(医学版), 2025, 57(5): 975-979. |
| [10] | 余霄腾, 黄奕瑄, 李新飞, 陈昶甫, 赵方舟, 应鸿刚, 陶子豪, 张一鸣, 徐丽清, 李志华, 杨昆霖, 周利群, 李学松, 赵峥. 结石相关输尿管狭窄的上尿路修复手术技术与临床结局[J]. 北京大学学报(医学版), 2025, 57(4): 670-675. |
| [11] | 冀竞辉, 林秀石, 潘大猛, 吴芝莹, 薛子璇, 田晓军, 张树栋, 王滨帅, 邱敏. 输尿管硬镜联合勺状阻石篮激光碎石术治疗输尿管1.5 cm及以上结石的效果[J]. 北京大学学报(医学版), 2025, 57(4): 676-683. |
| [12] | 缪祺, 洪保安, 张学舟, 孙志鹏, 王维, 王宇轩, 薄予轩, 赵佳晖, 张宁. 膀胱癌合并冠心病患者行经尿道膀胱肿瘤切除术围手术期抗血小板药物管理[J]. 北京大学学报(医学版), 2025, 57(4): 698-703. |
| [13] | 王起, 柯涵炜, 丁泽华, 张维宇, 张晓鹏, 徐涛, 许克新. 耻骨后与经闭孔尿道中段悬吊术对术后最大尿流率及残余尿量的影响[J]. 北京大学学报(医学版), 2025, 57(4): 717-720. |
| [14] | 刘世豪, 徐丽清, 李新飞, 杨昆霖, 李兆莹, 张子博, 王祥, 傅炜骁, 李志华, 李学松. 国产模块化手术机器人系统辅助肾盂成形术的可行性和安全性评价[J]. 北京大学学报(医学版), 2025, 57(4): 779-783. |
| [15] | 王焕瑞, 赖世聪, 胡浩浦, 丁泽华, 徐涛, 胡浩. 腹腔镜与输尿管软镜联合定位治疗复杂输尿管狭窄的疗效分析[J]. 北京大学学报(医学版), 2025, 57(4): 784-788. |
|
||
