北京大学学报(医学版) ›› 2026, Vol. 58 ›› Issue (2): 313-318. doi: 10.19723/j.issn.1671-167X.2026.02.014
无症状高尿酸血症患者小肠细菌过度生长及炎症细胞因子表达水平
温倩颖1,2, 张丽卿1,*( ), 秦安霖1, 李小峰3
), 秦安霖1, 李小峰3
- 1. 山西医科大学附属汾阳医院, 山西省汾阳医院风湿免疫科, 山西汾阳 032200
2. 临汾市妇幼保健院儿童医院, 山西临汾 041000
3. 山西医科大学第二医院风湿免疫科, 太原 030001
Small intestinal bacterial overgrowth and inflammatory factor expression levels in patients with asymptomatic hyperuricemia
Qianying WEN1,2, Liqing ZHANG1,*(), Anlin QIN1, Xiaofeng LI3
- 1. Department of Rheumatology and Immunology, Shanxi Fenyanq Hospital, Fenyang 032200, Shanxi, China
2. Linfen Maternal and Child Health Hospital Children's Hospital, Linfen 041000, Shanxi, China
3. Department of Rheumatology and lmmunology, Second Hospital of Shanxi Medical University, Taiyuan 030001, China
摘要:
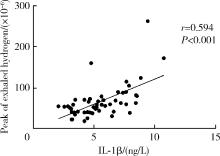
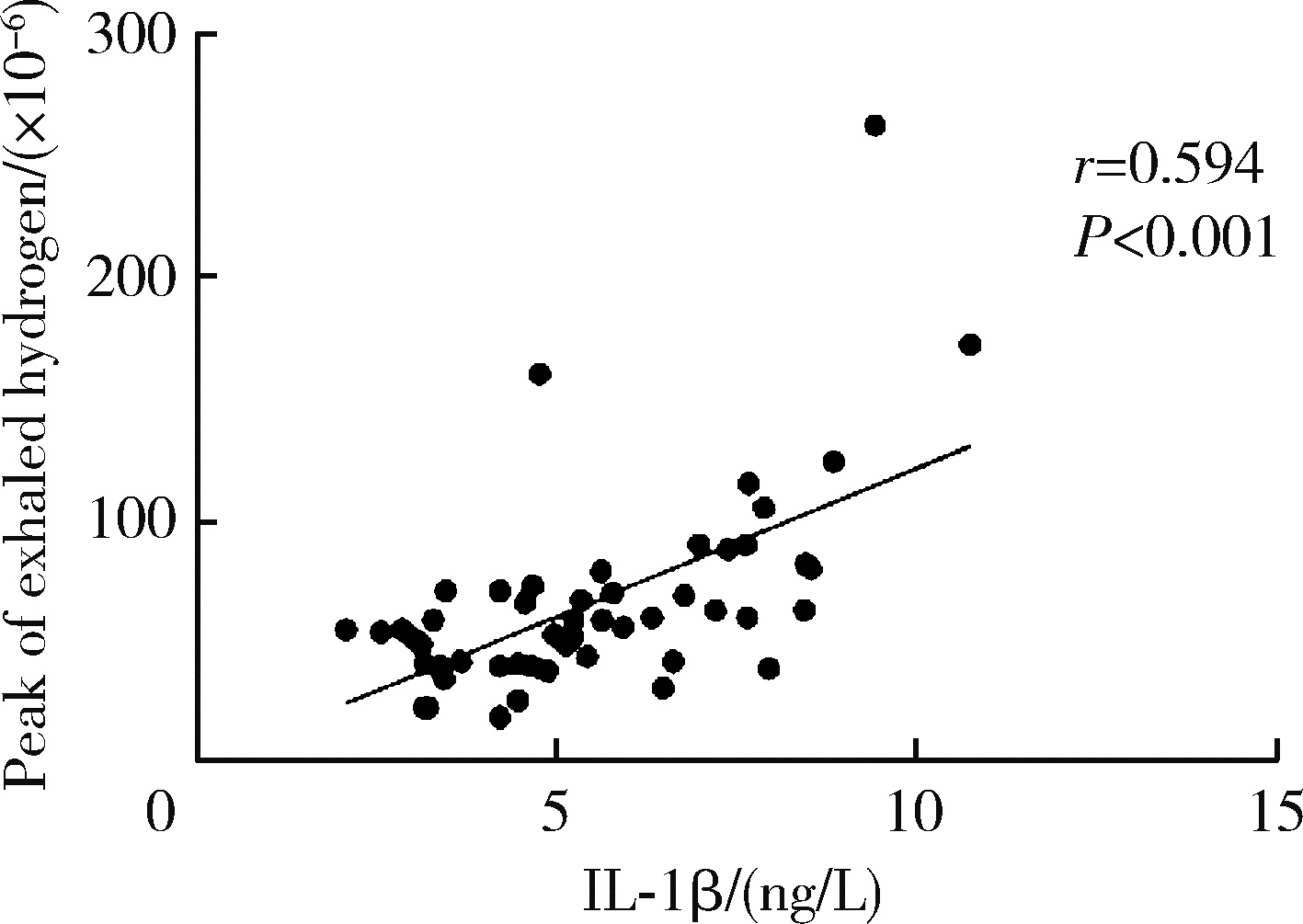
目的: 分析无症状高尿酸血症(hyperuricemia, HUA)患者小肠细菌过度生长(small intestinal bacterial overgrowth, SIBO)发生情况及无症状HUA合并SIBO患者血清中C-反应蛋白(C-reactive protein, CRP)、白细胞介素(interleukin, IL)-1β、IL-6和肿瘤坏死因子-α(tumor necrosis factor-α, TNF-α)表达水平。方法: 选取山西省汾阳医院2023年6月至2024年6月的87例无症状HUA患者和40例健康对照者为研究对象, 收集基线资料和实验室指标。采用乳果糖甲烷-氢呼气试验(lactulose methane-hydrogen breath test, LHBT)检测SIBO的发生情况, 并根据LHBT的检测结果将无症状HUA患者分为SIBO阳性组及SIBO阴性组, 分析无症状HUA患者SIBO阳性率, 比较无症状HUA患者与健康对照者各个时间点(0、30、60和90 min)H2和CH4浓度及CRP、IL-1β、IL-6、TNF-α水平, 以及SIBO阳性组和SIBO阴性组之间的CRP、IL-1β、IL-6、TNF-α水平。采用多因素Logistic回归分析无症状HUA患者发生SIBO的影响因素, 采用Spearman秩相关分析无症状HUA患者CRP、IL-1β、IL-6、TNF-α水平与SIBO的相关性。结果: 无症状HUA患者SIBO阳性率高于健康对照者, 差异有统计学意义(58.62% vs. 20.00%, χ2=16.431, P<0.001)。无症状HUA患者与健康对照者呼出H2浓度在各时间点差异均有统计学意义(P<0.05), 但呼出CH4浓度在各时间点差异均无统计学意义(P>0.05)。无症状HUA患者CRP、IL-1β、IL-6、TNF-α水平高于健康对照者, 差异有统计学意义(P<0.05)。无症状HUA患者SIBO阳性组血清CRP、IL-1β、IL-6水平均明显高于SIBO阴性组(P < 0.05), 但TNF-α水平在两组间差异无统计学意义(P>0.05)。多因素Logistic回归分析分析表明, IL-1β升高(OR=1.332, 95%CI: 1.005~1.764, P=0.046)、IL-6升高(OR=1.586, 95%CI: 1.216~2.069, P=0.001)是无症状HUA患者发生SIBO的独立危险因素。无症状HUA合并SIBO患者中, LHBT集值与血清IL-1β成正相关(r=0.594, P<0.001)。结论: 无症状HUA患者较健康人群更容易发生SIBO, 且SIBO的发生与炎症因子水平密切相关, 应重视无症状HUA患者SIBO的检测和干预。
中图分类号:
- R589
| 1 |
封番番, 张蓓, 周连锁, 等. 无症状高尿酸血症的诊治和管理[J]. 江苏医药, 2021, 47 (11): 1182- 1185.
|
| 2 |
doi: 10.3389/fpubh.2022.1008598 |
| 3 |
doi: 10.1080/00365521.2017.1342141 |
| 4 |
中华医学会内分泌学分会. 中国高尿酸血症与痛风诊疗指南(2019)[J]. 中华内分泌代谢杂志, 2020, 36 (1): 1- 13.
|
| 5 |
doi: 10.1038/ajg.2017.46 |
| 6 |
doi: 10.14309/ajg.0000000000000501 |
| 7 |
doi: 10.2174/1573397113666170425145405 |
| 8 |
doi: 10.3390/ijms232113450 |
| 9 |
doi: 10.1111/apt.15133 |
| 10 |
doi: 10.1007/s10620-020-06720-6 |
| 11 |
doi: 10.3349/ymj.2022.63.3.241 |
| 12 |
王帅, 左丽娟, 高扬, 等. 小肠细菌过度生长的治疗研究进展[J]. 临床消化病杂志, 2021, 33 (4): 303- 306.
|
| 13 |
doi: 10.1371/journal.pone.0234906 |
| 14 |
doi: 10.1016/j.tem.2018.02.006 |
| 15 |
doi: 10.1007/s10620-008-0315-x |
| 16 |
doi: 10.1371/journal.pntd.0012023 |
| 17 |
doi: 10.1080/0886022X.2022.2036620 |
| 18 |
doi: 10.1074/jbc.RA118.005197 |
| 19 |
doi: 10.1136/annrheumdis-2014-206564 |
| 20 |
doi: 10.3748/wjg.v20.i10.2482 |
| 21 |
阚美佳, 张尤历, 徐岷. 炎症性肠病与小肠细菌过度生长关系的荟萃分析[J]. 胃肠病学和肝病学杂志, 2019, 28 (11): 1256- 1261.
|
| 22 |
doi: 10.21037/apm-21-427 |
| 23 |
doi: 10.1111/nmo.12399 |
| [1] | 高嘉琪, 李文鹏, 李晓怡, 谭音希, 李奕昕, 段丽萍, 吴涛, 陈大方, 胡永华, 王梦莹. 基于可穿戴设备的老年人身体活动模式与肠道菌群的关联[J]. 北京大学学报(医学版), 2026, 58(3): 551-559. |
| [2] | 傅强,高冠英,徐雁,林卓华,孙由静,崔立刚. 无症状髋关节前上盂唇撕裂超声与磁共振检查的对比研究[J]. 北京大学学报(医学版), 2023, 55(4): 665-669. |
| [3] | 包文晗,唐雯. 初诊IgA肾病患者的肠道菌群及其与疾病进展因素的相关分析[J]. 北京大学学报(医学版), 2023, 55(1): 124-132. |
| [4] | 张家赫, 史佳琪, 陈章健, 贾光. 基于人消化道微生态体外模拟系统观察纳米二氧化钛对肠道菌群的影响[J]. 北京大学学报(医学版), 2022, 54(3): 468-476. |
| [5] | 王子靖,李在玲. 有幽门螺杆菌感染家族史儿童胃部菌群的特点[J]. 北京大学学报(医学版), 2021, 53(6): 1115-1121. |
| [6] | 张学武. 痛风关节炎治疗中几个备受关注的问题[J]. 北京大学学报(医学版), 2021, 53(6): 1017-1019. |
| [7] | 赵卫, 高辉, 朱佳鑫, 张学武, 栗占国. 血清Dickkopf-1与原发性痛风性关节炎骨破坏的相关性[J]. 北京大学学报(医学版), 2012, 44(2): 254-258. |
| [8] | 武丽君, 宋小芸, 库尔班江, 石亚妹, 黄慈波, 黄嘉, 刘爱华, 米克拉依, 滕玉芬, 古丽娜, 孟新艳, 单新洁, 木亚赛, 苑爱萍, 张莉. 新疆吐鲁番地区维吾尔族人群高尿酸血症和痛风的流行病学调查[J]. 北京大学学报(医学版), 2012, 44(2): 250-253. |
| [9] | 李丽君, 陈红, 任景怡, 王岚, 罗宇. 微粒化非诺贝特对高脂血症患者血脂及尿酸代谢的影响[J]. 北京大学学报(医学版), 2009, 41(5): 541-544. |
|
||
