Journal of Peking University (Health Sciences) ›› 2021, Vol. 53 ›› Issue (6): 1196-1200. doi: 10.19723/j.issn.1671-167X.2021.06.032
Previous Articles Next Articles
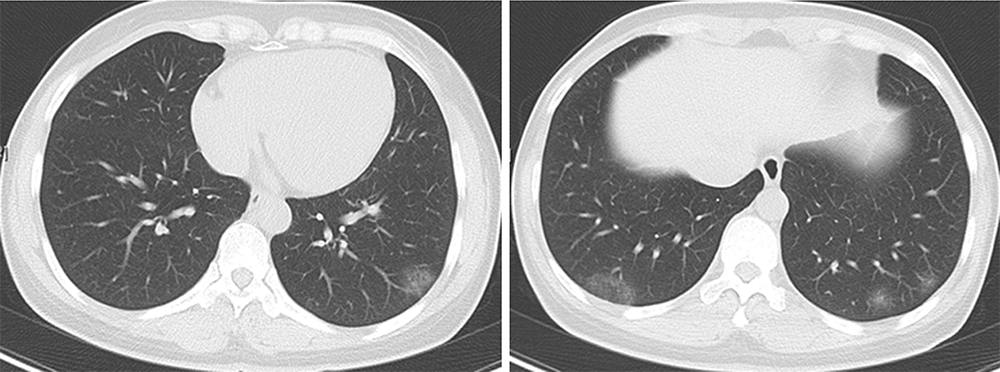
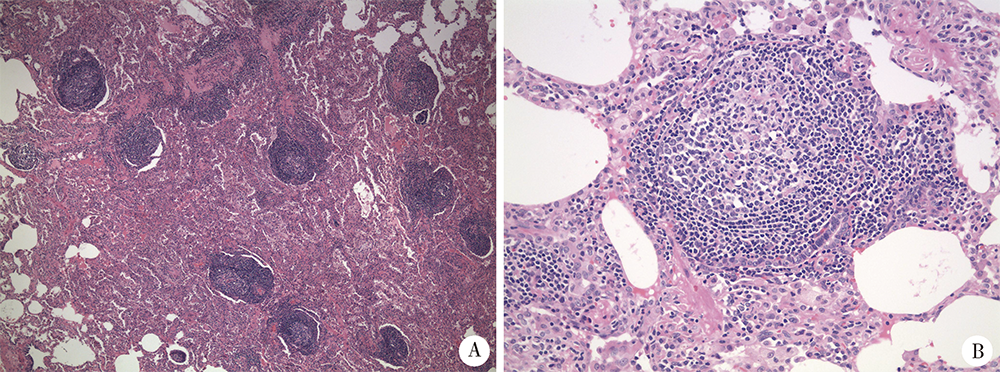
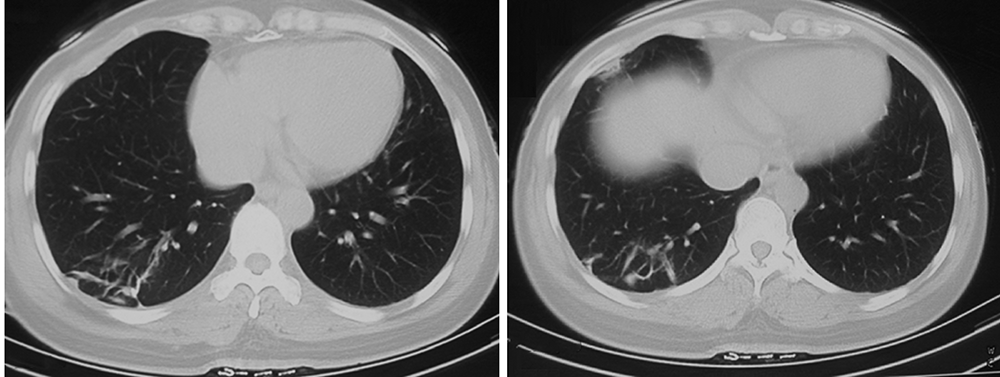
Spontaneous remission of follicular bronchiolitis with nonspecific interstitial pneumonia: A case report and literature review
WANG Fei1,ZHU Xiang2,HE Bei1,ZHU Hong1,SHEN Ning1,△( )
)
- 1. Department of Respiratory and Critical Care Medicine, Peking University Third Hospital, Beijing 100191, China
2. Department of Pathology, Peking University Third Hospital, Beijing 100191, China
CLC Number:
- R562.21


| [1] |
Romero S, Barroso E, Gil J, et al. Follicular bronchiolitis: Clinical and pathologic findings in six patients[J]. Lung, 2003, 181(6):309-319.
pmid: 14749935 |
| [2] |
Burgel PR, Bergeron A, de Blic J, et al. Small airways diseases, excluding asthma and COPD: An overview[J]. Eur Respir Rev, 2013, 22(128):131-147.
doi: 10.1183/09059180.00001313 |
| [3] | 方芳, 王芳, 张伟, 等. 肺活检表现为滤泡性细支气管炎的干燥综合征一例[J]. 中华结核和呼吸杂志, 2013, 36(3):229-230. |
| [4] | 戴建, 蔡后荣, 李燕, 等. 滤泡性细支气管炎三例并文献复习[J]. 中华结核和呼吸杂志, 2017, 40(6):457-462. |
| [5] |
Lu J, Ma M, Zhao Q, et al. The clinical characteristics and outcomes of follicular bronchiolitis in chinese adult patients[J]. Sci Rep, 2018, 8(1):7300.
doi: 10.1038/s41598-018-25670-8 |
| [6] |
Aerni MR, Vassallo R, Myers JL, et al. Follicular bronchiolitis in surgical lung biopsies: Clinical implications in 12 patients[J]. Respir Med, 2008, 102(2):307-312.
doi: 10.1016/j.rmed.2007.07.032 |
| [7] |
Exley CM, Suvarna SK, Matthews S. Follicular bronchiolitis as a presentation of HIV[J]. Clin Radiol, 2006, 61(8):710-713.
pmid: 16843757 |
| [8] | Mateos EA, Lópze FIA, Medel EB, et al. Follicular bronchiolitis. A review of 11 cases[J]. Virchows Arch, 2008, 452(Suppl 1):S56. |
| [9] |
Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 17-2001. A 42-year-old man with multiple pulmonary cysts and recurrent respiratory infections[J]. N Engl J Med, 2001, 344(22):1701-1708.
doi: 10.1056/NEJM200105313442208 |
| [10] |
Vos R, Vanaudenaerde BM, De Vleeschauwer SI, et al. Follicular bronchiolitis. A rare cause of bronchiolitis obliterans syndrome after lung transplantation: A case report[J]. Am J Transplant, 2009, 9(3):644-650.
doi: 10.1111/j.1600-6143.2008.02518.x pmid: 19191770 |
| [11] |
Shimizu K, Konno S, Nasuhara Y, et al. A case of follicular bronchiolitis associated with asthma, eosinophilia, and increased immunoglobulin E[J]. J Asthma, 2010, 47(10):1161-1164.
doi: 10.3109/02770903.2010.515326 |
| [12] |
Goksel O, Nart D, Ergonul AG, et al. Successful colchicine the-rapy in a patient with follicular bronchiolitis presumed to be asthma[J]. Respir Care, 2015, 60(7):e122-e124.
doi: 10.4187/respcare.03610 |
| [13] |
Roddy E, Summers G, Chaudry Z, et al. Follicular bronchiolitis, an unusual cause of haemoptysis in giant cell arteritis[J]. Clin Rheumatol, 2006, 25(3):433-435.
doi: 10.1007/s10067-005-0009-0 |
| [14] | Terada T. Follicular bronchiolitis and lymphocytic interstitial pneumonia in a Japanese man[J]. Diagn Pathol, 2011(6):85. |
| [15] |
Hwangbo Y, Cha SI, Lee YH, et al. A case of multicentric castleman’s disease presenting with follicular bronchiolitis[J]. Tuberc Respir Dis (Seoul), 2013, 74(1):23-27.
doi: 10.4046/trd.2013.74.1.23 |
| [16] | Wakamatsu K, Nagata N, Taguchi K, et al. A case of follicular bronchiolitis as the histological counterpart to nodular opacities in bronchiectatic mycobacterium avium complex disease[J]. Case Rep Pulmonol, 2012, 2012:214601. |
| [17] | Thalanayar PM, Holguin F. Follicular bronchiolitis in primary ciliary dyskinesia[J]. Australas Med J, 2014, 7(7):294-297. |
| [18] | 牟向东, 廖纪萍, 贺丹眉, 等. 滤泡性细支气管炎一例[J]. 呼吸与危重监护杂志, 2018, 17(1):86-87. |
| [19] |
Hare SS, Souza CA, Bain G, et al. The radiological spectrum of pulmonary lymphoproliferative disease[J]. Br J Radiol, 2012, 85(1015):848-864.
doi: 10.1259/bjr/16420165 pmid: 22745203 |
| [20] | 何慕芝, 蔡闯, 王继业, 等. 反晕征的病因谱及临床意义研究进展[J]. 国际呼吸杂志, 2018, 38(19):1516-1520. |
| [21] |
Tansey D, Wells AU, Colby TV, et al. Variations in histological patterns of interstitial pneumonia between connective tissue disorders and their relationship to prognosis[J]. Histopathology, 2004, 44(6):585-596.
pmid: 15186274 |
| [22] |
Travis WD, Hoffman GS, Leavitt RY, et al. Surgical pathology of the lung in Wegener’s granulomatosis: Review of 87 open lung biopsies from 67 patients[J]. Am J Surg Pathol, 1991, 15(4):315-333.
pmid: 2006712 |
| [23] | Tashtoush B, Okafor NC, Ramirez JF, et al. Follicular bronchiolitis: A literature review [J]. J Clin Diagn Res, 2015, 9(9): OE01-OE05. |
| [24] |
Bates CA, Ellison MC, Lynch DA, et al. Granulomatous-lymphocytic lung disease shortens survival in common variable immunodeficiency[J]. J Allergy Clin Immunol, 2004, 114(2):415-421.
doi: 10.1016/j.jaci.2004.05.057 |
| [1] | Bo PENG, Fangfang LIU, Wei YANG, Ruiping XU, Lei CHEN, Baozhong LI, Xinjia WANG, Ji KE, Wenlei YANG, Yu HE, Zhen LIU, Bolin HOU, Liqun ZHANG, Miaoping LIN, Lixin ZHANG, Fan ZHANG, Fen CAI, Huawen XU, Mengfei LIU, Ying LIU, Yaqi PAN, Zhonghu HE, Yang KE. Perioperative hyperglycemia predicts poorer prognosis of esophageal squamous cell carcinoma patients treated with esophagectomy [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 567-574. |
| [2] | Fan SHU, Liyuan GE, Hanzhang DENG, Haoming YIN, Junyong OU, Shaohui DENG, Yichang HAO, Min LU, Zhanyi ZHANG, Peichen DUAN, Shudong ZHANG. Molecular characteristics for poor prognosis related renal cell carcinoma with lymph metastases [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 631-640. |
| [3] | Youdong LIU, Yajun LYU, Jie CHEN, Mingde ZANG, Hongda PAN, Xiaowen LIU, Jun LU, Fenglin LIU. Clinical efficacy and safety of totally laparoscopic subtotal gastrectomy with cardia-gastric fundus preservation in middle-upper gastric cancer [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 301-306. |
| [4] | Weihao LI, Xuemin ZHANG, Wei LI, Tao ZHANG, Xiaoming ZHANG. Outcomes of suture-mediated vascular closure device in the closure of left brachial artery access site after thoracic endovascular aortic repair [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 388-392. |
| [5] | Ebrahimi Farin, Zhiqiang FENG, Ebrahimi Faraz, Weihua HAN, Ziyang YU, Kuankuan JIA, Jingang AN. Surgical treatment outcomes of different stages of maxillary medication-related osteonecrosis of the jaw [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 107-114. |
| [6] | Lingfu ZHANG, Ming CHEN, Xiaoyu ZHAO, Gang WANG, Long CUI, Xiaofeng LING, Lixin WANG, Zhi XU, Limei GUO, Chunsheng HOU. Gross classification of gallbladder cancer with primary lesion limited to the gallbladder wall and its correlation with prognosis and precancerous lesions [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 184-189. |
| [7] | Hailing ZANG, Yuhong LIANG. Endodontic retreatment of a maxillary second molar with chronic apical periodontitis and separated instrument: A case report [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 214-219. |
| [8] | Lianfei PAN, Wenjing LI, Ruiyang WANG, Jian JIAO, Zhanqiang CAO, Li GAO, Dong SHI. Short-term efficacy and influencing factors of systemic antibiotics as an adjunct to mechanical periodontal therapy for stages Ⅲ/Ⅳ periodontitis [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 30-36. |
| [9] | Jingyan GU, Xinyi LI, Jinxia ZHAO, Rong MU. Diabetic Charcot neuroarthropathy initially misdiagnosed as rheumatoid arthritis and gout: A case report [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1193-1197. |
| [10] | Shang XIE, Luming WANG, Xinyuan ZHANG, Qiushi FENG, Yangyang XIA, Ziwei DAI, Xiaofeng SHAN, Zhigang CAI. Construction and application of oral squamous cell carcinoma organoid bank [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 847-851. |
| [11] | Boda GUO, Min LU, Guoliang WANG, Hongxian ZHANG, Lei LIU, Xiaofei HOU, Lei ZHAO, Xiaojun TIAN, Shudong ZHANG. Clinicopathological and prognostic differences between clear cell and non-clear cell renal cell carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 644-649. |
| [12] | Weihao LI, Jing LI, Xuemin ZHANG, Wei LI, Qingle LI, Xiaoming ZHANG. Effect of intraoperative blood salvage autotransfusion on the prognosis of patients after carotid body tumor resection [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 272-276. |
| [13] | Yuanyuan YANG, Shanshan ZHANG, Guangyan YU, Huijun YANG, Hongyu YANG. Clinical outcomes of partial sialoadenectomy for the treatment of benign tumors in the submandibular gland [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 334-339. |
| [14] | Wenxin CHEN, Xiaomei HOU. Cyclic fatigue resistance of nickel-titanium files made by Gold heat treatment in simulated S-shaped root canals at different temperatures [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 136-141. |
| [15] | Jingqian LI, Zilu ZHU, Jian JIAO, Jie SHI. Clinical efficacy of clear aligner treatment for pathologically migrated teeth in the anterior region of patients with severe periodontitis [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 51-56. |
|
||